
Abstract
Reports on the association between hemophilia and pediatric diabetes are very scarce in the literature, with no more than four worldwide. This report describes the case of a 14-year-old male with severe hemophilia A and type 1 diabetes who was brought to the emergency department due to fever and bruising on his back and jaw following trauma. The patient responded well to plasma-derived factor VIII, drainage, antibiotic therapy, and management with NPH and Regular insulin. There were no problems with the use of subcutaneous insulins during hospitalization. Previously reported cases in the literature describe potential bleeding and bruising associated with devices used for managing pediatric diabetes. However, severe bleeding and bruising that significantly impede diabetes treatment do not appear to be present, although individualized management is still required.
Introduction
The association between diabetes and hereditary hemophilia is very rare. 1 In the pediatric population, only 4 cases of this association in the same patient have been reported.1-4 This is the first case report on the association of hereditary hemophilia and pediatric diabetes in Latin America. This association is clinically significant beyond rarity since diabetes management requires devices that can induce significant bleeding or injuries in children with severe hemophilia. The use of continuous glucose monitors (CGMs), subcutaneous insulin, and insulin pumps can be concerning in hemophiliac patients due to the increased risk of bleeding and bruising associated with this condition. Joint management between specialists in pediatric hematology and endocrinology is necessary. Therefore, a novel case and a review of the literature are discussed below.
Case Report
Ancillary Tests During Hospitalization
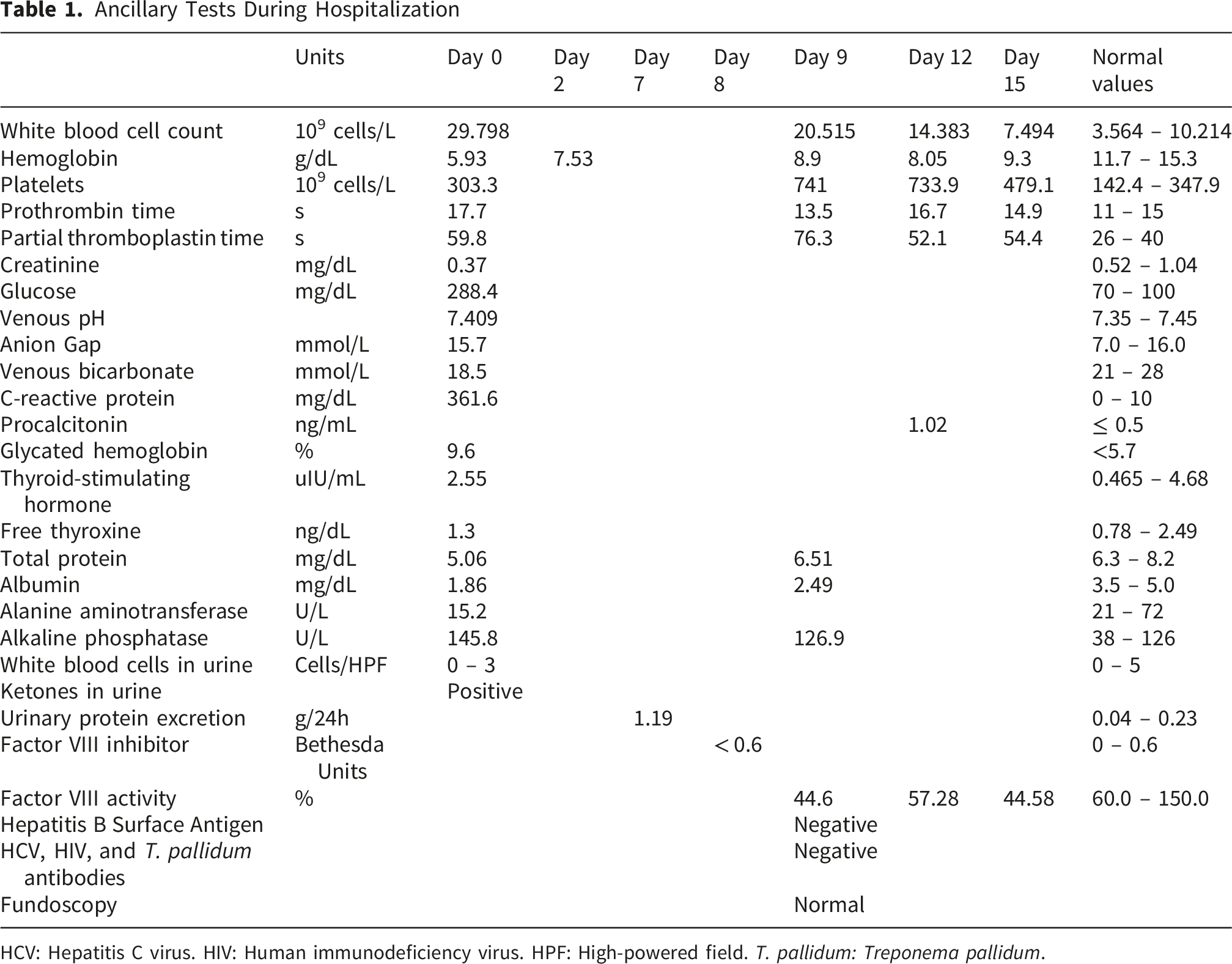
HCV: Hepatitis C virus. HIV: Human immunodeficiency virus. HPF: High-powered field. T. pallidum: Treponema pallidum.
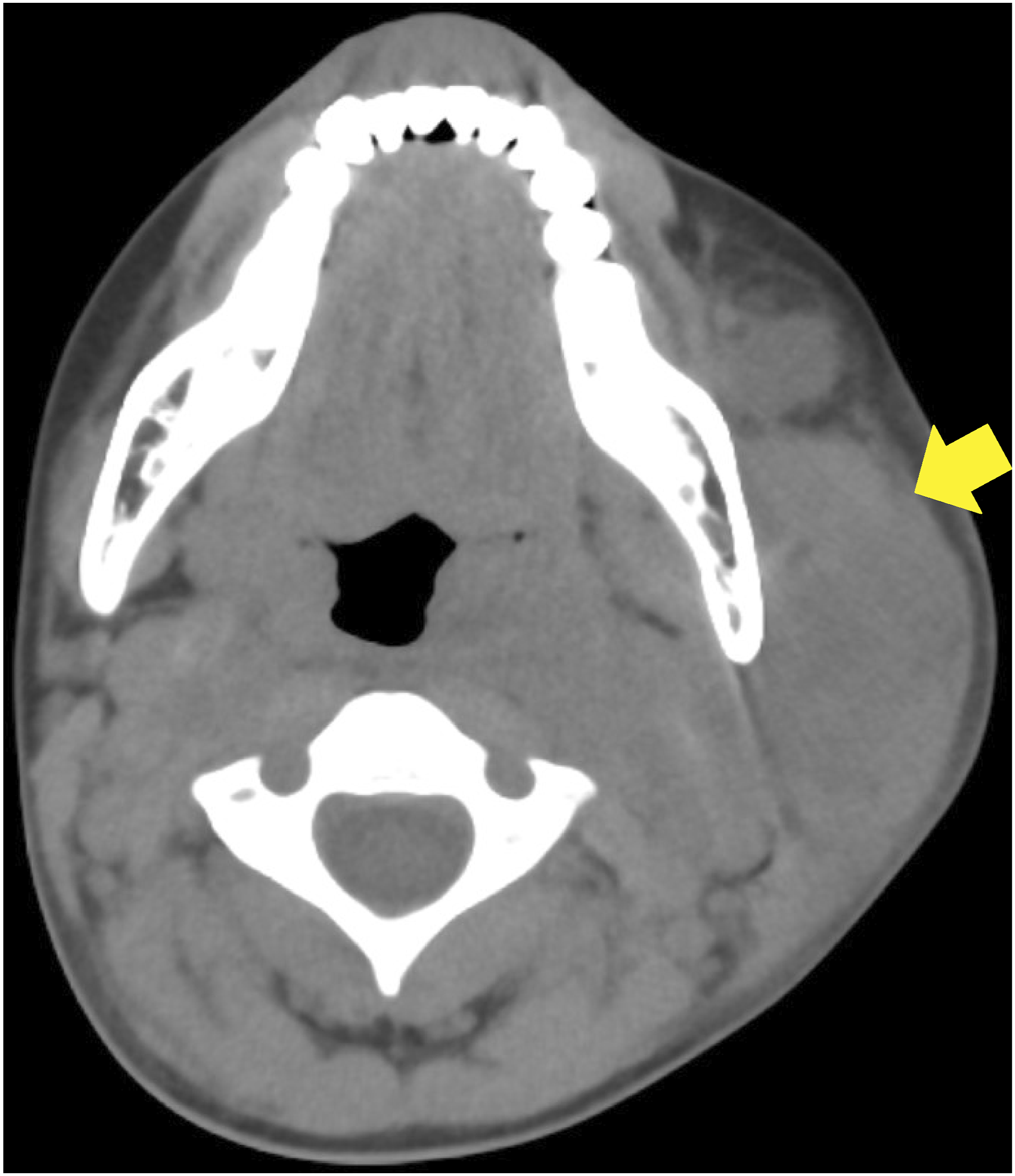
Axial non-contrast head CT (3 mm slide thickness) with arrow indicating a heterogeneous mass located in the left submaxillary region
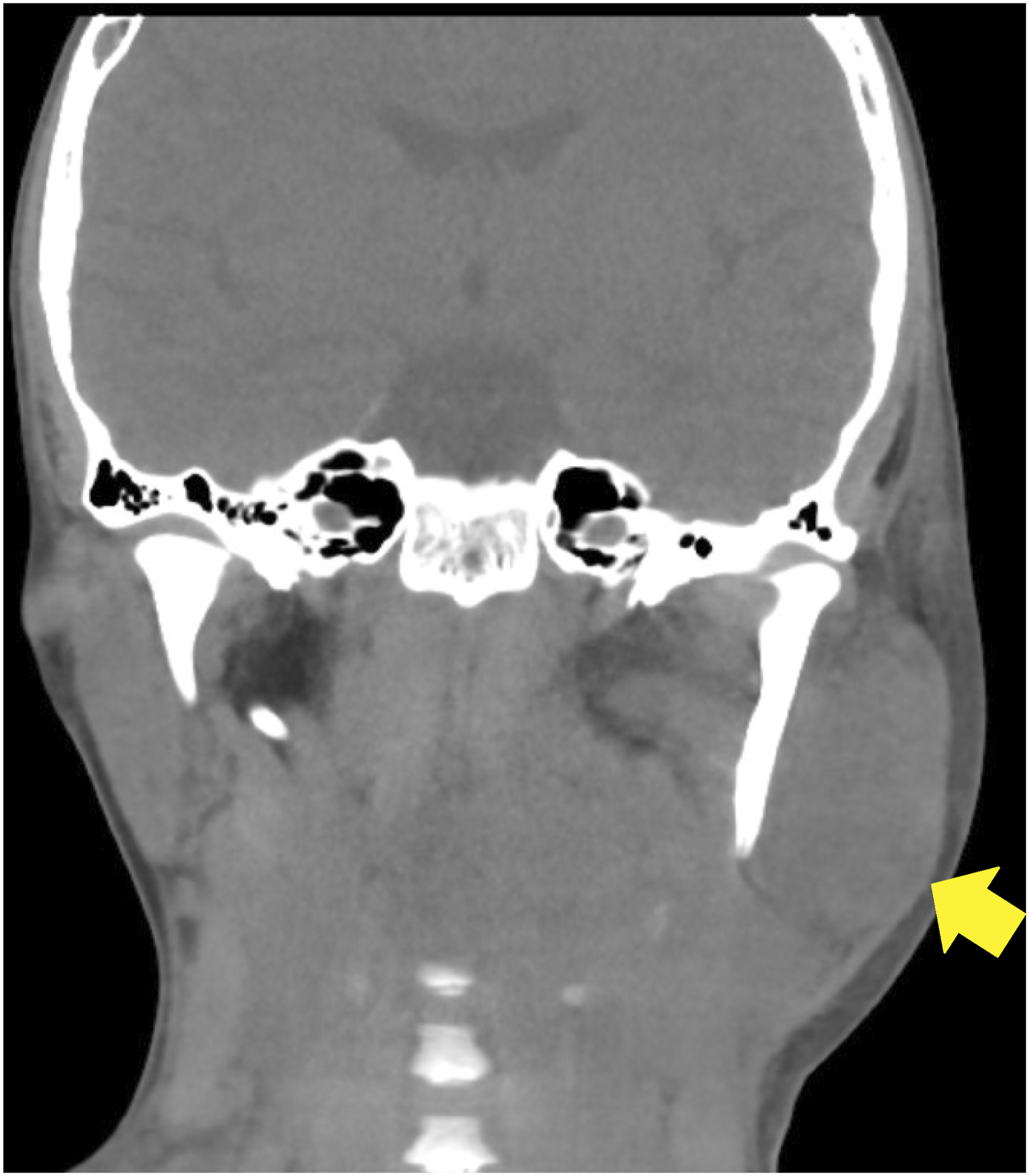
Coronal non-contrast head CT (3 mm slide thickness) with arrow indicating a heterogeneous mass in the left submaxillary region
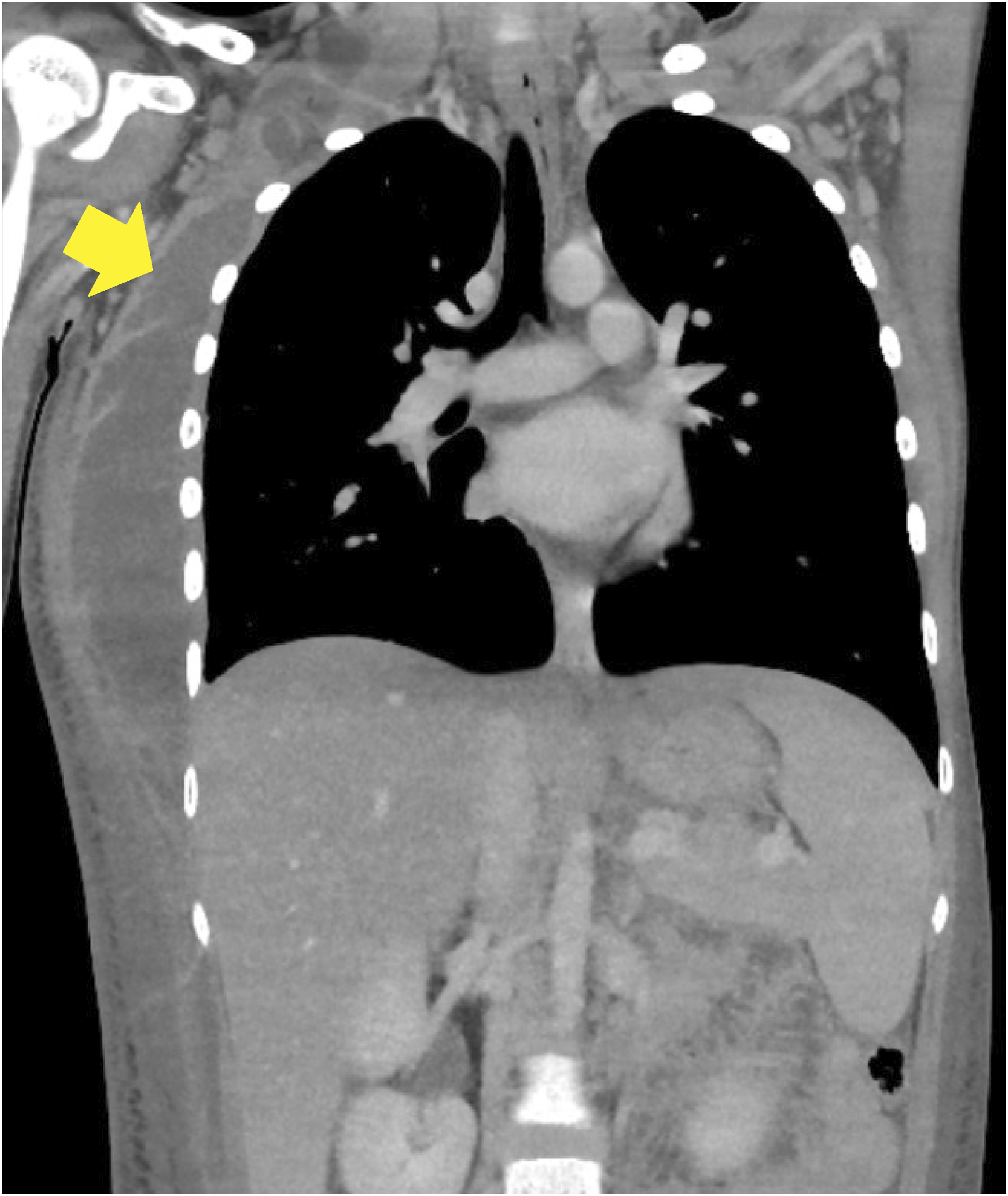
Coronal non-contrast chest CT (2 mm slice thickness) with arrow indicating a hyperdense area extending from the right clavicular region to the twelfth right rib

Axial non-contrast chest CT (2 mm slice thickness) with arrow indicating a hyperdense region in the lower and posterior area of the right lung
On the third day, the patient was transferred to the pediatric ward and transitioned to subcutaneous (SC) NPH and R insulin. Additionally, a blood culture obtained before antibiotic therapy revealed clindamycin-sensitive Streptococcus pyogenes. Over the following days, the patient received tramadol and even morphine for pain management.
On day 12, purulent fluid was drained from the left submaxillary tumor in the operating room. On the 15th day, S. aureus was found in the culture of this fluid, and vancomycin was administered for persistent fever. However, the patient developed a rash after the administration of vancomycin, and it had to be stopped. Later that day, purulent material was removed from the right thoracic area in the operating room. Following this, the patient was transferred to the Pediatric Intensive Care Unit (PICU). In the PICU, linezolid 600 mg IV q12h was administered for 7 days, and the fever resolved.
On day 23, the patient was transferred to the general pediatric ward to adjust the SC insulins dosages and one week later was discharged. During hospitalization, no bleeding or hematomas were observed with the use of SC insulins. It is unknown whether the patient experienced any bleeding or bruising from insulin injections before this admission, as he has communication difficulties and his relatives were not aware of the presence of these adverse effects.
During hospitalization, the patient received 1500 – 4500 IU of pdFVIII daily and, upon discharge, was instructed to use prophylaxis with 1000 IU of pdFVIII three times per week. Furthermore, a C-peptide level of 0.1 ng/mL (1.1–4.4 ng/mL) was obtained, islet cell antibodies were negative, and anti-GAD, anti-insulin, and anti-ZnT8 antibodies were positive. These results confirmed that the patient had type 1 diabetes.
Discussion
The first report of hemophilia and pediatric diabetes in the same patient is from 1958, in which the case of a child with classic hemophilia who developed diabetes when he was 10 years old is described very briefly in a letter to the editor. 2 According to the author, he seemed to bleed at the insulin injection site only when he was in a “bleeding phase”. 2 The author also suggested that the low incidence of the association between hemophilia and diabetes might be related to the fact that most people with hemophilia had died at a relatively young age. 2 This report did not mention the type of diabetes or the type of hemophilia the child had. 2 The studies that led to the diagnosis of hemophilia were not detailed, nor was it specified whether the child was receiving any prophylactic therapy for this diagnosis. 2 Another letter to the editor, adjacent to the one already described, mentioned the case of a 71-year-old man with diabetes and hemophilia, without providing further information about the diagnosis or treatment of these diseases. 6
Due to the scarcity of literature on the association between hereditary hemophilia and pediatric diabetes, it is also relevant to mention the case of an adult published in 1962. 7 This patient was a 31-year-old male with hemophilia A who was diagnosed with diabetes at age 24. 7 He had experienced several bleeding episodes in several joints since childhood. 7 According to the report’s author, despite initial concerns about using subcutaneous insulin in this patient, he was successfully managed with NPH insulin using fine needles. 7 During seven years of treatment, the only incident related to subcutaneous insulin use was a single injection site infection. 7 The author did not describe the type of diabetes, provide details about the studies that led to the hemophilia A diagnosis, or indicate whether the patient was receiving any prophylaxis for his hemophilia diagnosis. 7 However, the report mentions the absence of bleeding problems resulting from diabetes management in this patient. 7
In 1974, there was another report of a child who had a history of bleeding from minor trauma since he was 6 months old, who at 9 months was diagnosed with classic hemophilia A with a factor VIII (FVIII) level < 1%. At 13 months, he was diagnosed with diabetes after experiencing polyuria and polydipsia for two weeks. 4 At the time of diagnosis, he had altered mental status, glucosuria, ketonuria, and a blood glucose level of 850 mg/dL. 4 The patient responded to injections of long-acting and rapid-acting insulins. 4 The authors did not describe the type of diabetes the patient had, nor did they mention whether he received prophylaxis for his hemophilia diagnosis or if there were any bleeding problems associated with the insulin injections. 4
In 2021, the case of a 6-year-old child with severe hemophilia A, diagnosed at 8 months of age, was reported. 1 The diagnosis was based on FVIII activity <1% and normal von Willebrand factor antigen levels. 1 Shortly after diagnosis, the patient began receiving prophylaxis with recombinant FVIII (rFVIII), and by age 6, he was using a dose of 35–40 U/kg three times a week. 1 At age 6, the boy experienced polyuria, polydipsia, polyphagia, and weight loss for one week. 1 Blood tests were performed, revealing a glucose level of 291 mg/dL, HbA1c of 10.5%, positive islet cell and insulin antibodies, negative anti-GAD antibodies, and a C-peptide level of 0.35 mg/mL, leading to the conclusion that the patient had type 1 diabetes. 1 For diabetes management, the patient initially received treatment with glargine and glulisine insulins, without showing adverse effects. 1 After a few days, the patient began using a CGM and sensor-augmented pump therapy with predictive low glucose suspend mode. 1 Due to frequent automatic interruptions in the insulin infusion and the presence of blood in the insulin delivery tubing, the insulin pump was discontinued after six months, and detemir and glulisine insulins were used. 1 Injections were administered once or twice daily, and a higher frequency of injections was associated with more local lesions. 1 Three months later, the basal insulin was changed to degludec, with which the patient experienced minor bruising, which apparently did not affect its effectiveness. 1 On the other hand, bruising was more frequent on Mondays, possibly because these were the days with the longest time elapsed since the last rFVIII injection (administration days: Tuesday, Thursday, and Saturday). 1 Furthermore, bleeding was more common when the CGM was applied shortly before administering rFVIII (likely because the effect of the last rFVIII dose was wearing off), which could even interfere with the sensor’s performance. 1 Therefore, it was recommended to apply the CGM shortly after administering rFVIII, and with this, the sensor functioned well even when bleeding occurred, although it was not excessive. 1 One month after the diagnosis of type 1 diabetes, the child developed a calf injury, and six months later, a gum injury requiring sutures. 1 In both cases, rFVIII was infused, resulting in no bruising at the injection sites, and the previous injuries were even absorbed more quickly. 1
Finally, another report published in 2021 describes the case of a child who was diagnosed with severe hemophilia A at 2 months of age, with FVIII activity <1% at diagnosis, and type 1 diabetes at 2 years of age. 3 Following the hemophilia diagnosis, the patient began treatment with pdFVIII on demand. 3 At 18 months of age, the patient used a prophylactic dose of 500 IU (37.5 IU/kg/day) three times a week. 3 The diabetes was successfully managed using glargine and aspart insulins, with 4 to 6 injections per day and glucose monitoring at least 8 times daily. 3 To simplify treatment, at 7 years of age, the patient was switched to prophylaxis with rFVIII at 500 IU (24 IU/kg) twice a week. 3 Using rFVIII as prophylaxis allowed for a reduction in the number of infusions to twice a week, a shorter infusion time, a smaller infusion volume, and easier management. 3 Six months later, the rFVIII dose was increased to 1000 IU (43 IU/kg) twice a week due to the patient’s weight gain and increased physical activity, and it was administered on days when greater physical activity was expected. 3 The child did not develop inhibitors against FVIII. 3 Occasional joint bleeds while playing soccer were successfully treated with rFVIII infusions and magnetotherapy. 3 Minor bruising secondary to mild trauma or insulin administration did not require treatment. 3
As can be seen in the cases described, the older reports did not mention the type of diabetes because the terms type 1 diabetes and type 2 diabetes, as well as their characteristics, were defined in 1997. 8 The recent reports do classify the type of diabetes as type 1 diabetes,1,3 which is the same type of diabetes that the patient in this new case report had.
Furthermore, the initial reports did not describe any prophylactic therapy for hemophilia,2,4,6,7 probably because FVIII concentrates appeared in the 1970s. 9 Recent reports do describe the use of prophylaxis with FVIII concentrates, either pdFVIII or rFVIII.1,3 In individuals with severe hemophilia, prophylaxis with pdFVIII or rFVIII is suggested, and pdFVIII is recommended during the first 50 days to reduce the risk of developing inhibitors. 10 The patient in this report always used pdFVIII because it was the only one available. However, using rFVIII instead of pdFVIII may be easier, reduce the number of weekly infusions, and decrease the infusion time and volume. 3
Regarding the presence of bleeding or bruising during insulin injection in published pediatric cases,1-4 in one case, the presence of this complication is unknown. 4 The other three cases did have it1-3 (in one, the type of insulin is not mentioned, 2 and the other two used insulin detemir, 1 insulin glulisine, 1 insulin degludec, 1 insulin glargine, 3 and insulin aspart 3 ). At the time of Quick’s report, 2 prophylaxis with FVIII concentrates was not available, 9 which would easily explain the bleeding with insulin administration.
Summary Table of the Pediatric Cases With Diabetes and Hemophilia Reported in the Literature, Including This Case Report
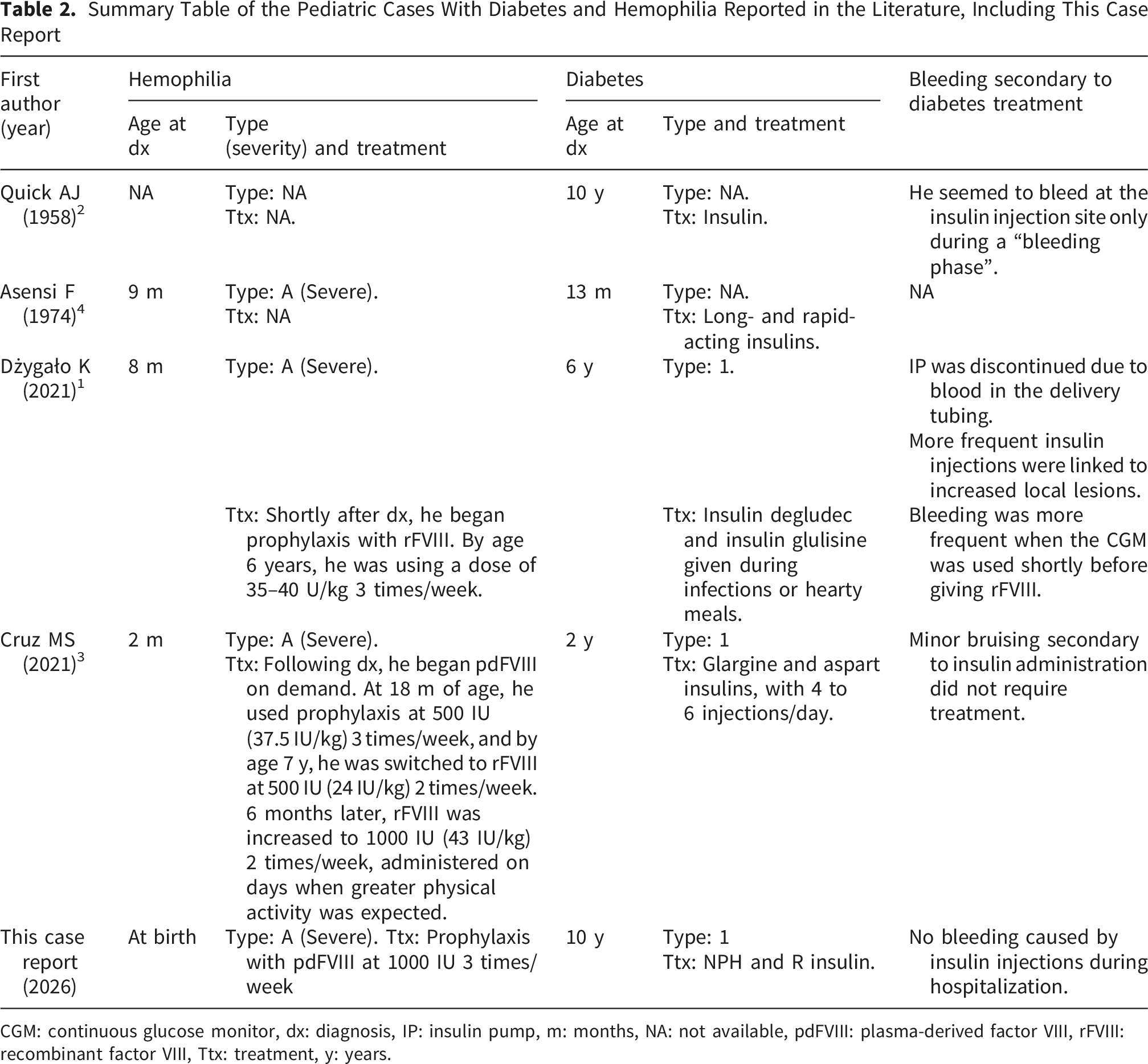
CGM: continuous glucose monitor, dx: diagnosis, IP: insulin pump, m: months, NA: not available, pdFVIII: plasma-derived factor VIII, rFVIII: recombinant factor VIII, Ttx: treatment, y: years.
Only one previous report describes the use of a CGM and insulin pump in a child with hemophilia and diabetes. 1 Bruising and bleeding occurred with the use of these devices. 1 This necessitated discontinuation of the pump as it was not functioning correctly due to bleeding in the insulin delivery tubing. 1 Although it was indicated that the CGM should be placed after and not before administering rFVIII, the bleeding episodes upon placement (although not excessive) did not entirely subside. 1
Clinical Considerations
According to the available literature, we can draw some suggestions that might be useful for managing pediatric diabetic patients with hemophilia. Pump therapy may not be useful in patients with severe hemophilia, as blood in the insulin delivery tubing may impair pump function. 1 Insulin injections should be reduced to a minimum to minimize local lesions, with a preference for once-daily basal insulins over NPH insulin when available. 1 Regarding CGM placement, it is recommended to apply the CGM shortly after administering rFVIII, to avoid the increased risk of bleeding that may arise as the effect of the last rFVIII dose wears off. 1 There is no literature describing differences in the frequency of local lesions by CGM placement site in patients with hemophilia.
In patients with the association of hemophilia and pediatric diabetes, multidisciplinary care should involve pediatric hematology, pediatric endocrinology, nursing, and social work. Especially for patients such as the one in the present report, given the complex psychosocial barriers (autism, limited family supervision, financial constraints), multidisciplinary care is essential.
Conclusion
While subcutaneous insulin injections, CGM placement, and insulin pump use can cause bleeding and bruising in children with hemophilia and diabetes, these have not been reported to be severe or to prevent diabetes treatment. However, individualized management is required. Current published experience does not address the timing of FVIII prophylaxis relative to insulin injections or specific monitoring parameters in children with hemophilia and diabetes. It seems to be good practice to apply the CGM shortly after administering rFVIII. The current literature suggests that alternative diabetes technologies, such as insulin pumps, are not useful in patients with severe hemophilia. This report is expected to contribute to the limited literature on the management of pediatric patients with hemophilia and diabetes, particularly in resource-limited settings.
Footnotes
Ethical Considerations
Patient information was obtained with the written informed consent of the patient’s parents. The Institutional Ethics Review Board of the Hospital Nacional Dos de Mayo approved this report (Ethical Approval Code: 090-2025-CEIB-HNDM).
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad San Ignacio de Loyola funded the publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized data for the purpose of medical research or teaching can be requested from the Department of Pediatrics at Hospital Nacional Dos de Mayo, Lima, Peru.