
Abstract
Keywords
Background
Warfarin use in the perioperative setting creates challenges due to the delayed and variable time to peak effect and because warfarin may be potentiated by other genetic and pharmacokinetic characteristics.1,2 Guidance for warfarin use in this setting primarily is based on indirect evidence and clinical experience. 2 The decision to discontinue anticoagulants with or without heparin bridging is made by assessing thrombotic risk if anticoagulation is discontinued and bleeding risk with concomitant antithrombotic drug administration. For invasive surgical procedures with a significant bleeding risk, warfarin is discontinued 5 days before surgical interventions with international normalized ratio (INR) assessment within 24 hours of the procedure. Following the surgery, most often warfarin may be resumed 12 to 24 hours postoperatively depending on bleeding and thrombotic risks. For less invasive procedures with minimal bleeding risk, warfarin therapy may continue through the procedure. 2
The current Chest guidelines of anticoagulation therapy do not contain recommendations regarding use of warfarin around the time of tattoo placement. 2 The guidelines do provide level 2C recommendations to continue vitamin K antagonists for minor dermatologic procedures, which include excision of basal and squamous cell skin cancers, actinic keratoses, and premalignant or cancerous skin nevi. 2 Similar to the aforementioned cutaneous procedures involving the dermal layer, tattoo placement marks the skin by making punctures to the dermal layer and inserting pigments, and minor bleeding is possible. Thus, recommendations of warfarin management for cutaneous procedures may reasonably be extrapolated to tattoo placement.
Literature Review
PubMed and IDIS were searched (up to May 2013) using the search terms vitamin K antagonists, warfarin, anticoagulation, tattoo, tattoo placement, cutaneous procedure, and cutaneous surgery. The search was expanded to include the terms “cutaneous surgery” and “cutaneous procedure,” since trials evaluating vitamin K antagonists, warfarin, anticoagulation, and tattoo placement have not been published. Prospective clinical trials were included if they were published in English and included subjects receiving vitamin K antagonists undergoing cutaneous surgery. Case reports and review articles were excluded. Eleven trials, 4 retrospective and 7 prospective, met the expanded criteria and were included in this evaluation.
Ah-Weng and colleagues retrospectively evaluated perioperative outcomes of patients on warfarin therapy undergoing cutaneous surgery from January 1999 to June 2002 in a single center. 3 The primary outcome was incidence of perioperative bleeding in patients receiving warfarin. The study included 68 patients undergoing 85 cutaneous procedures; the mean age of the patients was 75 years. The procedures are listed in Table 1. Most procedures were performed with INR evaluation the day of surgery, with few checked 24 to 48 hours prior to the surgery. Excessive intraoperative or postoperative bleeding was not reported. The authors concluded that warfarin should be continued prior to dermatologic surgery as long as the INR is less than 3.5 and monitored 24 hours before surgery. 3 This study did not report specific methodology, statistics, or demographic information pertaining to the indication for anticoagulation. Other limitations include that this study was a retrospective evaluation without a comparator group.
Comparison of Articles Evaluating Bleeding Complications.
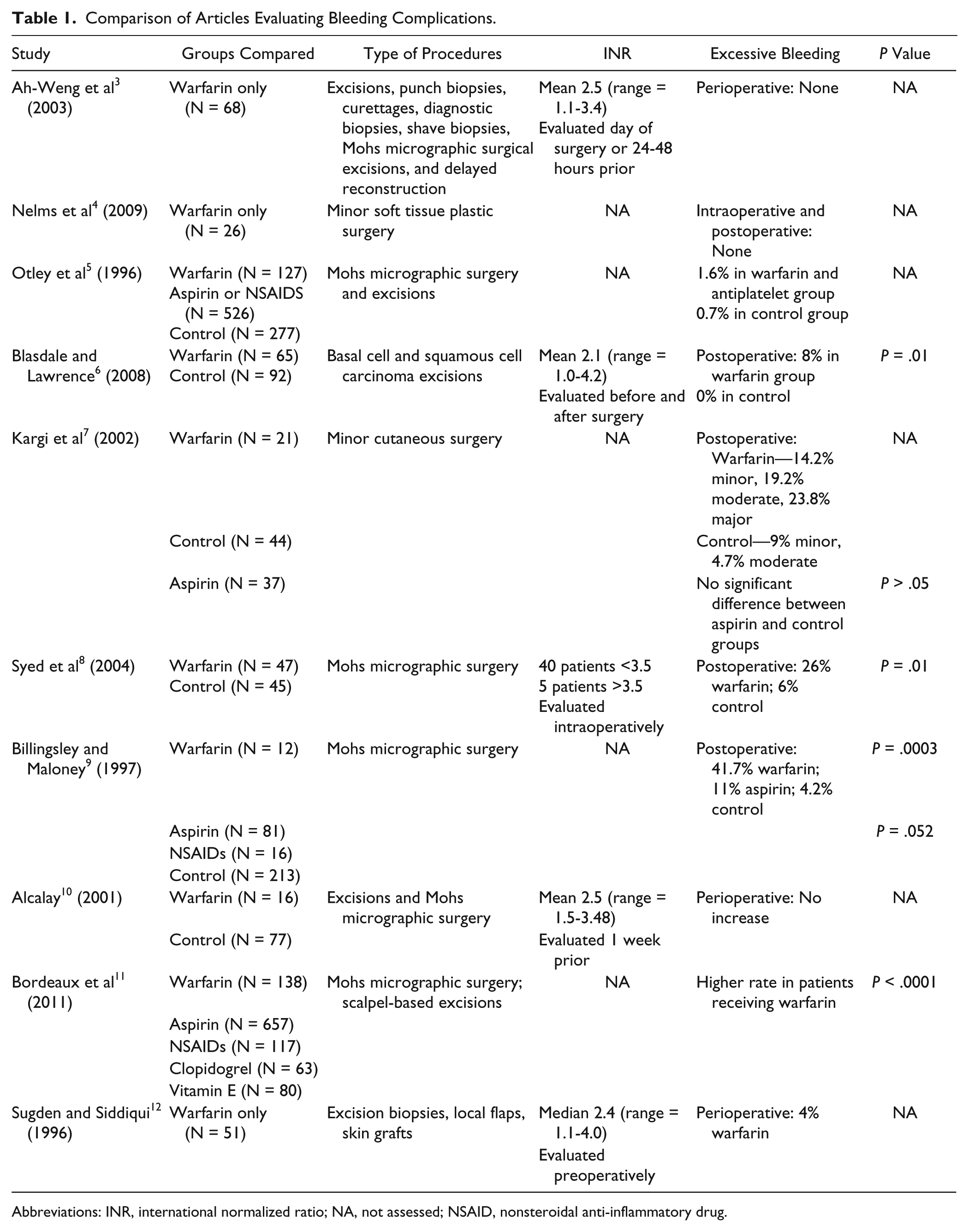
Abbreviations: INR, international normalized ratio; NA, not assessed; NSAID, nonsteroidal anti-inflammatory drug.
Nelms and colleagues retrospectively evaluated 26 patients on warfarin undergoing 56 soft tissue procedures. 4 Of these patients, 10 were women with an average age of 78 years. INR values were not measured preoperatively. Patients did not experience any major hemorrhagic complications in the intraoperative or postoperative period. Although this study was not powered to draw statistically significant conclusions, the authors recommend that continuation of anticoagulation around soft tissue surgery is safe. 4
Otley and colleagues retrospectively reviewed more than 653 excisional and Mohs micrographic procedures to determine if there is increased risk with continuation or discontinuation of warfarin, aspirin, and nonsteroidal anti-inflammatory drugs in the setting of these procedures. 5 Similar rates of severe events were noted in patients continuing warfarin or antiplatelet therapy compared to control patients; the rates were not statistically different. No significant difference in incidence of severe events was noted in patients who had discontinued warfarin more than 2 days prior to the procedure. The authors concluded there is minimal risk of continuing warfarin for minor cutaneous surgery with the mention that discontinuation of warfarin prior to the procedure may result in the same bleeding complications. 5
Blasdale and Lawrence evaluated the frequency of hemorrhagic complications in patients on chronic warfarin therapy undergoing cutaneous surgery. 6 The primary outcome was frequency of postoperative bleeding. All patients on warfarin requiring basal cell carcinoma and squamous cell carcinoma excisions during a 3-year period were identified by the authors for inclusion in the study. Of the 65 patients included in the warfarin group, 26 were female with a median age of 69 years, with the indication of atrial fibrillation for approximately 64% of those treated with warfarin. The control group was matched for gender and size, site, and type of tumor. Of the 92 patients in the control group, 52 were female with an average age of 73.5 years. INR values were obtained preoperatively and on the day of surgery. INR values were made known to the surgeon 24 to 48 hours after the procedure. Bleeding was defined as normal if it was the expected degree of bleeding based on tumor site. Normal bleeding occurred in 90% of procedures in the warfarin group and 88% in the control group. Bleeding was defined as excessive if it required postoperative pressure dressings. Excessive bleeding occurred in 10% of the patients in the warfarin group and 12% in the control group. The results of this study indicate that there is no difference in intraoperative bleeding complications in patients taking warfarin compared to controls. However, 5 out of 65 patients taking warfarin experienced moderate or severe postoperative bleeding compared to none in the control group. All bleeding complications occurred with INR of <2.6, suggesting there is still risk of bleeding for surgical patients even if the INR is within therapeutic range. The average age of this population may not be representative of the average age of the patient seeking tattoo placement. 6
Kargi and colleagues prospectively evaluated 102 patients undergoing cutaneous surgeries with 37 patients using aspirin, 21 patients using warfarin, and 44 patients not on anticoagulant therapy. 7 The primary outcome was postoperative complications in patients taking warfarin and aspirin. Anticoagulation was not stopped prior to or after the procedure. Of the 21 patients taking warfarin, 9 patients were female with an average age of 68 years. Complications were grouped as minor, moderate, or major, with minor complications defined as persistent oozing and early dressing changes. Moderate complications were defined as postoperative bleeding; major complications were defined as persistent bleeding, wound hematoma, loss of skin graft, and wound infection. Of the patients receiving warfarin, there were a total of 12 bleeding complications. This was in comparison to a total of 6 complications in the control group (P value not provided), suggesting increased bleeding in the warfarin-treated patients. 7 No recommendations regarding perioperative INR measurement are mentioned in the article, nor is there any information regarding the indication for anticoagulation.
Syed and colleagues prospectively evaluated 47 anticoagulated patients to determine if there was a difference in bleeding risk in patients anticoagulated with warfarin undergoing Mohs micrographic surgery from March 2003 to February 2004. 8 The primary outcome was postoperative bleeding. Of the 55 patients who met the inclusion criteria, 47 patients were contacted at follow-up, with 8 patients excluded as they were lost to follow-up. INR values were checked intraoperatively, with 5 patients noted to have an INR >3.5. Minor bleeding was defined as bleeding relieved by pressure after discharge, with excessive bleeding defined as a hematoma or persistent bleeding unrelieved by pressure dressings or manual pressure. Minor bleeding occurred more frequently in the warfarin group as compared to the control group. 8 The article did not elucidate the indications for warfarin in the patients studied.
Billingsley and Maloney prospectively evaluated the incidence of postoperative bleeding complications in 81 patients taking aspirin, 12 patients taking warfarin, and 16 patients taking nonsteroidal anti-inflammatory agents undergoing Mohs micrographic surgery from October 1994 to May 1995. 9 The primary outcome was postoperative bleeding complications. There were 213 patients in the control group who had not taken anticoagulation prior to the procedure. Of the 8 patients who returned to clinic with oozing or bleeding, 1 was on warfarin, 2 were taking aspirin, and 5 were not taking anticoagulants. Although not defined, excessive bleeding was noted in 5 of the 12 patients taking warfarin, 1 of 16 patients taking aspirin, and 9 of 213 patients not taking any anticoagulants. Based on primary outcome, the authors conclude that there was no statistically significant difference in postoperative bleeding complications among the 3 anticoagulant agents. 9
Alcalay prospectively evaluated the impact of continued warfarin therapy during cutaneous surgery in 16 patients, with 5 patients undergoing excisional surgery and 11 patients undergoing Mohs surgery. 10 The primary outcome was perioperative bleeding. The average age of the warfarin-treated patient was 72 years, with the majority of patients anticoagulated with warfarin for the indication of atrial fibrillation. Gender was not reported. INR values were obtained in the warfarin-treated group 1 week prior to surgery. No bleeding was reported postoperatively by the patients in the warfarin group or the control group. The authors found no increase in postoperative bleeding in patients treated with warfarin. 10 This study did not note methodology for evaluating bleeding.
Bordeaux and colleagues prospectively evaluated hemorrhagic, infection, flap and graft necrosis, and dehiscence complications in patients undergoing cutaneous procedures who were anticoagulated with warfarin. 11 Of the 1911 patients included during the 15-month time period, 731 patients were on 1 anticoagulant or antiplatelet medication, 136 were on 2, 16 were on 3, and 1 patient was on 4 anticoagulant or antiplatelet medications. Anticoagulant medications were not discontinued prior to the surgery. Hemorrhagic complications occurred in 17 patients (0.89%). Patients on warfarin were found to have significantly higher risk of bleeding complications in comparison to patients undergoing cutaneous surgeries and were not taking warfarin; however, this study did not provide bleeding rates for patients receiving only warfarin in comparison to other anticoagulants. Noted bleeding complications did not require hospitalization. 11 The procedures evaluated in this study could be associated with a greater bleeding risk than simple cutaneous procedures and tattoo placement. Although this was one of the larger studies evaluating bleeding rates in patients undergoing cutaneous surgery and taking warfarin, the study did not evaluate INR values perioperatively and did not provide basic demographic information such as age and anticoagulant indication, which would be helpful for generalizability.
Sugden and Siddiqui prospectively examined the safety of warfarin continuation in minor cutaneous procedures. 12 The study included 51 patients, average age of 73 years, with an INR less than 4 prior to the procedure. The most common indication for warfarin was atrial fibrillation. Two patients experienced minor bleeding complications despite both patients having therapeutic INR values of 2.5 prior to the procedure. The classification of minor bleeding is unclear, although notably one patient’s sites healed without intervention whereas the other patient’s site healed by secondary intention. Although this study did not use statistical methods, the authors recommend that continuation of anticoagulation around minor cutaneous procedures is safe assuming that the patient’s INR is therapeutic on the day of surgery. 12
Thrombotic complications were evaluated by Kovich and Otley who surveyed 504 members of the American College of Mohs Micrographic Surgery and Cutaneous Oncology regarding thrombotic complications when anticoagulants were withheld. 13 Questions included in the survey sought to obtain information regarding the patient, procedure, indication and type of anticoagulant, and thrombotic complications. A total of 168 surveys were returned, which described 46 patients who met the inclusion criteria and were anticoagulated with warfarin, aspirin, or both. The average age of the patients was 73 years, with 28% of patients being female and the majority of patients being anticoagulated for an indication of stroke. Thrombotic events, which included 24 strokes, 3 cerebral emboli, and 1 retinal artery occlusion, occurred in 54% of patients when warfarin was withheld and in 39% of patients when aspirin was withheld. Hemorrhagic adverse events were not discussed. Given the thrombotic risk of withholding anticoagulation therapy perioperatively, the authors recommend continued use of anticoagulants. 13
Summary
Of studies involving use of warfarin in patients on chronic therapy undergoing minor cutaneous procedures, evidence is conflicting with regard to continuing warfarin throughout the procedure. In evaluating studies for cutaneous procedures, postoperative bleeding rate in the anticoagulated patient was statistically higher in 4 studies and, though not evaluated statistically, trended toward higher in 3 studies and was comparable in 3 studies. INR should be evaluated prior to procedures with delay if INR is elevated. Careful consideration of warfarin cessation is warranted due to increased thrombotic risk to the patient.
Discussion
A literature search was performed to evaluate data for anticoagulation management in the setting of tattoo placement for patients receiving chronic warfarin therapy and unfortunately was without result. As tattoo placement involves puncturing the skin to the dermal layer similar to minor cutaneous procedures, another search involving chronic warfarin therapy management in cutaneous procedures was performed. Four retrospective and 7 prospective trials were identified and are not without limitations. Studies were small in size, with most studies having less than 50 patients in the warfarin group. Study design was variant, with both retrospective and prospective trials, both controlled and noncontrolled. Indication for anticoagulation was seldom mentioned. Types of procedures performed varied between studies. Notably, bleeding evaluation was inconsistent, measuring various degrees of bleeding, both intraoperatively and postoperatively. INR evaluation also varied among the studies reviewed. Last, no studies were identified reviewing perioperative bridging strategies with short-acting anticoagulants. These limitations render the evidence inconclusive with respect to continuation of warfarin during cutaneous procedures.
Several considerations must be made in applying the evidence from cutaneous procedures to tattoo placement. Patients in the aforementioned studies were of an age greater than most seeking tattoo placement, which may affect bleeding and thrombotic risk. Tattoo placement may occur over larger areas of skin than the cutaneous procedures reviewed. Patients may not consider tattoo placement a significant procedure and may not notify the practitioner monitoring their anticoagulant. If the anticoagulant provider is notified of an upcoming tattoo placement, bleeding and thrombotic risks must be carefully weighed to determine the optimal plan for the patient. In preparation, pharmacists and other providers should counsel their patients on the importance of informing their tattoo artists of their concomitant administration of an anticoagulant if applicable. Patients should be informed that there may be an increased risk of bruising, bleeding, and for ink to run under the skin in the presence of bleeding. To enhance patient care, further trials evaluating chronic warfarin therapy and tattoo placement are warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.