
Abstract
Keywords
Background
Dexmedetomidine is a selective α2-adrenergic receptor agonist that is approved for “sedation of initially intubated and mechanically ventilated patients during treatment in an intensive care setting” and for “sedation of nonintubated patients prior to and/or during surgical and other procedures.” 1 Only 1 case report has been previously published on dexmedetomidine-induced hyperthermia. 2 According to the product information, in randomized placebo controlled trials, fever occurred in 5% of dexmedetomidine patients as compared to 4% in the placebo group. However, hyperpyrexia was reported in 2% of dexmedetomidine patients as compared to 3% in the placebo group. 1 According to the Food and Drug Administration (FDA), there has been several reports related to fever associated with dexmedetomidine, 2 which indicate that this is a rare reaction that needs to be brought to the attention of critical care practitioners.
Case Report
A 68-year-old male was transferred from a neighboring hospital to undergo diagnostic coronary angiography after experiencing a non-ST elevation myocardial infarction. The patient had no prior medical history and took no medications prior to admission. The coronary angiography revealed severe multivessel coronary artery disease. Left ventricular angiography showed severe left diastolic dysfunction with an ejection fraction of 20% to 25% and severe mitral regurgitation. The abdominal aortogram demonstrated an abdominal aortic aneurysm starting below the renal arteries into both iliac arteries. On hospital day 10, the patient underwent coronary artery bypass grafting of 3 vessels and mitral valve replacement. Postoperative medications are listed in Table 1, postoperative vital signs are listed in Table 2, and laboratory values are listed in Table 3. Initially, he did fairly well postoperatively and was extubated the day after surgery. The patient’s temperature increased to a maximum Foley temperature of 38.7°C, and a possible left lung infiltrate was seen on chest X-ray; therefore, he was started on ceftriaxone. However, on the second postoperative day (POD), the patient began to have increased respiratory distress and eventually went into shock (blood pressure was 77/41 mm Hg at 0530). He was intubated and started on propofol for sedation, and later that day, the sedation was switched to lorazepam and fentanyl infusions. He was started on norepinephrine for blood pressure support requiring a max of 0.8 µg/kg/min. The chest X-ray showed infiltrate versus edema. In addition, Infectious Disease (ID) was consulted. ID’s impression was possible systemic inflammatory response syndrome/septic shock and health care–associated pneumonia of the left upper lobe with multidrug-resistant risk factors; therefore, vancomycin, piperacillin/tazobactam, and levofloxacin were initiated on POD 2.
Medications.
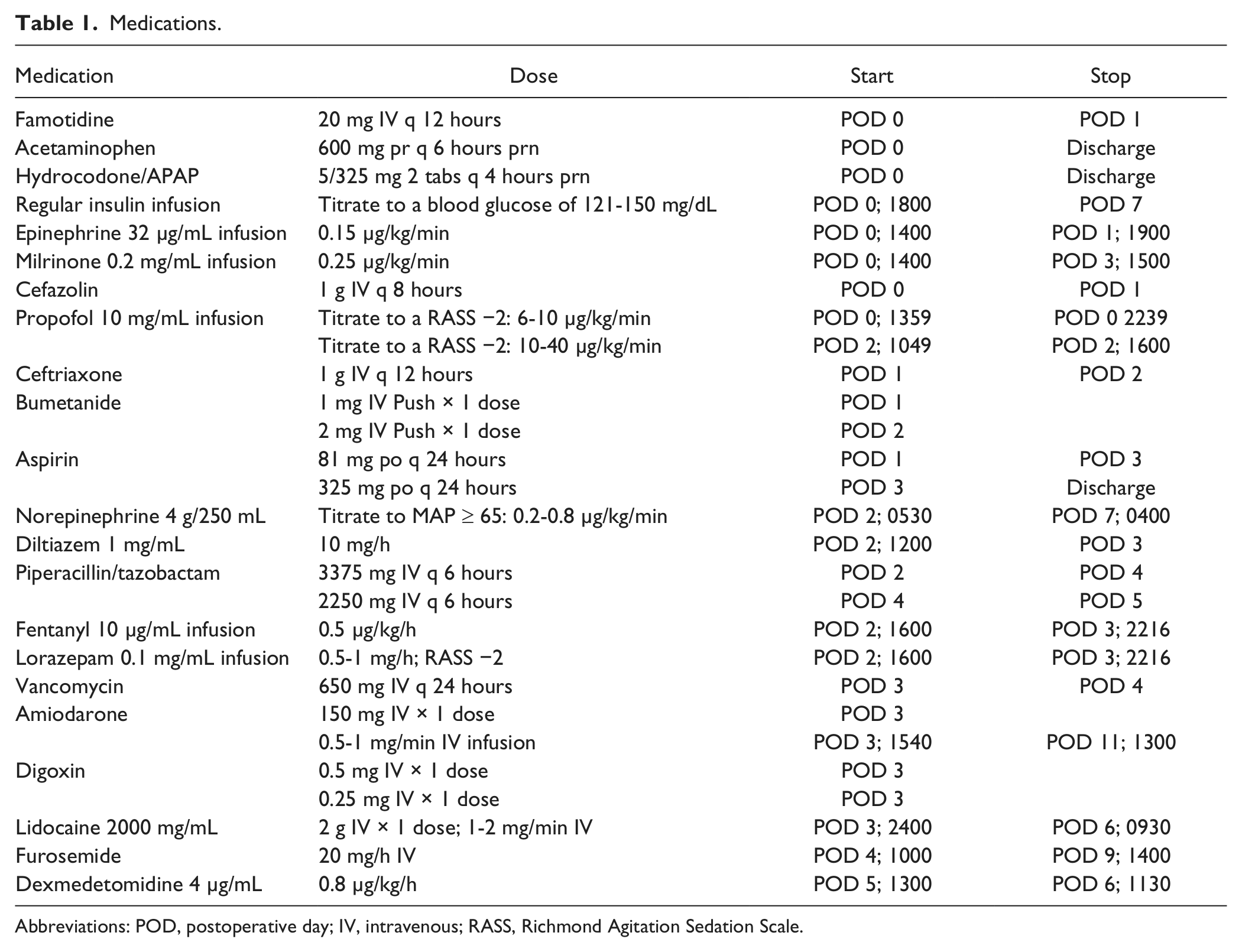
Abbreviations: POD, postoperative day; IV, intravenous; RASS, Richmond Agitation Sedation Scale.
Vital Signs.
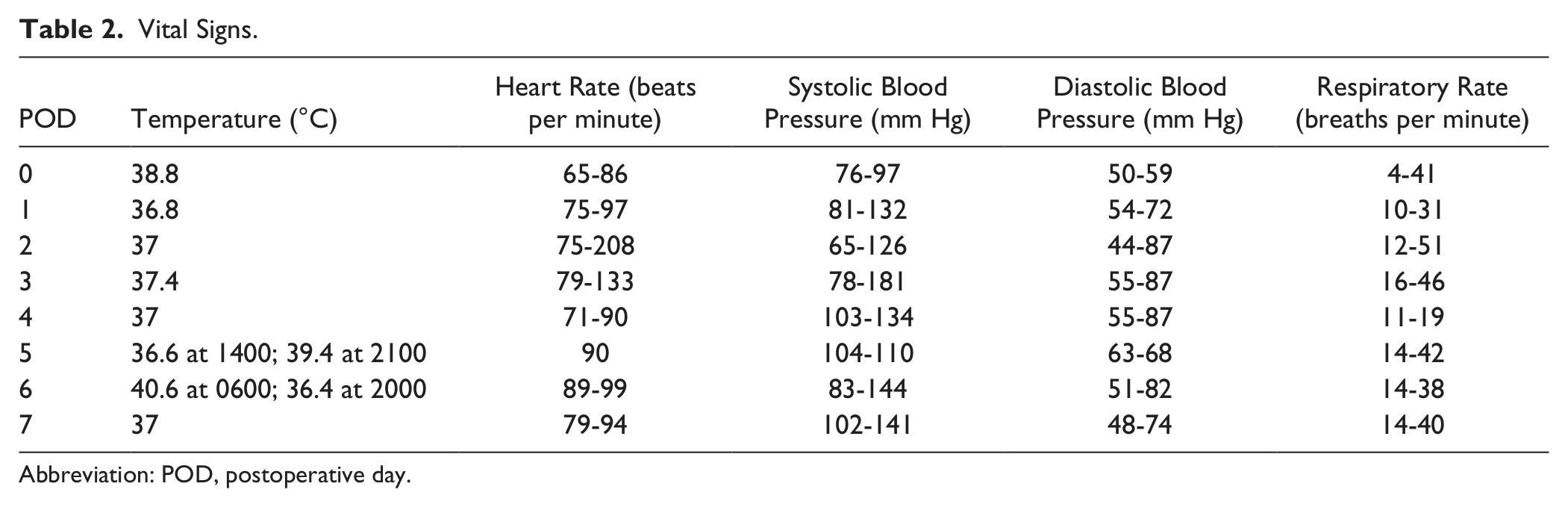
Abbreviation: POD, postoperative day.
Laboratory Values.
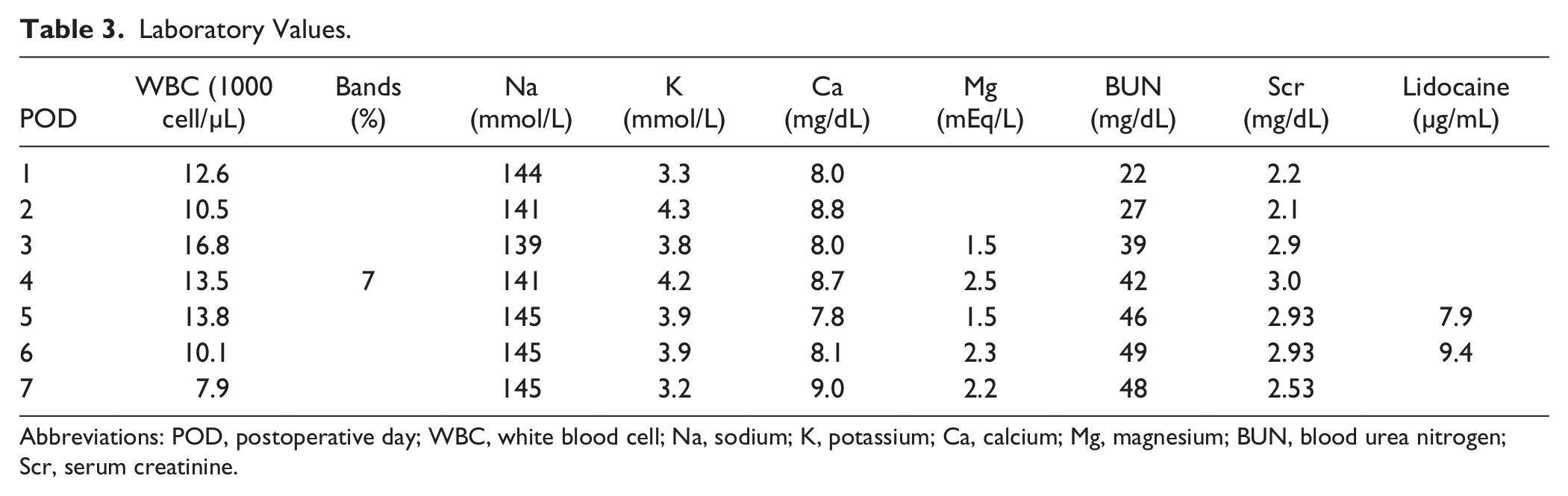
Abbreviations: POD, postoperative day; WBC, white blood cell; Na, sodium; K, potassium; Ca, calcium; Mg, magnesium; BUN, blood urea nitrogen; Scr, serum creatinine.
On POD 3, the patient went into atrial fibrillation and was started on an amiodarone drip. He went into ventricular fibrillation 3 times during the night, which led to the patient being defibrillated at 2216, 2351, and 0354 on POD 4. Subsequently, he was started on a lidocaine drip at 2400 after the second arrest. Lorazepam and fentanyl were discontinued. On POD 4, the patient’s overall condition began to improve. Since the blood, urine, sputum, and blind bronchial lavage culture results were all negative and the Legionella DFA and culture were negative, ID felt that he most likely did not have an infection; therefore, vancomycin and levofloxacin were discontinued, and piperacillin/tazobactam was discontinued on POD 5. In addition, on POD 5, dexmedetomidine hydrochloride was initiated at 1300 for sedation. At initiation of the drip, the patient’s axillary temperature was 36.8°C; however, at 2100, the first temperature measured after starting dexmedetomidine, he developed an oral temperature of 39.4°C, and he became very unresponsive and flaccid. On POD 6, at 0500 his oral temperature rose to 40.5°C, and he was packed in ice and given acetaminophen suppository. The patient’s peak temperature was 40.6°C at 0600. At 0900, his temperature remained elevated at 39.7°C; subsequently, lidocaine was discontinued by the physician at 0930.
Dexmedetomidine was discontinued at 1130, and consequently his temperature rapidly decreased from 39.2°C to 38.4°C within 2 hours. A cooling blanket was applied at 1200; however, it was discontinued 2 hours later, since the patient’s temperature improved. Creatine kinase and thyroid function tests were ordered, which indicated the following: creatine kinase level 260 units/L, thyroid-stimulating hormone 1.4 mU/L, free T4 0.83 ng/dL, and free T3 1.4 pg/mL. An electroencephalogram (EEG) was ordered to rule out seizures. The EEG revealed encephalopathy and no signs of seizures. The next temperature, measured rectally at 1900, was 36.4°C, and the patient began opening his eyes to voice commands. With the discontinuation of dexmedetomidine, the patient’s overall condition improved without further temperature increases. The patient was never restarted on dexmedetomidine or lidocaine (Figure 1).
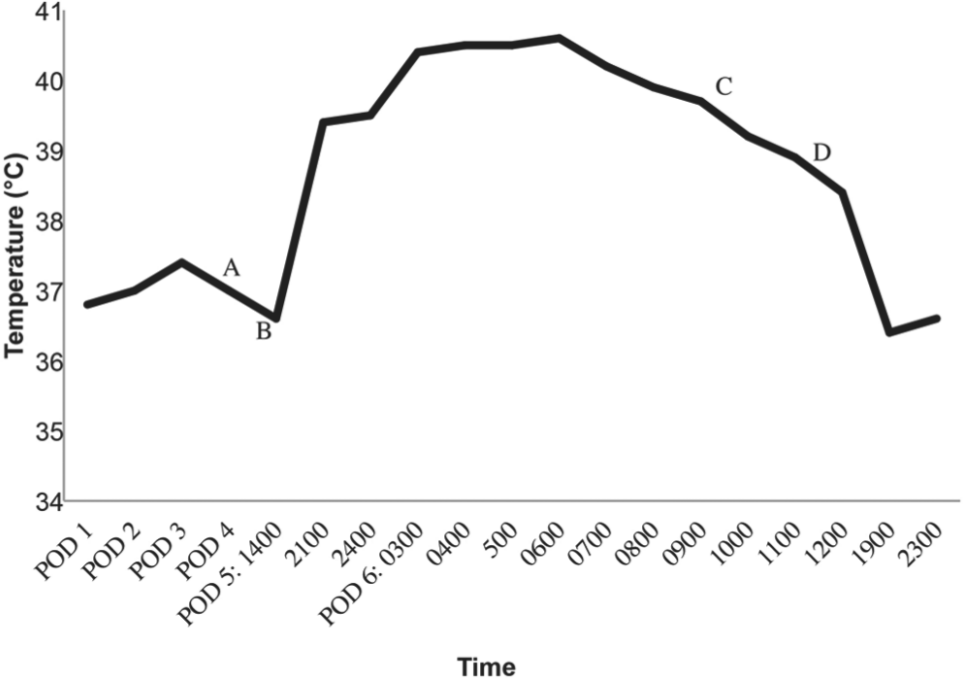
Temperature in response to dexmedetomidine.
The patient remained in the hospital for 2 more weeks. During these few weeks he developed paroxysmal atrial fibrillation, which was treated with amiodarone and metoprolol. Unfortunately, he developed tachybrady syndrome and ultimately had a pacemaker placed. In addition, the patient experienced a left-hemispheric ischemic stroke with right-sided weakness on POD 16. On discharge to a rehabilitation facility, the patient was alert and able to follow commands; however, he continued to have right upper extremity weakness.
Discussion
In this patient, the cause of his fever was not clear. All cultures remained negative, and although the possibility of infection was initially considered when he had a change in his condition postoperatively, all cultures remained negative and antibiotics were discontinued 2 days later by our ID specialist. He did not have apparent seizure activity, and his EEG did not show evidence of seizures. Thyroid function studies were obtained as hyperthyroidism can cause fevers, and there are reports in the literature of amiodarone-induced thyroidtoxicosis. 3 However, his thyroid function studies remained normal.
Drug-induced hyperthermia fall into 7 categories: (a) adrenergic fever (eg, cocaine exposure), (b) anticholinergic fever (eg, atropine, antihistamines, psychotropic medications, etc), (c) antidopaminergic fever (eg, neuroleptic malignant syndrome or withdrawal of anti-Parkinsonian medication), (d) serotonin syndrome (eg, serotonin reuptake inhibitors), (e) malignant hyperthermia from anesthetics and depolarizing muscle relaxants, (f) uncoupling of oxidative-phosphorylation such as phencyclidine or salicylate overdose, and (g) baclofen withdrawal. 4 Other than fentanyl, our patient was not exposed to any agents associated with serotonin syndrome. Because his operation and exposure to anesthetics was several days before the onset of fever, malignant hyperthermia induced by those agents is unlikely. We did find one case report of malignant hyperthermia induced by lidocaine, 5 and the patient was receiving lidocaine when the fever developed. However, his measured creatine kinase was only slightly elevated, and he did not have muscle rigidity, which would argue against malignant hyperthermia. His high lidocaine levels most likely contributed to the change in his mental status, but because of the rapid increase in temperature after initiation of dexmedetomidine, we suspect that dexmedetomidine is the more likely cause of the high temperature.
Through a Medline literature search using the terms dexmedetomidine, fever, or hyperpyrexia, we found one published case report from the Department of Anesthesiology and Intensive Care Medicine, Tokyo, Japan. 2 In this report, similar to ours, high fevers (40.6°C) developed rapidly after starting dexmedetomidine and improved 7 hours after stopping dexmedetomidine.
As previously mentioned, fever is listed in the manufacturer’s information as a possible adverse reaction occurring in 5% of dexmedetomidine patients as compared to 4% of those receiving placebo. 1 However, fever was not reported as an adverse reaction in large-scale comparative trials of dexmedetomidine for ICU sedation.6,7
Although lidocaine and dexmedetomidine were stopped within hours of each other, we feel the most likely cause of the fever was dexmedetomidine, as the patient was afebrile prior to starting dexmedetomidine while on lidocaine, but because we cannot rule out the possibility of lidocaine as a cause, we would rate the reaction as a “possible” adverse reaction by the Naranjo scale (score 3). 8
Through the Freedom of Information Act, we obtained dexmedetomidine adverse reaction reports submitted to the Food and Drug Administration, and we found 9 reports that listed dexmedetomidine as the primary suspected cause of adverse reactions that included fever, hyperpyrexia, or increased body temperature as a part of the reaction. Table 4 summarizes these reports.
FDA Reports of Fever/Hyperpyrexia With Dexmedetomidine.
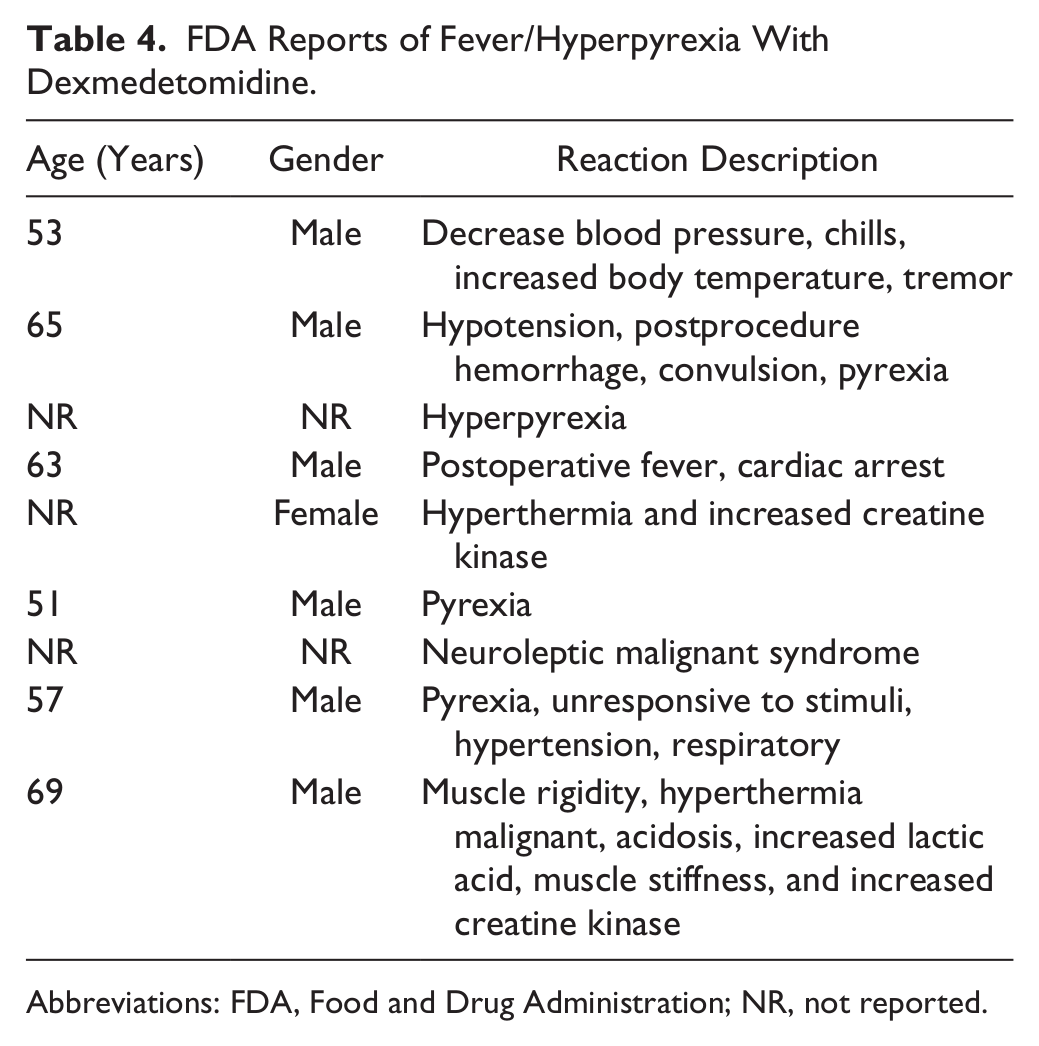
Abbreviations: FDA, Food and Drug Administration; NR, not reported.
Summary
We report a case of a patient who developed a high fever after the initiation of dexmedetomidine. There is one previous published case report in the literature with similarities to ours, as well as several reports to the FDA that indicate that this may be an infrequent reaction that physicians should be aware of and consider in the differential diagnosis of patients who develop fever in the intensive care unit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.