
Abstract
Introduction
Anemia is a global public health concern. This study aimed to analyze the non-fatal health outcomes of dietary iron deficiency anemia in ESSA from 1990 to 2023.
Methods
Data from the Global Burden of Diseases 2023 study was used to estimate the non-fatal health outcomes of dietary iron deficiency anemia.
Results
In 2023, the age-standardized prevalence and YLD rate of dietary iron deficiency anemia were 26899 (95% UI: 23092, 31657), and 807 (95% UI: 488, 1357) in ESSA. The Prevalence and YLD rates were highest among children under five years, with females showing higher rates across nearly all age groups. From 1990 to 2023, the age-standardized rates remained unchanged throughout the region.
Conclusion
Dietary iron deficiency anemia remains a public health problem in the ESSA region since 1990.
Introduction
Anemia is a major public health concern, mainly affecting children and women of reproductive age. 1 In 2021, the prevalence of anemia was 1.92 billion worldwide, accounting for 5.7% of all years lived with disability (YLD) and ranking first among all impairments. 2 Dietary iron deficiency is the most common cause of anemia, especially in low-income countries.3-5
The inclusion of anemia in the Sustainable Development Goals of the United Nations prompted substantial and widespread policy actions. 6 Nutrition programs, such as iron supplementation for pregnant women and children and food fortification with iron-containing multiple micronutrient powders, were recommended by the World Health Organization. 7 However, there is a shortage of epidemiological studies that clarify the distribution of dietary iron deficiency anemia, particularly in resource-limited setting. 8 Although iron deficiency anemia is well documented, little is known about dietary involvement in symptomatic iron deficiency manifesting in medical conditions. Lack of comprehensive, comparable, and updated information may delay nutrition intervention outcomes.
Thus, this study aimed to: (1) estimate prevalence and YLDs due to dietary iron deficiency anemia by age, sex, and country in ESSA from 1990-2023; (2) examine trends over time; and (3) identify disparities to inform targeted interventions.
Methods
Study Setting
This study was conducted in the ESSA region, which included Eritrea, Ethiopia, Burundi, Comoros, Kenya, Madagascar, Malawi, Djibouti, Mozambique, Rwanda, Somalia, South Sudan, United Republic of Tanzania, Zambia, and Uganda. The ESSA region is experiencing a demographic boom, with the population expected to exceed one billion by 2050. A large percentage of the population is under the age of 15, and the median age is relatively low. While the region is still predominantly rural, it is experiencing significant urban growth, with a projected increase in urban population. 9 Conflict and climatic shocks, including floods and cyclones, have driven more than 87 million people into food insecurity in East and Southern Africa and the Middle East. 10
Data Sources
The GBD 2023 study’s input data were used to estimate the prevalence and YLDs (i.e., non-fatal health outcomes) due to dietary iron deficiency anemia in the ESSA region from 1990 to 2023. The GBD 2023 study provides a comprehensive assessment of the burden of diseases, injuries, and risk factors, including dietary causes of iron deficiency anemia. It utilizes a more extensive dataset and employs advanced analytical methods. Thus, it provides a more accurate and up-to-date assessment of non-fatal health outcomes related to dietary iron deficiency anemia, as it incorporates the latest research and data sources. This allows for a more precise comparison of health progress and the impact of various health factors over time. In GBD burden estimates, dietary iron deficiency anemia is treated as a cause of anemia resulting specifically from inadequate dietary iron intake that leads to clinically significant anemia (anemia defined by hemoglobin below WHO thresholds). 11 Other causes of iron deficiency (e.g., blood loss, or genetic disorders affecting iron metabolism and inflammation) are modeled separately in the GBD cause hierarchy. The methods of GBD 2023 have been detailed in earlier reports. 12 This GBD study provided estimates of unique, continuous distributions of hemoglobin concentrations (g/L) adjusted for elevation, with corresponding dietary iron deficiency anemia prevalence and YLD across different severity levels.11-13 YLDs for dietary iron deficiency anemia in the GBD Study are estimated by identifying prevalence of anemia attributable to insufficient dietary iron intake, stratified by age, sex, location, and year. Assigning disability weights to anemia severity levels (mild, moderate, severe) using standardized DWs on a 0–1 scale to reflect severity. Multiplying prevalence with disability weight for each severity level and summing across the population to obtain total YLDs. Adjusting for comorbidity, ensuring the burden reflects the independent health loss due to dietary iron deficiency anemia. The complete list is available at the GBD 2023 data input sources: https://ghdx.healthdata.org/gbd-2023/sources.
Data Analyses
This study used the methods and tools of the GBD 2023 study. The GBD study modeled the prevalence and YLDs of dietary iron deficiency anemia using DisMod-MR 2.1 and ST-GPR. ST-GPR is used to model the mean hemoglobin concentration over time and space to estimate the prevalence of dietary iron deficiency anemia in the population by severity levels. DisMod-MR 2.1 then integrates these prevalence inputs with other epidemiological data when applicable to ensure consistent estimates and calculate YLD by combining prevalence with established disability weights. 14 Both methods produce comparable estimates across locations and years, thereby identifying trends and the burden of dietary iron deficiency anemia in Eastern sub-Saharan Africa. Dietary iron deficiency anemia is stratified by severity (based on hemoglobin level) to refine the YLD estimate, with each severity category assigned its own disability weight reflecting the health loss experienced. To translate prevalence into YLDs, GBD multiplies the number of people with anemia at each severity level by disability weights that reflect health loss (e.g., higher weights for moderate and severe anemia). This yields estimates of non-fatal health burden stratified by location, age, sex, and cause. All parameter estimates generated in the GBD 2023 were accompanied by 95% UIs. The 95% UIs are derived from the 25th and 75th percentiles of the posterior distribution’s ordered 1,000 sample values, as described in the existing literature, ensuring that our estimates reflect a higher level of precision, especially when the data are uncertain. A non-overlapping UI with zero indicates statistical significance, indicating a meaningful association between the variables. A 95% UI not including zero means that the observed trend is highly likely to be real rather than random chance, a standard practice for assessing progress across GBD studies. 15 The percentage change in rates was calculated as the difference between the rates in 2023 and 1990, divided by the rates in 1990, representing the direction and magnitude of change over the past 34 years. We also calculated the age-standardized rates and corresponding 95% confidence intervals (CIs) based on the world standard population reported in the GBD Study 2023 for comparison across regions, and estimated the average annual percentage changes to measure temporal trends.
Ethics Aapproval and Iinformed Cconsent
The GBD study used fully anonymized aggregated data from multiple secondary sources. All data were accessed with permission from data-providing institutions and are compliant with relevant ethical standards. Informed consent was not required because no individually identifiable data were used.
Results
Prevalence
In 2023, there were no statistically significant differences in the age-standardized prevalence rate of dietary iron deficiency anemia by sex in the ESSA region. In 2023, there were an estimated 121 million cases of dietary iron deficiency anemia (95% UI: 104, 143) in ESSA region, 2023. Of these, 55 million (45.67%) were males (95% UI: 46, 67) and 66 million (54.33%) were females (95% UI: 57, 76). The corresponding age-standardized rate was 26,899 cases per 100,000 population (95% UI: 23092, 31657), with 22,757 cases per 100,000 males (95% UI: 18270, 28353) and 28,664 cases per 100,000 females (95% UI: 24577, 33486). In the same year, no statistically significant differences were found in the rates by sex. Prevalence rates were highest among children under five years, declined among adults aged 15-49 years, and remained elevated among females aged 25-49 years compared to males of the same age.
In 2023, there were national disparities in age-standardized dietary iron deficiency anemia prevalence rates in some countries of the region, in 2023 (Supplemental Table 1). Notably, Mozambique is emerged as the country with the highest age-standardized prevalence rate of dietary iron deficiency anemia, with a prevalence rate of 34464 cases per 100,000 population (95% UI: 31430, 50076). This was closely followed by Zambia with a prevalence rate of 34302 cases per 100,000 population (95% UI: 26915, 44916), the United Republic of Tanzania with 32,863 cases per 100,000 (95% UI: 28964, 37465), Somalia with 32863 cases per 100,000 (95% UI: 24172, 44037), and Eritrea which recorded a rate of 32863 cases per 100,000 (95% UI: 22780, 49169). The lowest age-standardized prevalence rate for dietary iron deficiency anemia was observed in Kenya (17565; (95% UI: 13752, 21894)).
From 1990 to 2023, the age-standardized rate was remaining unchanged throughout the region (Supplemental Table, Figure 1, and Figure 2). Age-sex specific prevalence rate of dietary iron deficiency anemia by age and sex in the ESSA region, 2023 Age-standardized prevalence rate of dietary iron deficiency anemia by location in the ESSA region, 1990 to 2023

Years Lived With Disability
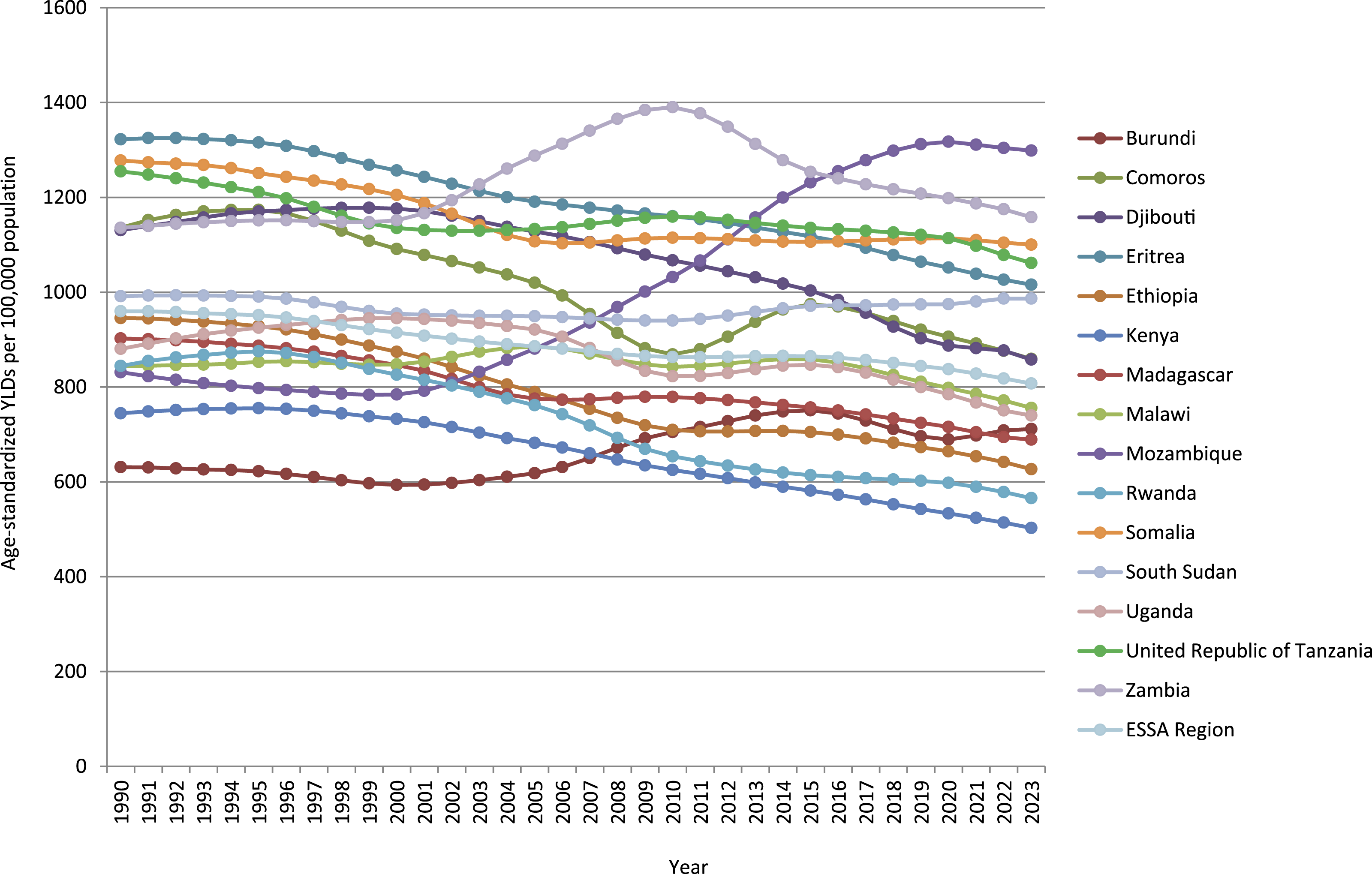
In 2023, there were an estimated 4 million (95% UI: 2.5, 6.3) YLDs in the ESSA region attributable to dietary iron deficiency anemia in 2023. Of these, 1.6 million (40.79%) were males (95% UI: 1, 2.6) and 2.3 million (59.2%) were females (95% UI: 1.4, 3.69). The equivalent age-standardized rate was 807 cases per 100,000 population (95% UI: 488, 1357), with 595 cases per 100,000 males (95% UI: 362, 1055) and 1006 per 100,000 females (95% UI: 602, 1626). In the same year, there were no statistically significant differences were found in the rates by sex and countries in the region. The highest YLDs rates were recorded in the under-5 age group for both sexes, with females showing higher YLD rates across nearly all age groups.
From 1990 to 2023, the age-standardized rate remained unchanged throughout the region (Supplemental Table, Figure 3, and Figure 4).
Discussion
This study provides a comprehensive estimate of levels and trends in the prevalence and YLDs rate of dietary iron deficiency anemia in ESSA region from 1990 to 2023. In this discussion, we will explore the trends of the non-fatal health outcomes of dietary iron deficiency anemia, compare them to regional patterns, and explore national, age, and sex differences. In addition, we will evaluate public health measures, while considering the limitations and potential solutions for mitigating dietary iron deficiency anemia in the ESSA region. Age-sex specific YLDs rates due to dietary iron deficiency anemia by age and sex in the ESSA region, 2023 Age-standardized YLDs rates due to dietary iron deficiency anemia by location in the ESSA region, 1990 to 2023
The age-standardized prevalence and YLDs rates of dietary iron deficiency anemia in Eastern sub-Saharan Africa from 1990 to 2023, showed no significant change since 1990. This unchanged trend of non-fatal health outcomes for dietary iron deficiency anemia over time suggests that no improvements in management of nutritional deficiency in Eastern part of sub-Saharan Africa. The previous GBD studies broadly reported that anemia burden (total prevalence and YLDs) remained highest in low-SDI regions such as sub-Saharan Africa. Dietary iron deficiency accounts for the largest share of anemia cases in most low-income regions, including sub-Saharan Africa, implying that it is a leading contributor to both the prevalence and YLDs.3,16 The lack of significant change in prevalence and YLDs of dietary iron-deficiency anemia from 1990 to 2023 likely reflects the persistence of structural nutritional determinants, population growth, infection burden, and limited scalability of interventions, compounded by data constraints within GBD modeling. In Eastern African countries, access to iron-rich food is inadequate due to the poor socioeconomic status, inadequate health care access, and inadequate utilization, which may result in anemia. 17 The availability and accessibility of animal source foods containing highly bioavailable micronutrients, particularly iron, must be improved through policy measures and education. In Africa, where most of the population is rural, the main foodstuffs consumed include corn-based products, onions and tomatoes, sunflower oil, peanuts, beans, rice, and baobab powder. Especially, during the dry season, animal products were almost completely absent from the diet. 16 In addition, although several countries in Sub-saharan Africa have adopted iron supplementation and school-based nutrition programs, coverage is inconsistent, and implementation challenges persist especially in remote or underserved regions.18,19 Apart from supplementation programs, agricultural and nutritional efforts should be made to improve the access and production of micronutrient dense foods. The National Nutrition Program must make more efforts to improve accessibility and use of iron-rich foods in collaboration with other sectors including the agricultural sector.
Despite insignificant regional variation in trend, in 2023 a relatively higher age standardized prevalence rate was observed in some countries like Mozambique, Zambia, the United Republic of Tanzania, Somalia and Eritrea, and a lower rate were observed in Kenya. This disparity may be attributed to variations in economic and cultural conditions, dietary habits, natural geographical environments, and unequal distribution of medical resources across countries.20,21 A previous study reported that dietary iron deficiency anemia disproportionately affects populations with limited access to healthcare and nutritious foods, especially in regions experiencing economic hardship. This was evidenced from the UNICEF report in 2016, which indicated a high prevalence of malnutrition mainly due to dietary iron deficiency was observed in Zambia, Mozambique, Madagascar, and Eritrea. 22
Dietary iron deficiency anemia shows significant variations in prevalence and YLDs rates across different age and sex groups. In general, the age-standardized prevalence and YLD rates of dietary iron deficiency anemia were higher among female individuals than males of the same age in most of age groups. Similarly, the 2021 GBD study reported that nutritional iron-deficiency anemia was one of the main conditions contributing to higher YLD rates in women. 23 A possible explanation for these sex differences in the non-fatal health outcomes of dietary iron deficiency anemia might be the gender inequalities in household food consumption, which probably exacerbate disparities in dietary iron deficient anemia. This is because women might be the most likely among household members to be affected by food insecurity18,24,25 and to lack access to sufficient quantities of iron-rich foods, 26 and be less likely to receive health screening and care.27,28 Although poverty is a barrier to accessing iron-rich foods, cultural factors also influence the distribution of iron-rich foods according to gender. In some countries of the region, the key iron-rich foods are prescribed to be fed to boys, whereas soft foods such as rice and tea are believed to be beneficial for girls. Therefore, in households economically able to purchase foods high in bioavailable iron, these foods are often preferentially fed to boys. 29 Social interventions, including education for girls and women and expanded agricultural empowerment (e.g., access to productive resources, self-managed time, decision making power, and financial control) of women, could help reduce these disparities.30,31 To design interventions that align with the social context where the target population lives, policymakers and program planners must consider the country context.16,19,29 When providing gender-transformative interventions, these norms are entrenched in social systems of unequal power and gender hierarchies. Without approaches that promote critical reflection of these norms by communities, shifting norms to be more gender-equitable will be challenging. 28 Therefore, to improve the health of women, especially in the prevention of dietary iron deficiency anemia, educational programs should be implemented using appropriate models of health education along with active participation mothers. 30
Concerning age-specific patterns of dietary iron deficiency anemia, a higher prevalence rate was recorded among children under five years of age, whereas the distribution of YLDs rate was higher among pediatric females than among other age groups. The higher prevalence rate and significant non-fatal health burden of dietary iron deficiency anemia among children and adolescent, especially in developing countries, might be due to a combination of factors including rapid growth, inadequate dietary iron intake, and increased iron requirements.32,33 i.e., children and adolescents with limited dietary diversity are more likely to have lower intakes of these essential iron sources, increasing their vulnerability to anemia. 34 Another previous study also revealed that, there is a significant association between low dietary diversity and anemia among adolescents (aged 6–18 years). Among all age groups, children under five exhibit the greatest vulnerability to chronic malnutrition and its associated micronutrient deficiencies35.
Dietary iron deficiency anemia affects fetal and neonatal development, potentially resulting in cognitive impairment and stunted growth. 36 Studies have shown that iron deficiency during pregnancy is strongly linked to a heightened risk of perinatal complications, such as premature birth and low birth weight. 20 In young children, iron deficiency is associated with adverse psychomotor, cognitive and socio-emotional development,28,37 with longitudinal studies demonstrating long-lasting adverse effects on behavior and development in adolescence, even if the deficiency has been corrected. 32 Therefore, interventions aimed at addressing dietary iron deficiency anemia, iron supplementation and dietary diversity promotion, are crucial in mitigating these health risks. 38 A diverse diet rich in iron-rich foods like red meat, poultry, fish, legumes, and leafy green vegetables is crucial for maintaining adequate iron stores and is associated with development of anemia. 34 Thus, designing multi-sectorial nutrition action plans that align agriculture (food security), education (nutrition knowledge), and health (supplementation and disease control) policies are recommended for comprehensive impact. Generally, our analysis of the non-fatal health outcomes of dietary iron deficiency anemia can provide the insights required to appropriately tailor interventions at the national and regional levels in effort to reduce the prevalence across all age and sex groups. Our estimates can have implications for reviewing the existing intervention measures, shaping programmatic priorities and supporting advocacy initiatives, all of which are imperative to achieving the targets set by the SDGs.
However, this study has several limitations. First, the study relies on estimates derived from the GBD methodology, where potential biases needs to be considered. Consequently, the actual level of dietary iron deficiency anemia in certain countries may have been either overestimated or underestimated, and results may be presented with broad and overlapping uncertainty intervals. These findings should be interpreted in light of limited primary data validation and substantial heterogeneity across countries in Eastern Sub-Saharan Africa. GBD 2023 estimates rely on modeled data where empirical nutrition surveys are sparse and regional aggregation may conceal important national differences in dietary intake, infection burden, and intervention coverage. Therefore, when interpreting the estimates, each country’s data collection environment and the potential for missing information, acknowledging that the true prevalence of dietary iron deficiency anemia may be higher or lower than the reported estimates. 23 Thus, the present results should be treated with caution by policy makers to prioritize resource allocation. Second, we were unable to further analyze the differences in the burden of non-fatal health outcomes of dietary iron deficiency anemia between urban and rural and among the different severity levels (mild, moderate, and severe). Finally, this study did not account for the role of ethnicity in the burden of dietary iron deficiency. It was evidenced from the previous research that there are significant variations in hemoglobin concentrations among different ethnic groups, with East Asians exhibiting higher concentrations than African Americans. 39
Conclusion
Dietary iron deficiency anemia has been a regional public health challenge in the ESSA region since 1990. A substantial difference was observed in the prevalence and YLD rate of dietary iron deficient anemia between sex and age groups. These findings underscore the urgent need for targeted interventions to address the persistent challenge of dietary iron deficiency anemia, particularly among female individuals and young children in ESSA countries. Future research should integrate local data on dietary practices, implement supplementation programs, and evaluate the effectiveness of intervention approaches, and piloting and scaling the best practices are also highly recommended.
Supplemental Material
Supplemental Material - Non-Fatal Health Outcomes of Dietary Iron Deficiency Anemia in Eastern Sub-saharan Africa, From 1990 to 2023
Supplemental Material for Non-Fatal Health Outcomes of Dietary Iron Deficiency Anemia in Eastern Sub-saharan Africa, From 1990 to 2023 by Sebsibe Tadesse, Girma Ashenafi, Gudina Egeta, Alqeer Aliyo, Angefa Ayele, Gelgelo Wodessa, Gemechis Tuke and Hailu Lemma in Sage Open Pediatrics.
Footnotes
Acknowledgements
The authors would like to thank the Institute for Health Metrics and Evaluation for coordinating the GBD 2023 study.
Ethical Considerations
The study used secondary data from the GBD 2023 study.
Author Contributions
ST conceived and designed the study. ST and HL were involved in the analysis and interpretation of the findings. All authors have approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.