
Abstract
Objectives:
To assess resting-state functional connectivity and exploratory cognitive vulnerability in pediatric survivors of severe COVID-19 compared with healthy pre-pandemic controls.
Introduction:
Pediatric neurocognitive sequelae after SARS-CoV-2 infection remain poorly characterized.
Methods:
We conducted an observational case–control study including 14 children hospitalized for severe COVID-19 and 31 healthy pre-pandemic controls scanned on the same 3T MRI system using identical rs-fMRI protocols and a standardized CONN/SPM pipeline. ROI-to-ROI connectivity was analyzed with cluster-level FDR correction (P < .05).
Results:
Post-COVID participants showed 3 altered connectivity clusters: increased Default Mode–visual medial coupling, stronger dorsal attention–sensorimotor anticorrelations, and enhanced temporo-occipital–vermis connectivity. In an exploratory subset (8 post-COVID, 12 controls), 50% of post-COVID children had abnormally low Timeliness and 25% low Impulsivity MOXO-d-CPT z-scores, whereas no controls were abnormal.
Conclusion:
These preliminary findings suggest subtle post-infectious cognitive vulnerability and warrant confirmation in larger longitudinal cohorts.
Introduction
The first pediatric case of SARS-CoV-2 (COVID-19) was reported in Shenzhen, China, on January 20, 2020. 1 Contrary to initial expectations that children would be relatively spared, later evidence indicated that young children were at substantial risk of infection and may have developed systemic and neurological complications. 2 SARS-CoV-2 enters host cells via binding of its spike (S) protein to the membrane-bound angiotensin-converting enzyme 2 (ACE2) receptor on lung cells, facilitating endocytosis of the SARS-CoV-2-ACE2 complex. 3 As the COVID-19 pandemic advanced, neurological manifestations became increasingly documented, encompassing direct viral effects on the nervous system, immune-mediated para-infectious or post-infectious processes, and complications from systemic disease.4,5
Post-mortem analyses of adult brains revealed scant SARS-CoV-2 genetic material in neurons, suggesting minimal direct neuronal infection; however, traces were more frequently detected in astrocytes6,7—the glial cells that provide structural support to the central nervous system (CNS), regulate neuronal metabolism, and mediate immunological responses. This astrocyte involvement may have underlined reported neuropsychiatric symptoms. Morphological studies in adults with moderate infection identified cortical thinning in specific regions, correlated with symptoms such as fatigue, drowsiness, and impaired cognitive memory. 8 Brain imaging from the UK Biobank, comparing pre- and post-COVID-19 adults, disclosed significant cortical alterations, particularly in olfactory and gustatory regions, alongside changes in the parahippocampal gyrus—a structure critical for temporal event sequencing. 9
In adults, persistent cognitive symptoms after COVID-19—commonly described in the lay literature as “brain fog” 10 —include difficulties with concentration, drowsiness, forgetfulness, fatigue, and, in some cases, exacerbated depressive symptoms.6,10,11 This term is descriptive and does not correspond to a formally defined diagnostic entity. Nevertheless, it underscores growing concern that SARS-CoV-2 infection may have lasting effects on networks supporting attention, executive functions, and memory. Resting-state functional magnetic resonance imaging (rs-fMRI) provides a non-invasive approach to probe large-scale brain networks by quantifying temporal correlations in blood-oxygen-level-dependent (BOLD) signals between regions of interest (ROIs), including resting-state networks (RSNs).13 -15
Rs-fMRI studies in adults and older adolescents recovering from COVID-19 have reported mixed patterns of hyper and hypoconnectivity network alterations linked to subjective cognitive complaints and altered triple-network connectivity.16 -18 However, to our knowledge, no rs-fMRI studies have specifically characterized these network changes in pediatric survivors of severe COVID-19. Post-COVID cognitive difficulties during late childhood and early adolescence could be particularly consequential because this developmental window is critical for the maturation of prefrontal and parietal circuits that underlie sustained attention, working memory, and higher-order reasoning. At the same time, most pediatric reports rely on clinical observation, and systematic neuropsychological testing is rarely available; thus, neuroimaging markers may provide early objective clues, although they cannot substitute behavioral assessment.
This study, therefore, explores alterations in resting-state functional connectivity in pediatric survivors of severe COVID-19 hospitalization, comparing them with healthy pre-pandemic controls, to identify potential network-level substrates that may underlie post-infectious cognitive vulnerability.
Materials and Methods
Study Design and Participants
This observational cross-sectional case–control study included 14 pediatric survivors of severe COVID-19 (COV group) and 31 healthy controls (CoG group). All participants were previously healthy children without known neurological or psychiatric diagnoses (no comorbidities). The COV group comprised subjects hospitalized for SARS-CoV-2 infection between November and December 2021, consistent with the predominant circulation of the Delta variant in Mexico, who required admission due to respiratory insufficiency and had a positive reverse transcription polymerase chain reaction (RT-PCR) result from nasopharyngeal and/or oropharyngeal samples. MRI was performed at least 3 months after clinical recovery, once no overt COVID-19 symptoms were apparent. Subjects had no history of COVID-19 or SARS-CoV-2 vaccination.
The CoG group consisted of archival rs-fMRI data from 31 healthy children acquired before 2019 at the same institution, thereby ensuring no SARS-CoV-2 exposure at the time of imaging and providing a pre-pandemic baseline. Controls had no history of COVID-19 or SARS-CoV-2 vaccination and were free of neurological, psychiatric, or major systemic illness. Participants in both groups were matched for sex (all male) and showed comparable age distributions; age was non-normally distributed and therefore compared using the Mann–Whitney U test.
Exclusion criteria for both groups included claustrophobia, MRI-incompatible implants or dental hardware, history of autism spectrum disorder, obsessive–compulsive disorder, oppositional defiant disorder, neoplasms, or other brain injuries. The initial COVID-19 cohort comprised 26 children who met preliminary inclusion criteria; 12 were excluded due to comorbidities to minimize potential confounding, yielding the final COV sample of 14 participants (Figure 1). The sample size was determined by the number of eligible cases and available pre-pandemic controls; no a priori power calculation was performed, and this is acknowledged as a limitation of the study.

Flux diagram of the exclusion process of the COV group. This diagram shows the selection process of the COV group from the initial candidate list to the final 14-subject cohort.
Clinical and Cognitive Assessment (MOXO-d-CPT)
A subset of participants completed the MOXO d-Continuous Performance Test (MOXO-d-CPT), a computerized attention task that provides age-adjusted z-scores for 4 domains: Attention, Timeliness (processing speed), Impulsivity, and Hyperactivity. The test was administered after clinical recovery and around the time of MRI acquisition, in accordance with standardized procedures.
Complete MOXO-d-CPT data were available for 8 of the 14 children in the COV group; the remaining 6 did not complete the assessment due to logistic or scheduling constraints. For each domain, z-scores were interpreted according to the test manual; values around 0 indicate performance within the normative range, whereas larger negative scores reflect lower-than-expected performance. For descriptive purposes, abnormal performance was defined a priori as z-scores ≤ −1, indicating performance below age-matched norms. Proportions of children with abnormal scores were calculated separately for each group and domain; inferential statistics were not performed, given the small sample size, and these analyses are presented as exploratory behavioral correlates of the imaging findings.
Ethical Approval
The study was approved by the Ethics Committee of Hospital Infantil de México Federico Gómez (IBH code HIM-2025-001) and conducted in accordance with the Declaration of Helsinki and international ethical standards. 19 Written informed consent was obtained from all participants’ legal guardians, and assent was obtained from children when appropriate. Participants could withdraw at any time without consequences, and data were anonymized before analysis. Data were anonymized and deposited in a repository from which they will be available upon reasonable request to the corresponding author.
Experimental Protocol
Following informed consent, participants of the COV group attended a single morning session at the HIMFG. The protocol comprised patient preparation, anatomical imaging, and resting-state functional magnetic resonance imaging (rs-FMRI), lasting approximately 30 minutes in total. Upon completion of imaging, participation concluded. No structural abnormalities were identified on anatomical scans, confirming the eligibility of all recruited participants. All children cooperated fully, minimizing motion artifacts and enabling data acquisition without sedation.
MRI Acquisition
All MRI scans (COV and CoG) were acquired on the same 3T Siemens Skyra scanner (Siemens, Erlangen, Germany) with a 70 cm bore, equipped with a 32-channel head coil and stabilizing cushions to minimize head motion during scanning. The identical imaging protocol used for the CoG group was used for the COV group to avoid batch effects; no hardware or software upgrades occurred between the pre-2019 control acquisitions and the post-COVID scans, and all datasets were processed from raw images using the same pipeline.
Anatomical imaging consisted of 44 two-dimensional (2D) T1-weighted FLASH slices (repetition time [TR] 285 ms, echo time [TE] 2.49 ms, field of view [FOV] 250 × 250 mm, slice thickness 3.5 mm, matrix 320 × 320, in-plane resolution 0.78 × 0.78 mm), covering the whole brain, including the cerebellum in rostro-caudal orientation (acquisition time was 1 minute 29 seconds). Resting-state fMRI used a gradient-echo echo-planar imaging sequence with simultaneous multi-slice acceleration, 20 acquiring 240 volumes of 44 axial slices (TR 1500 ms, TE 30 ms, FOV 250 × 250 mm, slice thickness 3.5 mm, matrix 94 × 94, in-plane resolution 2.66 × 2.66 mm), also covering the whole brain and cerebellum (acquisition time 6 minutes 12 seconds).
During rs-fMRI, participants were instructed to remain still with their eyes open, fixate on a cross, and think of nothing in particular. No sedation was used; all children tolerated the procedure well, and structural images showed no gross abnormalities.
Image Processing
Image preprocessing and analyses followed previously published methodology.21 -23 Functional and anatomical images were preprocessed using the CONN functional connectivity toolbox (version 20.b) 24 in combination with SPM12 running in MATLAB (version 2021b). The same standard CONN resting-state pipeline 25 was applied to all participants. The first 16 volumes of each functional run were discarded to allow signal stabilization, after which images were realigned and unwarped 26 to correct for head motion and susceptibility–motion interactions.
Temporal misalignment between different slices of the functional data was corrected following SPM slice-timing correction (STC) procedure, 27 using sinc temporal interpolation to resample each slice BOLD timeseries to a common mid-acquisition time. Potential outlier scans were identified using ART28,29 as acquisitions with framewise displacement above 0.78 mm, 0.5° for rotation or global BOLD signal changes above 5 standard deviations,30,31 and a reference BOLD image was computed for each subject by averaging all scans excluding outliers.
Definition of Regions of Interest and Networks
Gray matter was parcellated according to the AAL atlas and assigned to canonical resting-state networks (RSNs) from the CONN library, generating region-of-interest (ROI) for both atlas regions and RSNs. Voxels within white matter and CSF masks were excluded from further analysis. Lastly, functional data were smoothed using spatial convolution with a Gaussian kernel of 8 mm full width at half maximum (FWHM) to meet parametric statistical assumptions.
For each subject, blood-oxygen-level-dependent (BOLD) time series were extracted by averaging the signal within each ALL ROI and each RSN region. Functional data were denoised using a confound regression pipeline incorporating established nuisance regressors. This included the removal of potential confounding effects derived from white matter (5 regressors), CSF (5 regressors), motion parameters and their first order derivatives (12 regressors), 34 outlier scans (<109 regressors), 29 session effects and their first order derivatives (2 regressors), and linear trends (2 regressors) within each functional run, followed by bandpass frequency filtering of the BOLD timeseries 35 between 0.008 and 0.09 Hz. CompCor regressors36,37 were estimated within each subject’s eroded white matter and CSF masks by extracting the mean signal and the largest principal components orthogonal to the mean signal, motion parameters, and outlier scans.
Functional Connectivity and Statistical Analysis
For functional data, a group-level analysis was performed using a General Linear Model (GLM 38 ). For each individual voxel a separate GLM was estimated, with first-level connectivity measures at this individual voxel a separate GLM was estimated, with first-level connectivity measures at this voxel as dependent variables (1 independent sample per subject and 1 measurement for the only condition of rest), and groups as subject-level identifiers as independent variables. The voxel-level hypothesis was evaluated using multivariate parametric statistics with random-effects across subjects and sample-covariance estimation across multiple measurements. Inferences were performed at the level of individual clusters (groups of continuous voxels). Cluster-level inferences were based on parametric statistics from Gaussian Random Field theory. 39 , 40 Results were thresholded using a combination of a cluster-forming P < .001 voxel-threshold, and a familywise corrected P-FDR < .05 cluster-size threshold (corresponding to Z = 3.89).
Results
Participants
The initial COVID-19 cohort comprised 26 children who met preliminary inclusion criteria; 12 were excluded due to comorbidities to reduce potential confounding, yielding a final COV sample of 14 previously healthy participants (Figure 1). The COV group comprised 14 participants, with a mean age of 10.38 years (standard deviation (SD) = 0.96 years, median = 10 years, interquartile range [IQR] 10-11 years, [min, max] = [9, 12] years), while the control group (CoG) included 31 children with a mean age of 10.06 years (SD = 0.44 years, median = 10 years, IQR 10-10years; [min., max.] = [9, 11] years). Subjects were paired by sex (all male), age distribution tested not normal via the Shapiro-Wilk test (COV: w = 0.874, P-value = .049; CoG: w = 0.643, P-value = .000), ages were then compared with a Mann-Whitney test (COV: u = 261, P-value = .216) showing no statistical differences between both cohorts. Descriptive demographic and clinical characteristics of both cohorts are presented in Table 1.
Clinical and Demographic description of participants.
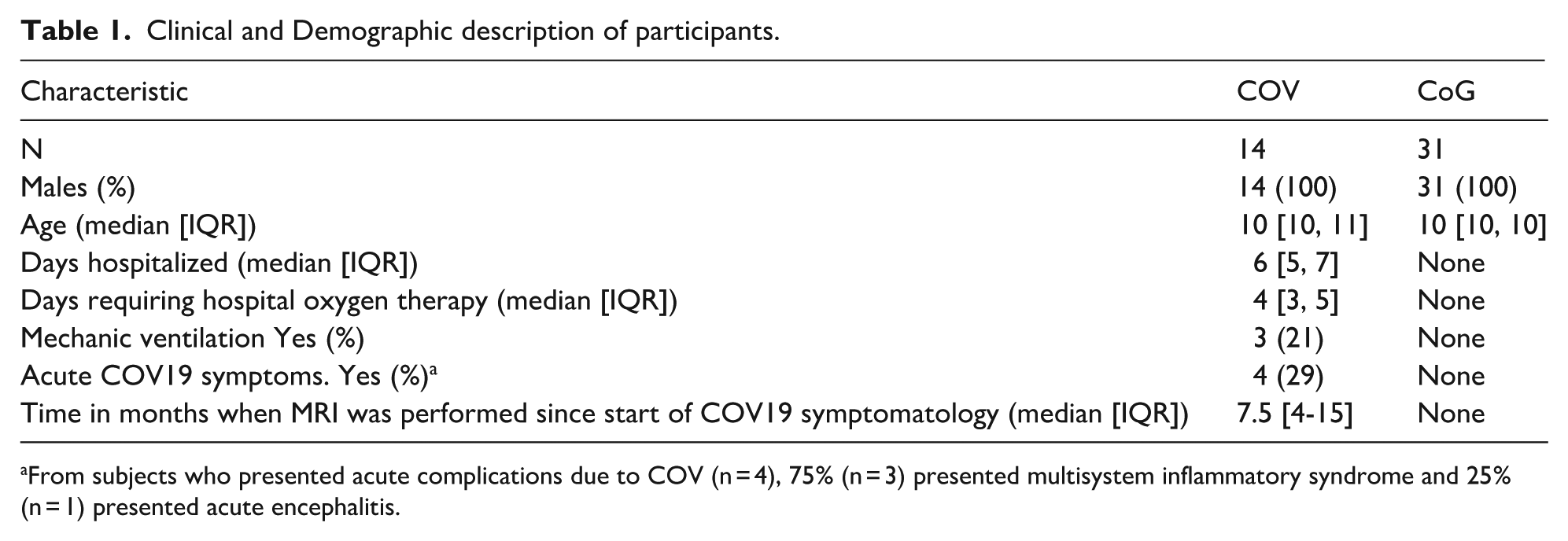
From subjects who presented acute complications due to COV (n = 4), 75% (n = 3) presented multisystem inflammatory syndrome and 25% (n = 1) presented acute encephalitis.
Resting-State Functional Connectivity
ROI-to-ROI analyses revealed significant differences in resting-state functional connectivity between the COV and CoG groups. Three connectivity clusters survived cluster-level false discovery rate correction (cluster-level P-FDR < .05) and showed robust connectivity (Fisher’s F (2,42) > 3.23) (Table 2, Figures 2–4).
Summary of the Statistical Results of COV Subjects Versus CoG.
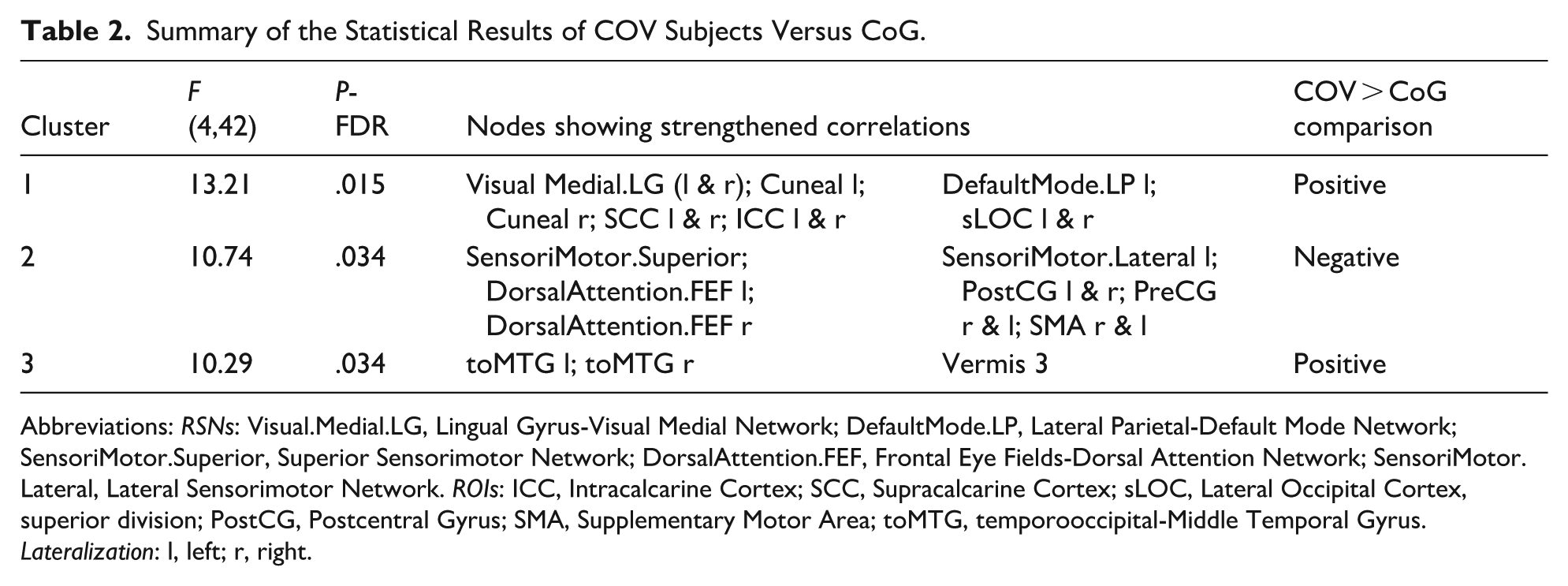
Abbreviations: RSNs: Visual.Medial.LG, Lingual Gyrus-Visual Medial Network; DefaultMode.LP, Lateral Parietal-Default Mode Network; SensoriMotor.Superior, Superior Sensorimotor Network; DorsalAttention.FEF, Frontal Eye Fields-Dorsal Attention Network; SensoriMotor.Lateral, Lateral Sensorimotor Network. ROIs: ICC, Intracalcarine Cortex; SCC, Supracalcarine Cortex; sLOC, Lateral Occipital Cortex, superior division; PostCG, Postcentral Gyrus; SMA, Supplementary Motor Area; toMTG, temporooccipital-Middle Temporal Gyrus. Lateralization: l, left; r, right.

Connectivity Matrix for COV versus CoG. This image shows the differences in FC displayed by the 2 groups. Warm colors (red scale) correspond to stronger positive FC for the COV versus CoG comparison of the ROIs and RSN tested. The cold colors (blue scale) correspond to anti-FC for the COV versus CoG comparison. Columns correspond to the same ROI distribution as in the rows (from left to right).

Connections projected on a glass brain for COV versus CoG. This image shows the anatomical positions of the ROIs in Figure 2, along with the links between them. Red color corresponds to stronger positive FC for the COV versus CoG comparison of the ROIs and RSN tested. Blue corresponds to anti-FC for the COV versus CoG comparison.
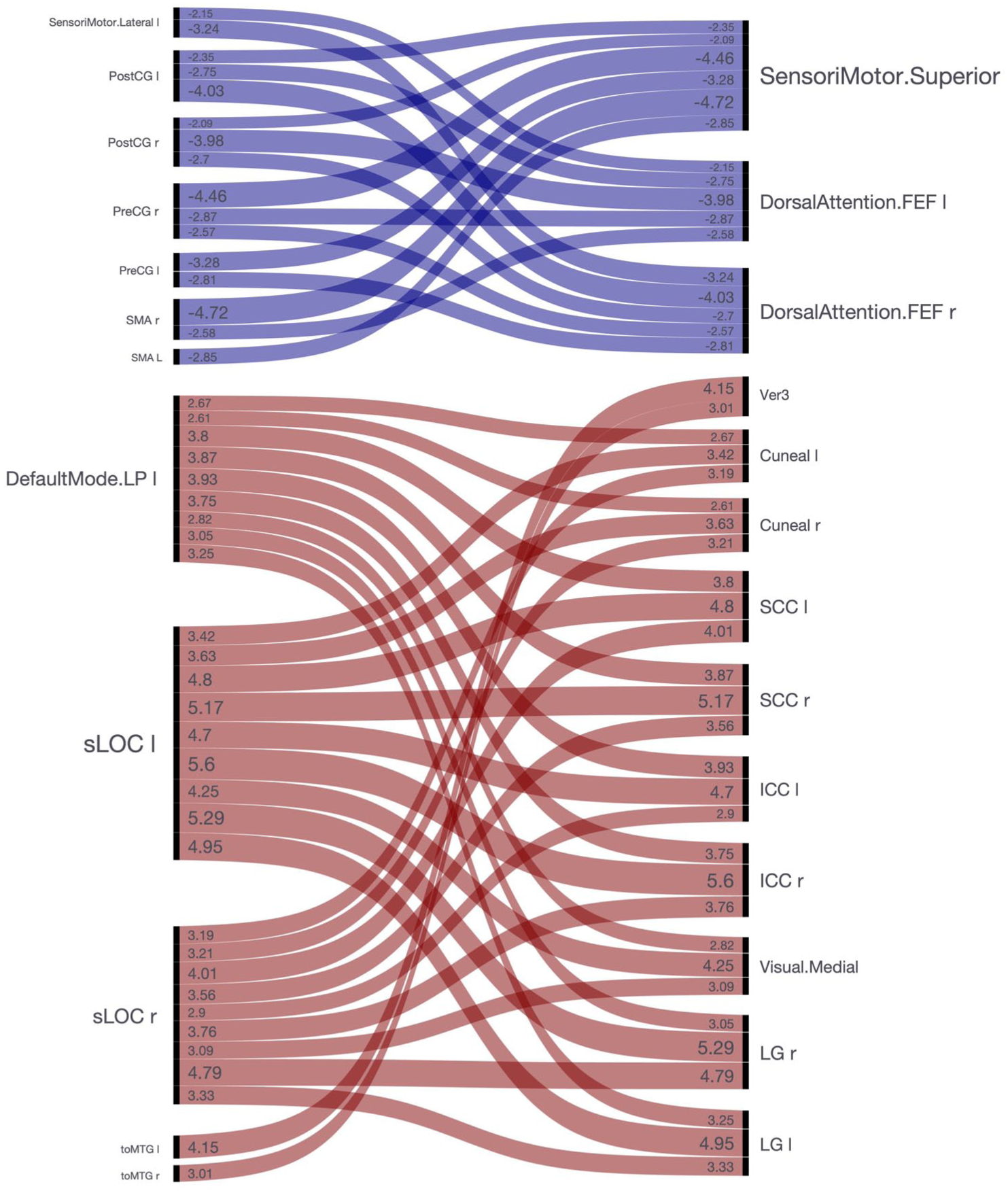
ROI to ROI connectivity diagram with connectivity estimated contrast magnitudes of each individual ROI analyzed. Cluster 1 involves significantly increased FC in the Default Mode Network (Warm colors; general Fisher’s F-score of 13.21; P-FDR = .015). Cluster 2 involves increased anticorrelated FC in the Sensorimotor Network (Cold colors; general F-score of 10.74; P-FDR = .034). Cluster 3 involves increased FC in nodes of the Vermis and the middle temporal gyrus (Warm colors; general F-score of 10.29; P-FDR = .034).
Cluster 1 (F (2,42) = 13.21; P-FDR = 0.015) comprised positive connectivity differences involving the Visual Medial network (lingual gyrus, intracalcarine and supracalcarine cortex bilaterally), the left Lateral Parietal node of the Default Mode Network, and bilateral superior lateral occipital cortex. In this cluster, children in the COV group showed stronger positive correlations between Default Mode and visual medial regions than controls.
Cluster 2 (F (2,42) = 10.74; P-FDR = .034) encompassed negative connectivity differences between dorsal attention and sensorimotor networks. Specifically, the COV group exhibited stronger anticorrelations between the frontal eye fields of the Dorsal Attention Network (left and right), the superior node of the Sensorimotor network, and the left Lateral Sensorimotor network, including precentral and postcentral gyri and supplementary motor areas.
Cluster 3 (F (2,42) = 10.29; P-FDR = .034) included positive connectivity differences between the temporo-occipital middle temporal gyrus (bilateral) and the vermis (Ver3), indicating increased coupling between temporo-occipital associative regions and cerebellar midline structures in the COV group.
Across clusters, connection-level T-statistics ranged from approximately 3.0 to 5.6, indicating robust group differences in resting state connectivity. The corresponding CONN effect-size plot reflects the estimated magnitude of the group-level connectivity contrast for each significant cluster (Figure 5). These network-level alterations suggest a configuration characterized by strengthened Default Mode–visual coupling together with enhanced anticorrelations between dorsal attention and sensorimotor systems in children who recovered from severe COVID-19.

Estimated effect sizes for significant resting-state connectivity clusters. The bars represent the estimated magnitude of the group-level connectivity contrast for each cluster in the CONN analysis. Connection-level T-statistics ranged from approximately 3.0 to 5.6, indicating robust group differences in resting-state connectivity.
MOXO-d-CPT Findings
Complete MOXO-d-CPT data were available for 8 of the 14 children in the COV group and for 12 of the healthy controls in the CoG group. In the control group, z-scores across the Attention, Timeliness, Impulsivity, and Hyperactivity domains clustered around 0, with no participant having a z-scores ≤ −1 in any domain (Figure 6).
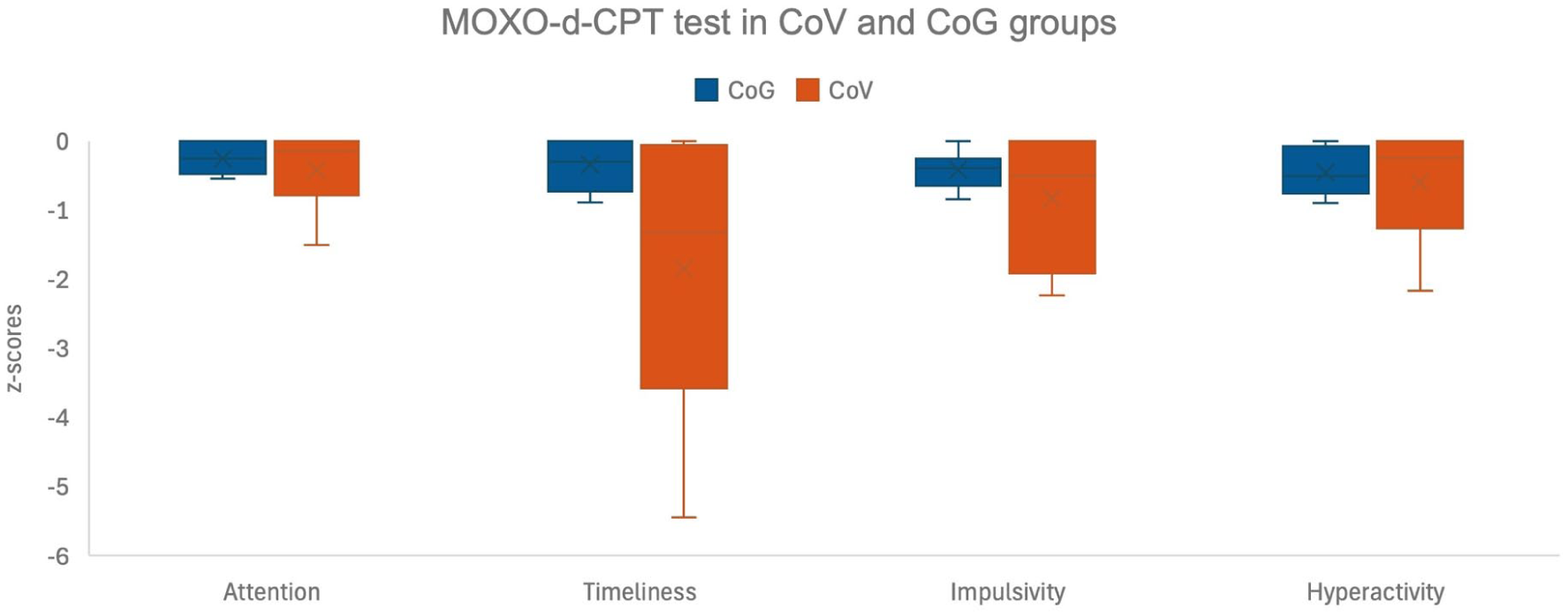
MOXO d-CPT test in COV (n = 8) and CoG (n = 12) groups. Although the sample is small, distinct descriptive patterns are observed in the z-scores for each group.
In contrast, among COV participants with available MOXO-d-CPT data, half (50%) had abnormally low Timeliness scores (z ≤ −1), indicating slower response speed relative to age-matched norms, and 25% had abnormally low Impulsivity scores at the same threshold. No COV participant exhibited abnormal Attention scores by this criterion, and 12.5% showed abnormal Hyperactivity scores. Although formal between-group statistical tests were not performed due to the small sample size, these descriptive patterns suggest that a subset of children recovering from severe COVID-19 may experience difficulties with processing speed and response control, whereas healthy controls in this sample did not show comparable abnormalities.
Given the limited sample size and incomplete MOXO-d-CPT data—particularly among children with more severe acute illness—these behavioral results should be considered exploratory and conservative estimates of the true cognitive burden. They are therefore interpreted as convergent, but preliminary, evidence consistent with the network-level alterations observed in dorsal attention and sensorimotor systems on rs-fMRI.
Discussion
The present study explored resting-state functional connectivity in pediatric survivors of severe COVID-19 compared with healthy pre-pandemic controls using a standardized rs-fMRI pipeline. Children in the post-COVID group showed increased coupling between Default Mode and visual medial regions, stronger anticorrelations between dorsal attention and sensorimotor networks, and enhanced connectivity between temporo-occipital and cerebellar vermis regions, organized into 3 statistically significant clusters. Exploratory MOXO-d-CPT data suggested that a subset of these children may experience difficulties in processing speed and response control, whereas healthy controls in this sample showed no abnormal test indices.
Interpretation of Network Alterations
The pattern of increased connectivity between the Default Mode Network (DMN) and visual medial regions, together with strengthened anticorrelations between dorsal attention and sensorimotor networks, points to a shift toward internally oriented processing at rest and reduced integration of attention and sensorimotor systems. Prior work has shown that efficient cognition requires dynamic interplay between DMN and task-positive networks such as the Dorsal Attention Network, with excessive DMN dominance or exaggerated anti-correlations being associated with attentional lapses and reduced cognitive flexibility. Within this framework, the present findings are compatible with a subtle vulnerability in sustaining attention and coordinating sensory–motor responses after severe pediatric COVID-19, although they do not by themselves demonstrate clinically significant impairment.
Connectivity increases between the temporo-occipital middle temporal gyrus and the cerebellar vermis may reflect compensatory reorganization or altered integration of visual–associative and cerebellar circuits. The cerebellum is increasingly recognized as contributing to cognitive and affective functions beyond motor control, and vermis involvement has been linked to processing speed and executive operations in other conditions. Together, the observed network configuration supports the hypothesis that SARS-CoV-2–related systemic and inflammatory processes can perturb large-scale functional networks in the developing brain without necessarily producing focal lesions.
Relation to Reported “Brain Fog” and Behavioral Data
In adults, persistent cognitive complaints after COVID-19—including difficulties with concentration, memory, and processing speed—are often described as “brain fog” in the lay literature and have been associated with alterations in DMN, salience, and attention networks on rs-fMRI. The term is descriptive and does not correspond to a formal diagnostic category, particularly in children, but it highlights concern about post-infectious cognitive vulnerability.
In this cohort, exploratory MOXO-d-CPT results provide preliminary behavioral support for this concern. Among children with available data, 50% of the COV group showed abnormally low Timeliness scores and 25% showed abnormally low Impulsivity scores (z ≤ −1), while no healthy control exhibited abnormal indices in these domains. These findings suggest that slowed processing speed and difficulties in response control may be present in a subset of pediatric survivors of severe COVID-19, consistent with the observed disruption of dorsal attention and sensorimotor networks. However, because MOXO-d-CPT data were available only for a fraction of the sample and more severely ill subjects were less likely to complete testing, these results likely underestimate the true cognitive burden and must be interpreted cautiously.
Overall, the convergence between rs-fMRI network alterations and exploratory MOXO-d-CPT findings supports the possibility of subtle post-COVID cognitive vulnerability in this pediatric population. Systematic, comprehensive neuropsychological assessment in larger samples will be essential to determine the prevalence, severity, and functional impact of these difficulties.
Methodological Considerations and Limitations
Several methodological aspects strengthen this study. First, the use of pre-2019 imaging data for the control group ensures that controls were unexposed to SARS-CoV-2 at the time of scanning and provides a robust pre-pandemic baseline. Second, all scans were acquired on the same 3T scanner using identical imaging protocols, with no intervening hardware or software upgrades, and processed from raw data using a single standardized CONN/SPM pipeline, which minimizes potential batch effects between groups. Third, rigorous motion control, artifact detection, and cluster-level FDR correction were applied, improving the reliability of the connectivity findings despite the modest sample size.
Important limitations must also be acknowledged. The sample size was relatively small and determined by the number of eligible cases and available pre-pandemic controls, and no a priori power calculation was performed; as a result, the study is best considered exploratory and underpowered to detect more subtle effects. The design is cross-sectional, precluding causal inferences about the temporal evolution of connectivity changes or their relation to pre-morbid functioning. Although acute complications such as multisystem inflammatory syndrome in children and encephalitis were recorded, the small sample prevented formal sensitivity analyses excluding these subgroups; such analyses are planned as future work and may help clarify the contribution of acute inflammatory conditions to the observed network changes.
In addition, detailed neuropsychological assessment was not available for all participants, and MOXO-d-CPT data were incomplete and biased toward less severely ill children, who were more likely to attend follow-up testing. Future studies with dedicated acquisition and data management protocols should address this gap. Finally, the present findings pertain to children hospitalized with severe COVID-19 and may not generalize to those with mild or asymptomatic infection.
Clinical and Research Implications
Despite these limitations, this study provides early evidence that pediatric survivors of severe COVID-19 can exhibit characteristic alterations in resting-state functional connectivity involving Default Mode, visual, dorsal attention, sensorimotor, and cerebellar networks, together with exploratory indications of slowed processing speed and impaired response control on MOXO-d-CPT in a subset of subjects. Clinically, these results support maintaining a high index of suspicion for subtle attention and processing-speed difficulties in children recovering from severe SARS-CoV-2 infection and underscore the importance of follow-up and access to neuropsychological evaluation when concerns arise.
From a research perspective, the findings highlight the need for longitudinal multimodal studies integrating rs-fMRI, structural imaging, detailed neuropsychological batteries, and inflammatory or immune markers in larger pediatric cohorts. Such work will be critical to determine whether the observed network alterations normalize, persist, or evolve over time, to quantify their impact on academic performance and daily functioning, and to identify children at greatest risk who may benefit from targeted interventions.
Conclusions
Pediatric survivors of severe COVID-19 in this study showed altered resting-state functional connectivity, characterized by increased coupling between Default Mode and visual medial networks and stronger anticorrelations between dorsal attention and sensorimotor systems, as well as enhanced connectivity between temporo-occipital and cerebellar vermis regions, compared with healthy pre-pandemic controls. Exploratory MOXO-d-CPT data suggested that a subset of these children may present slowed processing speed and difficulties in response control, whereas controls in this sample did not show comparable abnormalities.
Taken together, these imaging and behavioral findings are consistent with a subtle post-infectious cognitive vulnerability affecting attention-related and sensorimotor networks. Given the modest, convenience-based sample and incomplete neuropsychological data, the results should be viewed as preliminary and hypothesis-generating. Larger longitudinal studies integrating comprehensive neuropsychological assessments with multimodal neuroimaging are needed to confirm these observations, clarify their clinical significance, and guide follow-up and intervention strategies for children recovering from severe SARS-CoV-2 infection.
Summary Statement
Pediatric survivors of severe COVID-19 showed altered resting-state functional connectivity between Default Mode, visual, dorsal attention, sensorimotor networks, and cerebellar functional regions compared with healthy pre-pandemic controls, together with exploratory MOXO-d-CPT indications of slowed processing speed and impaired response control in a subset of subjects. These preliminary findings suggest a subtle post-infectious cognitive vulnerability and highlight the need for longitudinal multimodal studies with comprehensive neuropsychological assessment.
Key Results
Children who survived severe COVID-19 exhibited 3 significant clusters of altered resting-state functional connectivity, including increased coupling between Default Mode and visual medial networks, stronger anticorrelations between dorsal attention and sensorimotor networks, and enhanced connectivity between temporo-occipital regions and the cerebellar vermis, relative to healthy pre-pandemic controls. In an exploratory subset with MOXO-d-CPT data, 50% of post-COVID participants showed abnormally low Timeliness scores and 25% showed abnormally low Impulsivity scores, while no healthy controls displayed abnormal indices, suggesting possible vulnerabilities in processing speed and response control that warrant confirmation in larger longitudinal studies.
Footnotes
Acknowledgements
The authors gratefully acknowledge the valuable technical support of Jorge Olvera and Ricardo Sánchez. The authors also acknowledge the fellowship (No. 1098339) awarded by the Secretaría de Ciencias, Humanidades, Tecnología e Innovación (SECIHTI, formerly CONAHCYT) that supported Yunuen Rojas-Lemus’ doctoral studies.
ORCID iDs
Ethical Considerations
This study was approved by the Ethics Committee of Hospital Infantil de México Federico Gómez (IBH code HIM-2025-001) and conducted in accordance with the Declaration of Helsinki and with SAGE’s editorial policies on research ethics and integrity. All procedures complied with national and institutional regulations for research involving human participants and with international guidelines for pediatric imaging research.
Consent to Participate
Parents or legal guardians of all participants received written and verbal information about the study aims, procedures, potential risks, and benefits, and provided written informed consent before any research procedures were undertaken. Age-appropriate information was given to children, who were invited to assent according to their level of understanding, and their willingness to participate was respected. Participants were informed that they could withdraw from the study at any time without providing a reason and without affecting their medical care.
Consent for Publication
Images do not disclose any participant’s personal information.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All MRI data and clinical information were anonymized before analysis; personal identifiers were removed, and a study code was used in all datasets to protect confidentiality. Data were anonymized and deposited in a repository from which they will be available upon reasonable request to the corresponding author.*