
Abstract

Mesenteric ischemia due to arterial embolic occlusion can result in bowel necrosis requiring bowel resection. 1 Short bowel syndrome can result, requiring long-term total parenteral nutrition (TPN). 1 Long-term anticoagulation to reduce risk of future embolic events is recommended; however, some question whether oral anticoagulants will be absorbed given short bowel syndrome, and thus, whether long-term parenteral anticoagulation would be more appropriate. In this article, we describe a case in which a patient with 45 cm of small bowel remaining after bowel resection for mesenteric ischemia achieved stable, therapeutic treatment with warfarin.
A 65-year-old man was admitted to hospital for a 2-day history of severe nausea, vomiting, and abdominal spasms. He reported 9.1 kg weight loss and nonbloody diarrhea over the course of the previous month. Imaging revealed ischemic bowel and an occluded superior mesenteric artery. He was found to have infarcted bowel from the jejunum to the right colon. The distance from the ligament of Treitz to the distal-most part of bowel where the ischemia began was 45 cm. A small bowel resection and right hemicolectomy were performed; later, an ileocolonic functional end-to-end anastomosis was performed.
The patient was anticoagulated with continuous intravenous (IV) heparin immediately following his surgeries, targeted to therapeutic activated partial thromboplastin time. Investigations to determine the etiology of arterial occlusion identified atrial flutter, suggesting a cardioembolic source. Warfarin therapy was initiated on June 15, and bridged to therapeutic international normalized ratio (INR) with IV heparin. The patient’s course on warfarin is depicted in Figure 1. Although there were initial concerns of poor warfarin absorption, the lack of response to warfarin was subsequently attributed to a combination of conservative warfarin dosing and co-administration of vitamin K 2 mg IV every Wednesday in his TPN. Once the TPN was changed to daily IV vitamin K 0.2 to 0.3 mg and the warfarin total weekly dose adjusted to 45.5 mg orally, he achieved a time in therapeutic range of 83% using the Rosendaal method. 2 Unfortunately, despite therapeutic INRs, an upper extremity catheter-associated venous thromboembolism was identified on August 10, and the patient was switched to daily subcutaneous dalteparin.
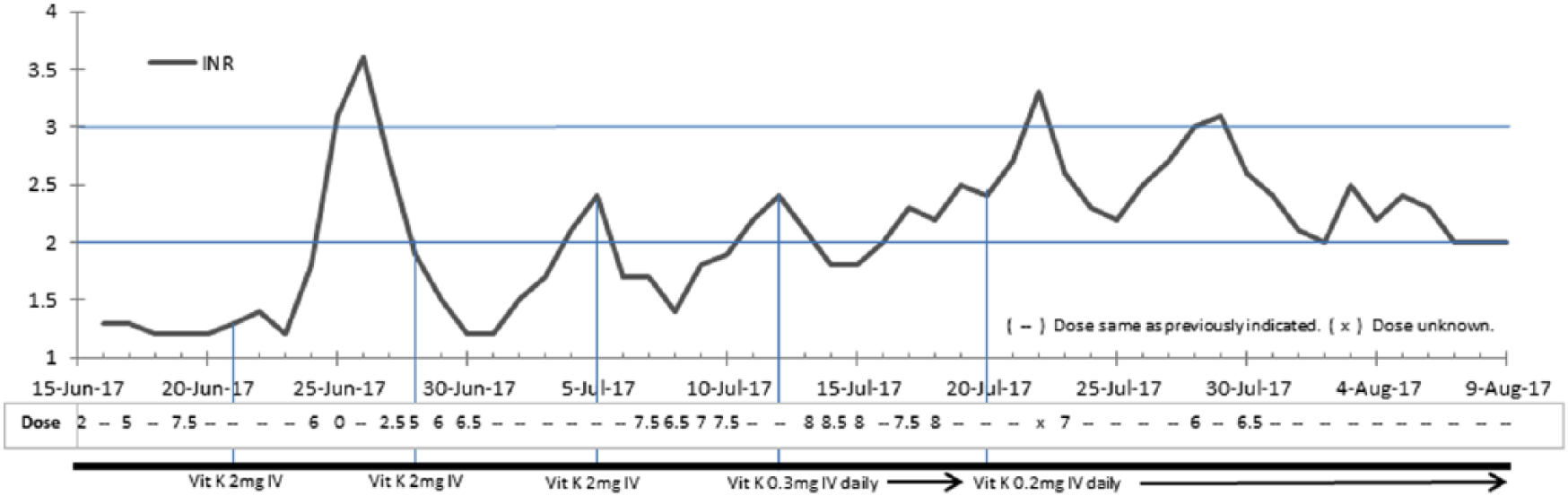
Patient’s course on warfarin therapy.
Despite no apparent direct studies of the site of warfarin absorption, several case series 3 indicate that it is absorbed extensively in the stomach and proximal small intestine, yet doubts about its effectiveness in short bowel syndrome have been expressed. Our case supports the conclusion by Owens et al 3 that a series of patients with short bowel syndrome can absorb warfarin, though it should be noted that all of the reported successful cases had an intact stomach. Several published cases demonstrate warfarin resistance after loss of gastric tissue, including Brophy et al, 4 who describe a case of proposed poor absorption due to total duodenectomy with loss of gastric tissue for a gastrojejunostomy, and Sobieraj et al, 5 who describe a case of warfarin resistance after complete gastric resection and Roux-en-Y gastric bypass. In contrast, Strong et al 6 found an overall increased warfarin sensitivity after Roux-en-Y gastric bypass. This phenomenon may result from substantially reduced postoperative intake of vitamin K–containing foods, 6 but seems to support a trial of warfarin therapy despite surgery involving the gastric tissue.
Advantages of oral anticoagulation over injectable include lower cost and avoidance of needle-stick pain. If using warfarin, one must consider vitamin K in TPN and/or lipids, which may be the cause of INR variations if not appropriately managed.3,7 Alterations to the gut microbiota can result in impaired bacterial vitamin K synthesis, 6 but are likely clinically insignificant if receiving TPN. Warfarin has an advantage over the direct oral anticoagulants due to the ability to monitor efficacy via the INR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.