
Abstract
ACFP-DP was developed to assess parental attitudes, beliefs, and knowledge about pediatric pain. In this methodological cross-sectional study, an initial item pool was appraised by 7 of 20 invited experts and pilot-tested in 41 parents and guardians of hospitalized children. Experts rated clarity, pertinence, and relevance; I-CVI, S-CVI/Ave, and modified kappa coefficients were calculated. Mean I-CVI was 0.89 (range, 0.71-1.00), S-CVI/Ave values were 0.878 for clarity, 0.905 for pertinence, and 0.899 for relevance, and modified kappa ranged from 0.66 to 1.00. Overall self-reported comprehensibility was 94.9%. These findings provide preliminary evidence of content validity and high pilot comprehensibility, but not full psychometric validation. Further studies should assess reliability, structural validity, construct validity, and score interpretation before broader use.
Keywords
Introduction
The role of parents and guardians in pediatric care has evolved substantially, moving from that of child companions to indispensable partners within the healthcare team.1,2 This paradigm, known as family-centered care, places the family at the core of decision-making and recognizes its fundamental influence on the child’s health and well-being.3,4 Collaboration between healthcare professionals and parents is especially important in the management of complex symptoms such as pain. 5
Pediatric pain remains a major clinical challenge and continues to be underestimated and undertreated.6,7 In early life, or in children with communication difficulties, the ability to self-report pain is limited, making caregiver observation and interpretation essential. 8 Because of their direct and continuous contact with the child, parents are often the first to detect behavioral changes that signal distress.9,10 Accordingly, parents’ ability to recognize, interpret, and accurately communicate their child’s pain to healthcare professionals is a cornerstone of effective analgesic management. 11
Successful pain management, however, depends not only on detection but also on parents’ attitudes, beliefs, and knowledge. 12 Previous studies have identified important barriers and misconceptions in this population, 13 including fear of analgesic side effects—particularly opioid addiction (opiophobia)—the belief that pain is necessary for healing or builds character, and difficulty distinguishing pain from anxiety.14-16 These beliefs may lead to underuse of prescribed analgesia and to reduced parental advocacy for adequate pain management in hospital settings.17,18
Reliable instruments are needed to measure these factors. Although many tools are available for pediatric pain assessment, most focus on the child’s self-report or on healthcare professionals’ knowledge.19-21 Instruments designed specifically for parents and guardians are usually restricted to particular contexts, such as the Parent Postoperative Pain Measure or oncology-related settings.22,23 These tools do not comprehensively address pediatric pain management in the broader home and hospital context. This highlights the need for broader instruments capable of assessing general attitudes, beliefs, and knowledge about pediatric pain in an integrated way. 24
The absence of an instrument that globally measures these dimensions limits both research and the design of educational interventions targeted at families. Therefore, the aim of the present study was to develop the ACFP-DP and obtain preliminary evidence of content validity through expert judgment, together with pilot data on comprehensibility among parents and guardians.
The development of a preliminary instrument of this kind may help strengthen family-centered care by identifying specific misconceptions and guiding the tailoring of educational interventions to the needs of each family.1,2,25 However, full psychometric validation is a fundamental subsequent step before such an instrument can be interpreted or used more broadly in clinical practice and research.26-28
Methods
This methodological, cross-sectional, observational study focused on early-stage instrument development, specifically content validation and pilot comprehensibility assessment of the ACFP-DP. The study followed the recommendations of the COSMIN framework for the selection and evaluation of health measurement instruments. 28 This phase did not include analyses of internal consistency, structural validity, construct validity, criterion validity, or test-retest reliability, which were reserved for subsequent validation studies with larger samples.
The process was carried out in 3 phases: (1) development of the first version of the ACFP-DP questionnaire; (2) expert content appraisal; and (3) administration of the revised questionnaire to parents and guardians to assess comprehensibility. In this manuscript, content validity refers to expert judgment about the adequacy of the items, whereas comprehensibility refers to the extent to which end users reported understanding the items during pilot testing.
Development of the Initial Version of the ACFP-DP
The initial item pool was generated through a focused review of the literature on family-centered care, pediatric pain assessment and management, parental misconceptions about analgesia, and caregiver educational needs.1,2,12-18,24,25,29-32 On the basis of this review and the study’s conceptual framework, the research team mapped candidate items to prespecified domains: caregiver attitudes toward pain-management strategies, beliefs about analgesia and pediatric pain, knowledge and self-perceived competence in pain management, and conceptual understanding of pediatric pain. At this stage, item generation was primarily literature-informed and theory-driven rather than based on a separate qualitative item-generation study.
The ACFP-DP questionnaire was structured into 5 blocks.
Block I collected caregiver sociodemographic variables, including relationship to the child, family situation, age, gender, educational level, and employment status.
Block II comprised 7 items addressing attitudes toward pediatric pain. Based on the scientific literature, these items focused on caregiver-centered strategies for pediatric pain management, especially nonpharmacological pain relief. Taken together, they covered different dimensions of parental attitudes and caregiving responses to the child’s pain experience and recognized pain as a multidimensional phenomenon.29,30
Block III comprised 6 items addressing a cognitive-attitudinal axis related to the use of analgesics and other pain-relief methods. Grounded in a biopsychosocial model of pediatric pain, this block assessed caregiving beliefs as central determinants of the quality of pediatric pain management.29,31,32
Block IV included 5 items exploring parents and guardians’ knowledge of pediatric pain management by combining practical skills, physiological knowledge, and self-perceived competence. This set of items assessed the interplay between skills, decision-making, and training, all of which are central to pediatric pain care.29,30
Blocks II, III, and IV used a 6-point Likert scale (0 = strongly disagree; 5 = strongly agree) to assess attitudes, beliefs, and knowledge related to pediatric pain management and to explore the perceived preparedness of parents and guardians.
Block V comprised 9 dichotomous questions (yes = 1; no = 0) designed to explore conceptual understanding of pediatric pain and the direct and indirect influence of parents and caregivers on the assessment, communication, and management of children’s pain.25,32
Different response formats were used because the blocks addressed distinct constructs. Blocks II-IV were designed to capture gradations in attitudes, beliefs, and self-perceived knowledge or preparedness, so Likert-type responses were considered more appropriate. Block V focused on conceptual understanding and common misconceptions about pediatric pain; therefore, dichotomous responses were used to simplify endorsement of statements during bedside administration.
At this preliminary stage, Block I is descriptive only. Blocks II-IV should be scored separately by summing item responses within each block (possible ranges: Block II, 0-35; Block III, 0-30; Block IV, 0-25), and Block V should be scored separately as a dichotomous knowledge-oriented block (0-9). Because negatively worded items require reverse coding and the dimensional structure has not yet been tested, no global total score, cutoffs, or normative interpretation are proposed at this stage.
Expert Content Appraisal
Content validation was conducted through expert judgment. The panel was intentionally multidisciplinary and experts were selected using the following inclusion criteria: (1) academic training in pediatrics, pediatric nursing, child psychology, or a closely related field; (2) clinical, teaching, and/or research experience involving pediatric pain or family-centered pediatric care; and (3) ability to evaluate item wording and conceptual adequacy. Experience in questionnaire development or methodological evaluation was also considered desirable. 33
An electronic invitation was sent to 20 experts to participate in the validation process. The invitation package included an evaluation form, a theoretical summary of the topic, and a detailed description of the validation procedure. Invitees were given up to 30 days to complete and return the evaluation. Seven experts responded (35.0%). Although this response rate was lower than expected, a final panel of 7 experts was considered methodologically acceptable for item-level CVI estimation in this phase 34 ; nonetheless, the possibility of non-response bias was taken into account when interpreting the findings.
Each expert evaluated the items in Blocks II, III, IV, and V of the questionnaire according to 3 criteria: clarity of language, pertinence, and relevance. Ratings were assigned using a 4-point ordinal scale, where 1 corresponded to ‘very little,’ 2 to ‘little,’ 3 to ‘quite a lot,’ and 4 to ‘very much,’ according to the degree to which each item was understood and considered appropriate.
For the assessment of clarity, the guiding questions were: ‘Is the language of each item sufficiently clear and understandable for the study participants?’ and ‘Will participants be able to interpret the item without ambiguity?’ For pertinence, the following question was used: ‘Do you consider the proposed items appropriate for evaluating the specific aspect intended to be measured by the questionnaire?’ Finally, to assess relevance, experts were asked: ‘Are the proposed items relevant to the context and target population?'
At the end of the evaluation process, experts were also able to provide comments, suggestions, and recommendations, as well as propose modifications to existing items, addition of new items, or deletion of unnecessary ones.
Content Validity Analysis
Content validity was examined using the Content Validity Index (CVI) to determine how well the items represented the theoretical constructs the instrument was intended to measure. Each item was assessed according to semantic clarity, conceptual pertinence, and relevance to the corresponding dimension. Item-level CVIs (I-CVIs) were calculated for each criterion as the proportion of experts assigning favorable ratings (‘quite a lot’ or ‘very much'). 34 Scale-level content validity was summarized using the average approach (S-CVI/Ave), calculated as the mean of the I-CVIs across items for each criterion and across the full set of item-criterion combinations.
To adjust agreement for chance, modified kappa coefficients were also calculated for each item and criterion using the probability of chance agreement for dichotomized ratings.26,27 For the 7-expert panel used in this study, an I-CVI of 0.78 or higher was considered acceptable. 34
Pilot Administration and Comprehensibility Assessment
The study population comprised parents, mothers, legal guardians, and primary accompanying caregivers of hospitalized children, all aged 18 years or older, attending a tertiary pediatric hospital.
This population was selected because of its central role in the process of pediatric hospitalization and its direct influence on the perception, expression, and management of pediatric pain. Parents and caregivers represent a key source of information about the hospitalized child’s experience and are fundamental agents in shared decision-making and in the implementation of family-centered care strategies.1,2
Including this population made it possible to explore knowledge, beliefs, and attitudes related to pediatric pain from a family, contextual, and humanized perspective, complementing the traditional clinical approach. Their participation was also essential for evaluating the understanding, acceptability, and pertinence of the instrument in a real pediatric hospitalization context, thereby strengthening its ecological validity and clinical applicability.
Statistical Analysis
Data were entered into Microsoft Excel and analyzed using IBM SPSS Statistics version 24. Descriptive statistics (absolute and relative frequencies) were used to summarize expert appraisal and pilot comprehensibility findings. No factor analysis or reliability analysis was performed in this initial phase because the objective was restricted to content validity and pilot comprehensibility.
For content validation, the I-CVI for each item was calculated as the number of experts assigning a favorable rating (‘quite a lot’ or ‘very much’) divided by the total number of experts (n = 7). S-CVI/Ave values were obtained by averaging I-CVI values across items. Modified kappa coefficients were calculated to adjust item-level agreement for chance. An I-CVI of 0.78 or higher was considered acceptable for panels of 6 or more judges. 34 Items that did not reach the threshold for at least 1 criterion were qualitatively reviewed and revised on the basis of expert comments.
In the pilot phase with parents and guardians, comprehensibility was analyzed by calculating the percentage of affirmative responses to the understanding check included after each item. Percentages above 80% were considered acceptable for this preliminary phase. Because this procedure was based on self-reported understanding, the results were interpreted as an initial indicator of comprehensibility rather than as a full assessment of item interpretation.
Results
Expert Content Validation Results
Of the 20 healthcare professionals linked to pediatric care who were invited to participate in the study, 7 completed and returned the questionnaire (response rate: 35.0%). The final expert panel comprised 2 pediatricians (1 woman with 12 years of experience and 1 man with 7 years of experience in specialized care), 4 pediatric nurses, and 1 child psychologist, thereby representing the main disciplinary profiles for which the questionnaire was designed. Although smaller than planned, this panel size was considered acceptable for item-level content validity analysis. 34
Summary of Item-Level Content Validity Index Values by Criterion (I-CVI)
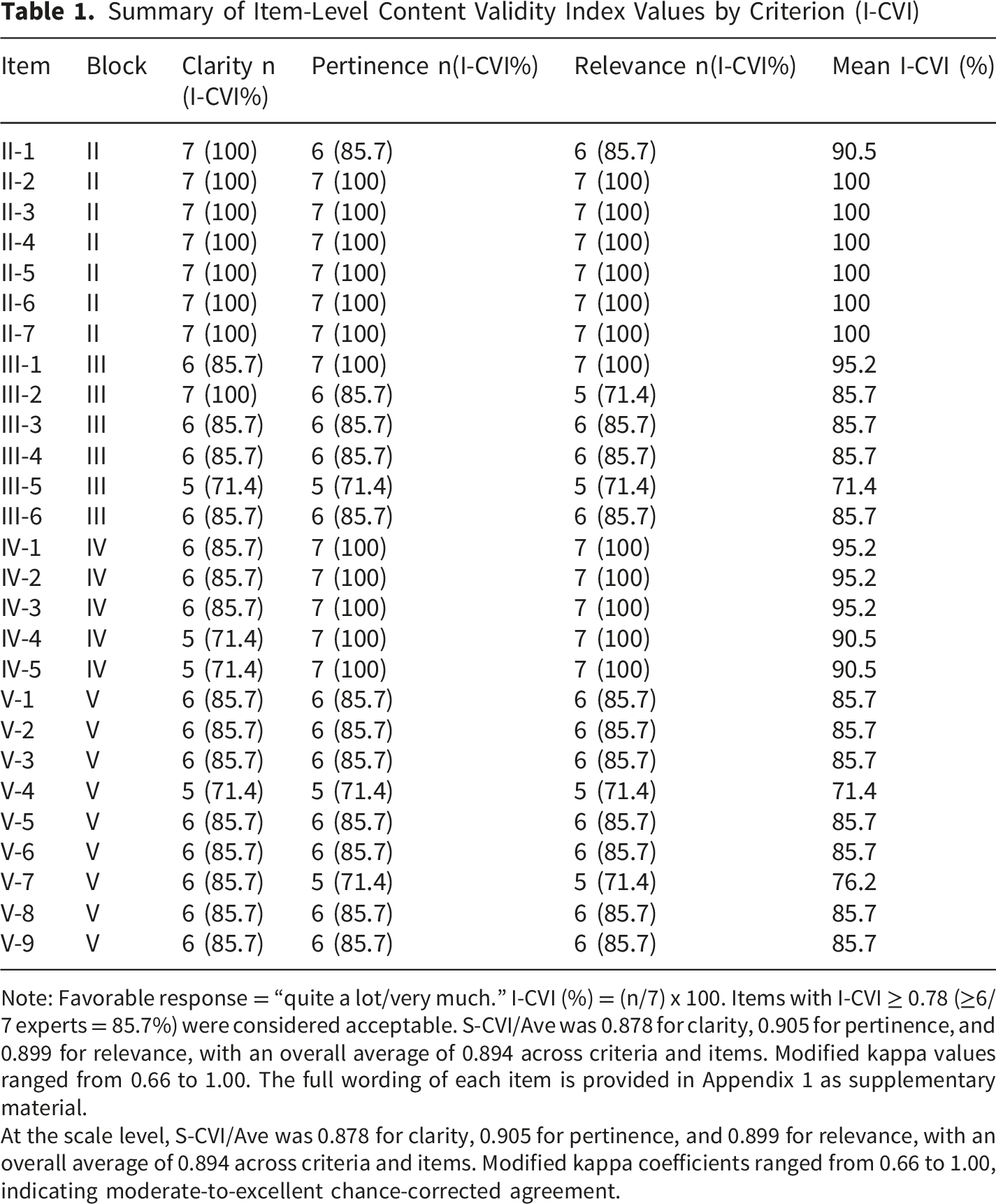
Note: Favorable response = “quite a lot/very much.” I-CVI (%) = (n/7) x 100. Items with I-CVI ≥ 0.78 (≥6/7 experts = 85.7%) were considered acceptable. S-CVI/Ave was 0.878 for clarity, 0.905 for pertinence, and 0.899 for relevance, with an overall average of 0.894 across criteria and items. Modified kappa values ranged from 0.66 to 1.00. The full wording of each item is provided in Appendix 1 as supplementary material.
At the scale level, S-CVI/Ave was 0.878 for clarity, 0.905 for pertinence, and 0.899 for relevance, with an overall average of 0.894 across criteria and items. Modified kappa coefficients ranged from 0.66 to 1.00, indicating moderate-to-excellent chance-corrected agreement.
For the clarity criterion, most items received high ratings from the experts, suggesting that the language used was understandable and appropriate for the target population. However, several items scored slightly below the threshold, which led to minor wording adjustments aimed at improving semantic precision and reducing ambiguity.
For pertinence, the experts considered the items appropriate for measuring the proposed theoretical constructs. The I-CVI values obtained reflected a satisfactory correspondence between the items and the questionnaire’s conceptual dimensions. Similarly, relevance was rated highly for most items, indicating that the content of the instrument was appropriate and meaningful for the clinical context and target population.
Summary of Revisions Proposed After Expert Review (Items With I-CVI < 0.78)
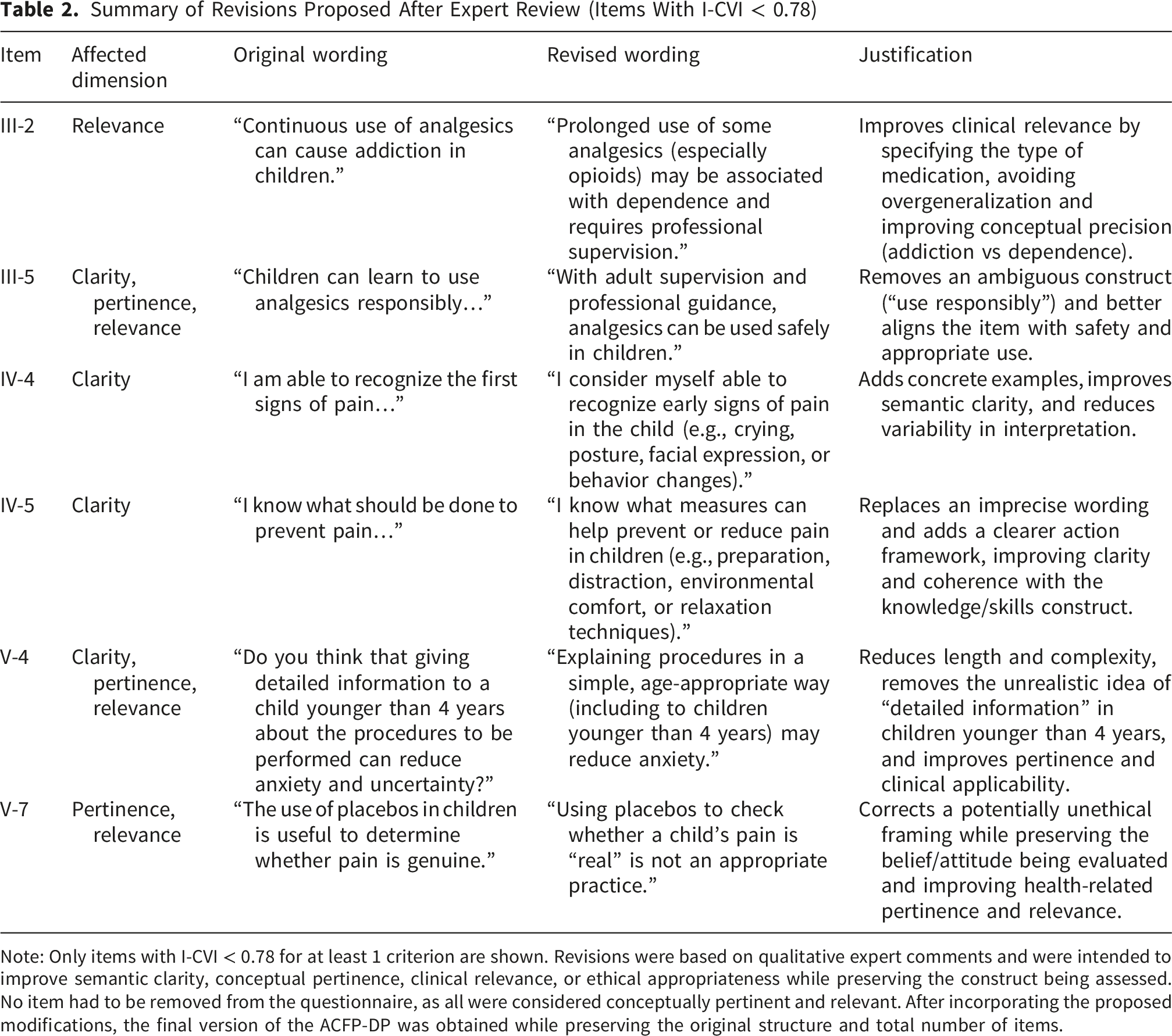
Note: Only items with I-CVI < 0.78 for at least 1 criterion are shown. Revisions were based on qualitative expert comments and were intended to improve semantic clarity, conceptual pertinence, clinical relevance, or ethical appropriateness while preserving the construct being assessed.
No item had to be removed from the questionnaire, as all were considered conceptually pertinent and relevant. After incorporating the proposed modifications, the final version of the ACFP-DP was obtained while preserving the original structure and total number of items.
Overall, the expert appraisal supports the preliminary content validity of the ACFP-DP in terms of clarity, pertinence, and relevance. These findings indicate that the item pool is conceptually adequate for subsequent psychometric testing, but they do not by themselves establish other measurement properties such as internal consistency, structural validity, or reliability.
Pilot Comprehensibility Testing With Parents and Guardians
The pilot phase was conducted with a sample of 41 parents and guardians of hospitalized children to evaluate item comprehensibility. The mean age of participants was 40.3 years, with representation across different age ranges (20-30, 31-40, 41-50, and >51 years), approximating a typical profile of primary caregivers in the hospital setting. Regarding kinship or caregiving role, mothers (n = 19) and fathers (n = 16) predominated, supplemented by other guardians or family caregivers (n = 5) and grandparents (n = 1), providing heterogeneity in caregiving experience and in the perception of pediatric pain from different family roles.
Educational level was also diverse, with vocational training being the most common category (n = 14). Caregivers with university education (n = 8) and postgraduate education (n = 5) were also included, alongside participants with intermediate and basic levels of schooling (compulsory secondary education/primary school certificate, n = 5; upper secondary education, n = 5; and primary education, n = 4). This educational variability is relevant for comprehensibility testing because it makes it possible to assess the clarity and accessibility of the questionnaire across different sociodemographic profiles, approximating the diversity expected in the target population.
In the pilot phase, the questionnaire was administered to parents and guardians (n = 41). To estimate item comprehensibility, a dichotomous understanding check was included after each question (‘Yes, I understood it well/No, I did not understand it well’ or ‘Yes/No,’ depending on the block). For each item, agreement was calculated as the proportion of affirmative responses out of the total number of valid responses.
Item Comprehensibility as Reported by Parents and Guardians (n = 41)
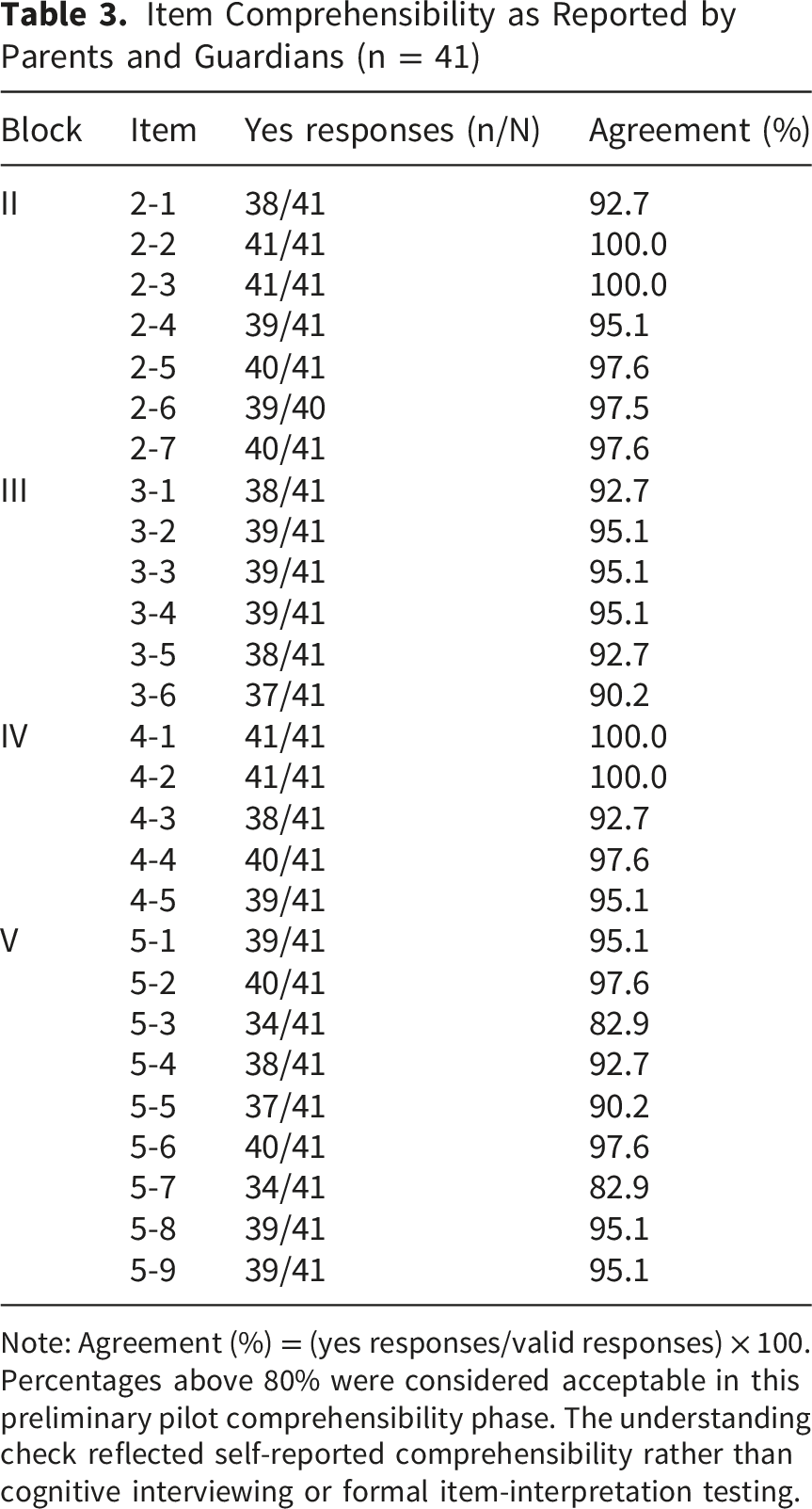
Note: Agreement (%) = (yes responses/valid responses) × 100. Percentages above 80% were considered acceptable in this preliminary pilot comprehensibility phase. The understanding check reflected self-reported comprehensibility rather than cognitive interviewing or formal item-interpretation testing.
Taken together, these findings indicate high comprehensibility of the instrument in the pilot sample, with understanding rates above 90% in all blocks. Nevertheless, 2 items in Block V (5-3 and 5-7) showed the lowest agreement values (82.9%), suggesting possible interpretation difficulties associated with more abstract wording or with conceptual and ethical content.
For this reason, minor revisions to the wording of these items (eg, clarifying terms or adding a brief explanation in the instructions) were considered appropriate before definitive administration, without changing the construct being measured. These adjustments would be incorporated into the final version of the questionnaire while preserving its original structure.
Discussion
The aim of this study was to develop the ACFP-DP and obtain preliminary evidence of content validity through expert judgment together with pilot data on comprehensibility among parents and guardians. The findings indicate that the initial item set was generally considered clear, pertinent, and relevant by the expert panel, and that the revised questionnaire was largely understandable for the pilot sample.
The overall content validity findings were favorable. The mean I-CVI across items was 0.89, S-CVI/Ave values were high across the 3 evaluated criteria, and modified kappa coefficients indicated agreement beyond chance. These indices suggest that the content domain was adequately represented in this first phase, consistent with recommendations for early instrument development.26,34
With respect to clarity, the experts rated the comprehensibility of the language positively, although some items required minor wording adjustments. This rewording process is common in validation studies and reinforces the value of expert judgment not only as a quantitative method, but also as a qualitative tool for improving semantic precision and linguistic suitability for the target population.
Regarding pertinence and relevance, the results indicate an appropriate correspondence between the items and the constructs they were intended to measure, as well as adequate suitability of the content for the clinical and family context of pediatric pain. This point is especially important because the questionnaire is directed at parents and guardians, a group for whom fewer validated instruments are available than for healthcare professionals or for children’s self-report.
The pilot phase showed high questionnaire comprehensibility among parents and guardians, supporting its preliminary feasibility for administration to caregivers of hospitalized children in the pilot context. The items with the lowest agreement were concentrated in the beliefs block, which is understandable because these formulations involve greater abstraction and may be more sensitive to wording nuances.
Once its measurement properties are confirmed in later validation studies, the ACFP-DP may provide nurses and pediatricians with a useful resource for operationalizing family-centered care. Rather than assuming that all parents have the same doubts, this instrument may eventually help the healthcare team identify specific cognitive or educational needs and tailor communication and support accordingly. 35
The multidisciplinary profile of the expert panel is a strength of the study, as it made it possible to integrate clinical, psychological, educational, and linguistic perspectives in the evaluation of the instrument. Nevertheless, several limitations should be considered. First, this phase evaluated only content validity and self-reported comprehensibility. Internal consistency, structural validity, construct validity, criterion validity, responsiveness, and test-retest reliability were not examined and will require subsequent studies with larger and more heterogeneous samples. Second, although 20 experts were invited, only 7 responded. This number is acceptable for item-level CVI analysis, but the 35% response rate may have introduced non-response bias if non-participating experts held different views. Third, item generation was primarily literature-informed and theory-driven; future studies could strengthen the instrument further through qualitative work with caregivers during item refinement. Fourth, comprehensibility was assessed with a dichotomous self-reported check, a pragmatic approach that may overestimate true understanding. Future research should incorporate cognitive interviewing or think-aloud methods to explore how caregivers interpret each item and response option. Finally, the pilot sample was drawn from caregivers of hospitalized children in a single center, whereas the instrument is intended for broader use across hospital and community settings; therefore, the generalizability of the pilot findings remains limited.
At this stage, the most appropriate use of the instrument is descriptive and block-specific. Block scores can be summed within each conceptual domain, but no global cutoffs or normative interpretation should yet be applied until the dimensional structure, reverse-scoring strategy, and reliability are established.
Conclusions
This study provides preliminary evidence supporting the content validity of the ACFP-DP and shows high self-reported comprehensibility in a pilot sample of parents and guardians of hospitalized children. These findings should be interpreted as an initial stage in instrument development rather than as full validation.
If future studies confirm its structural validity, reliability, and interpretability, the ACFP-DP may become a useful tool for identifying caregiver beliefs, attitudes, and knowledge gaps relevant to family-centered pediatric pain care. Subsequent validation work should include larger and more diverse samples from both hospital and community settings, together with analyses of internal consistency, construct validity, and test-retest reliability.
Supplemental Material
Supplemental Material - Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain
Supplemental Material for Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain by Abel Checa-Peñalver, Inmaculada García-Valdivieso, Juan Manuel Pérez-Pozuelo, María Isabel Donoso Calero, Miriam Hermida-Mota, Sonsoles Hernández-Iglesias and Sagrario Gómez-Cantarino in Sage Open Pediatrics.
Supplemental Material
Supplemental Material - Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain
Supplemental Material for Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain by Abel Checa-Peñalver, Inmaculada García-Valdivieso, Juan Manuel Pérez-Pozuelo, María Isabel Donoso Calero, Miriam Hermida-Mota, Sonsoles Hernández-Iglesias and Sagrario Gómez-Cantarino in Sage Open Pediatrics.
Supplemental Material
Supplemental Material - Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain
Supplemental Material for Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain by Abel Checa-Peñalver, Inmaculada García-Valdivieso, Juan Manuel Pérez-Pozuelo, María Isabel Donoso Calero, Miriam Hermida-Mota, Sonsoles Hernández-Iglesias and Sagrario Gómez-Cantarino in Sage Open Pediatrics.
Supplemental Material
Supplemental Material - Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain
Supplemental Material for Development and Content Validation of the ACFP-DP: A Questionnaire on Parental Attitudes, Beliefs, and Knowledge About Pediatric Pain by Abel Checa-Peñalver, Inmaculada García-Valdivieso, Juan Manuel Pérez-Pozuelo, María Isabel Donoso Calero, Miriam Hermida-Mota, Sonsoles Hernández-Iglesias and Sagrario Gómez-Cantarino in Sage Open Pediatrics.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ERDF funding: 2025-GRIN-38507 G-ENDOCU Research Group and European Union – European Social Fund Plus (FSE+) of Castilla-La Mancha.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.