
Abstract
Keywords
Introduction
On December 31, 2019, a pneumonia of unknown cause detected in Wuhan, China, was first reported to the World Health Organization (WHO). 1 On January 7, 2020, Chinese health authorities confirmed that this was associated with a novel coronavirus, 2019-nCoV. 2 On January 20, 2020, the first confirmed case of 2019-nCoV infection was reported in the United States. 3
On February 11, 2020, an official name for the disease associated with the novel coronavirus first identified in Wuhan, China, was announced by the WHO. The official names of this disease are “COVID-19” and “coronavirus disease.” 4
The name of this disease was selected according to the WHO guidelines for naming of new human infectious diseases. 5 According to the WHO, in the name COVID-19, “CO” stands for “corona,” “VI” for “virus,” and “D” for disease, 6 with “19” as reference to the year when identified, 2019.
The disease COVID-19 is caused by a coronavirus officially named “severe acute respiratory syndrome coronavirus 2” or “SARS-CoV-2.” 4 The name of the virus has also been referred to as “2019 novel coronavirus” or “2019-nCoV,” which appears in the medical literature. 6 WHO may refer to the virus as “the virus responsible for COVID-19” or “the COVID-19 virus” when communicating with the public. 4
Several types of human coronaviruses exist, which may include those that commonly cause mild upper respiratory tract illnesses. COVID-19 is a new disease, caused by a new (or novel) coronavirus not previously identified in humans. 7
Considerable attention has been focused on the pathogenesis, morbidity and mortality, and treatment of COVID-19. Since the outbreak began, medical researchers have been working at a rapid pace for an effective treatment against the novel coronavirus. Currently, there is no vaccine for use as a preventative for COVID-19, and the most effective way to prevent illness is to avoid being exposed to this virus, which is known to spread through person-to-person contact. 8 Practical measures to achieve this include, but are not limited to, frequent handwashing, avoiding close contact and maintain social distancing of at least 6 feet with other people, and use of a mouth and nose covering such as a mask when around others. Detailed preventative measures for coronavirus infection are provided by the Centers for Disease Control and Prevention. 8
At the time of this writing, there are no drugs or other therapeutics approved by the US Food and Drug Administration (FDA) to prevent or treat COVID-19. 9 However, the drug remdesivir has shown considerable promise as a treatment for patients to accelerate recovery from advanced COVID-19. 10
Although not approved by the FDA, on May 1, 2020, the FDA issued an Emergency Use Authorization (EUA) for remdesivir. 11 The EUA is supported by a Secretary of Health and Human Service (HHS) declaration that “circumstances exist to justify the emergency use of drugs and biological products during the COVID-19 pandemic.” 12
Remdesivir is authorized for the treatment of hospitalized patients with severe COVID-19 disease, and the EUA allows for the distribution and emergency use of remdesivir for the treatment of COVID-19. 11 The EUA enables select patients to access remdesivir more readily due to the public health emergency. Specifically, the EUA facilitates use of remdesivir to treat hospitalized patients with severe COVID-19 disease, by enabling access to remdesivir at additional hospitals across the United States.
As remdesivir has not been approved by the FDA for sale and marketing, the safety, efficacy, and optimal duration of treatment of remdesivir for the treatment of COVID-19 has not been established and are being studied in ongoing clinical trials. 13
Recently, the biopharmaceutical company Gilead Sciences, Inc, has submitted a New Drug Application (NDA) to the US FDA for remdesivir under the name Veklury. 13 According to the FDA, “the NDA application is the vehicle through which drug sponsors formally propose that the FDA approves a new pharmaceutical for sale and marketing in the United States.” 14
This is a review of the investigational drug remdesivir and its therapeutic potential for treatment of COVID-19, in the form of a series of questions and answers.
From June 2020 to August 2020, we conducted comprehensive searches of MEDLINE-PubMed, Scopus, and Google Scholar databases with no time limitations. The search terms included were “remdesivir,” “COVID-19,” “novel coronavirus” and “evidence,” “therapy,” “safety,” “effectiveness,” “efficacy,” “clinical trial.”
The sources of information include all publicly available data from previously published research reports. Reports must have at least one reference to remdesivir as a treatment modality for COVID-19 with no specified outcomes.
The purpose of the review is to narrow gaps in knowledge, clarify concepts, and to investigate research advancements for health care professionals. The answers have been formulated based on the latest available evidence in published literature.
What Is Remdesivir?
Remdesivir is an investigational drug used to treat viral infections. It is classified as a broad-spectrum antiviral with potential antiviral activity against a variety of RNA viruses. 15 It has emerged as a primary drug treatment option, and according to Dr Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, remdesivir may be considered a new “standard of care” for COVID-19. 16
How Does Remdesivir Work?
Remdesivir works against the novel coronavirus by inhibiting replication of the virus in the body. 17 This process takes place by interfering with the novel coronavirus’s RNA polymerase, an enzyme needed to copy a DNA sequence into an RNA sequence during the process of transcription.17,18
Remdesivir functions as a prodrug that is modified in the body before it becomes an active drug. 15 It is classified as a nucleoside analog, one of the oldest classes of antiviral drugs, and resembles the RNA base adenosine. 19 In general, nucleoside and nucleotide analogues simulate the structure of a true nucleoside or nucleotide. The simulated structure may then be incorporated into the virus; and in this sense may be considered a “counterfeit” agent—with therapeutic benefit. 20 Remdesivir works when the enzyme replicating the genetic material for the novel coronavirus—RNA polymerase—incorporates the adenosine analogue in place of the natural molecule into the growing RNA strand. By introduction of the modified agent remdesivir, replication of the novel coronavirus is interrupted, and the virus ceases to multiply and is not able to infect more cells in the body. 19
Who Developed Remdesivir? When Was It Developed?
Remdesivir was developed by Gilead Sciences, Inc, a research-based biopharmaceutical company with headquarters located in Foster City, California, near San Francisco. 21 A major focus of research programs at Gilead is antiviral drug therapy. 22
The research that led to the development of remdesivir began as early as 2009, during the time of Gilead’s antiviral research programs investigating hepatitis C and respiratory syncytial virus. 23 Following its discovery, Gilead continued to explore various uses for remdesivir.
In 2014, when the Ebola outbreak was spreading in West Africa, remdesivir was studied for treatment of Ebola virus disease but was unsuccessful. 24
Remdesivir demonstrated in vitro and in vivo activity in animal models against the viral severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) pathogens, which are also coronaviruses structurally similar to COVID-19. 15
In January 2020, Gilead began laboratory testing of remdesivir against SARS-CoV-2, with the limited preclinical data on remdesivir in MERS and SARS indicating potential activity against COVID-19. 24
What Dosage Forms Are Available for Remdesivir?
Remdesivir is supplied in 2 different injectable dosage forms: remdesivir for injection 100 mg lyophilized powder and remdesivir injection 5 mg/mL concentrated solution. 25
Supplies of remdesivir have been limited, and since January 2020, Gilead has invested significant capital to establish a supply chain capable of large-scale production of remdesivir. 24
On June 13, 2020, it was announced that the pharmaceutical company Dr Reddy’s Laboratories Ltd has entered into a nonexclusive licensing agreement with Gilead Sciences Inc. This gives the company the right to register, manufacture, and sell remdesivir in 127 countries including India. 26
What Is the Recommended Dosing and Administration for Remdesivir?
The optimal dosing and duration of remdesivir for the treatment of COVID-19 has not been determined. 27 Remdesivir is not taken orally and is not available in a capsule or tablet form, nor should it be administered intramuscularly. Remdesivir is only administered intravenously (IV) in a hospital setting under the care of a physician. 27
The following is the recommended method of preparation of remdesivir for intravenous administration. 25
Remdesivir for injection, 100 mg: reconstitute remdesivir for injection lyophilized powder with 19 mL of sterile water for injection and dilute in 0.9% saline prior to administration.
Remdesivir injection, 5 mg/mL: dilute remdesivir injection concentrated solution in 0.9% saline prior to administration. Prepare solution for infusion on same day as administration.
Remdesivir is to be administered via intravenous infusion in a total volume of up to 250 mL 0.9% saline over 30 to 120 minutes for adult patients. 27
After infusion is complete, flush with at least 30 mL of 0.9% saline.
Discard any remaining reconstituted remdesivir lyophilized powder, reconcentrated solution, and diluted solution.
The dose under investigation for treatment of COVID-19 is 200 mg IV on day 1 followed by 100 mg IV daily as a 5-day or 10-day treatment course. 28
Gilead Pharmaceuticals provides a pharmacy guide with frequently asked questions, 29 which includes information on storage, stability, and special requirements on preparation and administration for pharmacists and other health care professionals. The guide may be accessed at https://www.remdesivir.com/us/downloads/remdesivir_pharmacy_guide.pdf. 29
What Is the Evidence of Effectiveness of Remdesivir for COVID-19?
At the time of this writing, the evidence for effectiveness of remdesivir as a treatment for COVID-19 is inconclusive, yet trends indicate positive outcomes on certain indicators, such as shortening the disease course and/or severity of illness. Literature searches conducted by the authors reveal a mix of direct and indirect evidence for remdesivir alone or in combination with other drugs. Reports include randomized control trials with limitations, observational reports, case series studies, and case reports (Table 1).
Reports on Remdesivir for Treatment of COVID-19 (in Chronological Order).
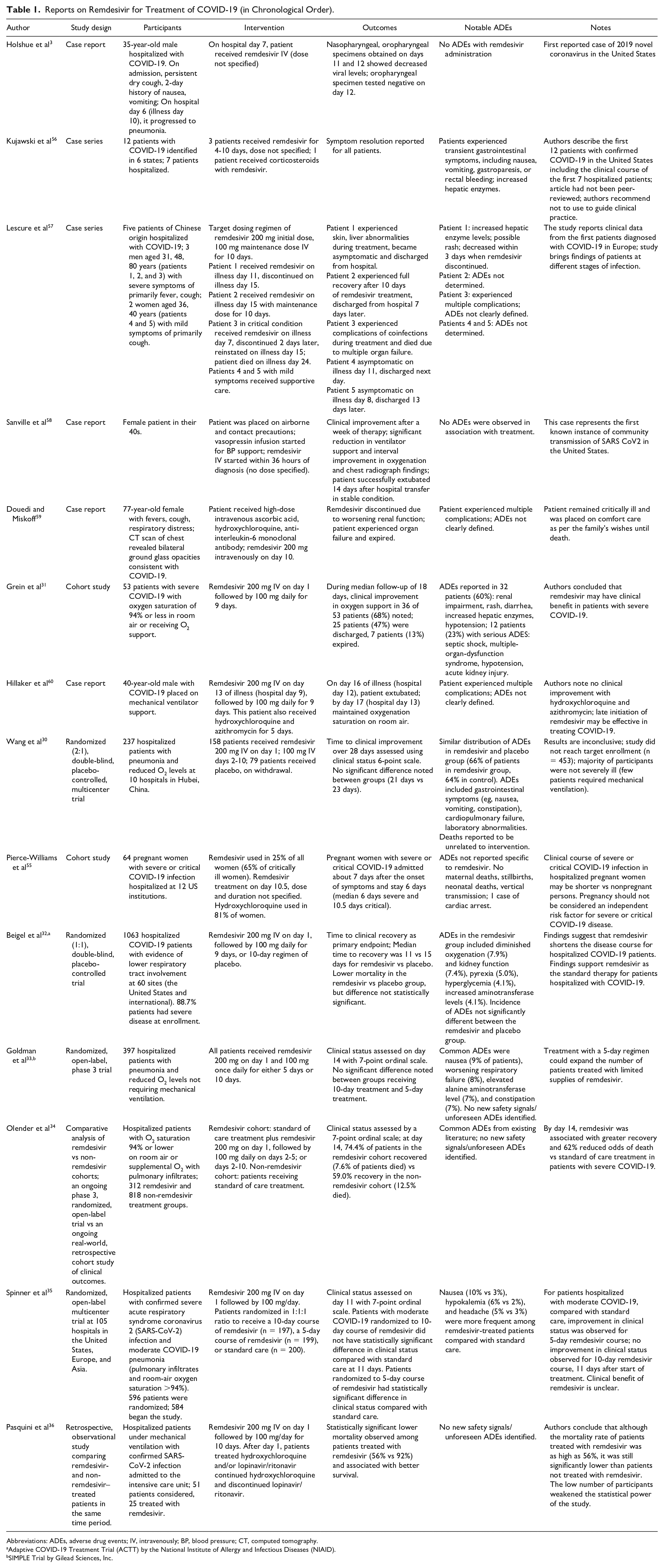
Abbreviations: ADEs, adverse drug events; IV, intravenously; BP, blood pressure; CT, computed tomography.
Adaptive COVID-19 Treatment Trial (ACTT) by the National Institute of Allergy and Infectious Diseases (NIAID).
SIMPLE Trial by Gilead Sciences, Inc.
While clinical trials on remdesivir treatment for COVID-19 have shown promising results for efficacy and effectiveness, often studies are limited to patients in specific clinical contexts. A brief summary of the findings for the major clinical studies are described below.
Wang et al reported the first double-blind placebo-controlled trial of remdesivir in adults in China admitted to the hospital with severe COVID-19. 30 One hundred fifty-eight patients were randomized to remdesivir and 78 to placebo, and results indicate that remdesivir was not associated with statistically significant clinical benefits. Post hoc analysis of the subgroup of patients enrolled within 10 days of symptom onset found shorter median time to improvement with remdesivir than with placebo. The authors recommend that findings require confirmation in larger studies.
Grein et al conducted a cohort study involving 53 patients in the United States, Europe, Canada, and Japan. 31 Patients were hospitalized for severe COVID-19 with an oxygen saturation of 94% or less in room air or receiving oxygen support. During a median follow-up of 18 days, clinical improvement in the level of oxygen support needed was observed in 36 patients (68%) including 17 of 30 patients (57%) receiving mechanical ventilation who were extubated. The authors concluded that measurement of efficacy will require ongoing randomized, placebo-controlled trials of remdesivir therapy.
Beigel et al reported preliminary analysis of data from the 1063-patient ACTT-1 randomized, double-blind, placebo-controlled trial in adults hospitalized with COVID-19. 32 Patients with evidence of lower respiratory tract involvement (88.7% patients had severe disease at enrollment) were randomly assigned to receive either remdesivir or placebo for up to 10 days. It was observed that patients who received remdesivir had a median recovery time of 11 days as compared with 15 days in those who received placebo, an improvement in recovery time in the overall study population by 4 days. The authors concluded that remdesivir was superior to placebo in shortening the time to recovery in adults hospitalized with COVID-19 with evidence of lower respiratory tract infection.
Goldman et al reported on the SIMPLE-1, randomized, open-label, phase 3, Gilead-sponsored trial. 33 The study compared 5- and 10-day remdesivir courses in 397 hospitalized patients with pneumonia and reduced oxygen levels not requiring mechanical ventilation (oxygen saturation at or below 94% on ambient air or requiring supplemental oxygen). The study found no difference between the 5- and 10-day courses in 14-day clinical status improvement on a 7-point ordinal scale. The authors concluded that the longer course did not significantly improve time to clinical improvement, time to recovery, or death. The significance of the study reveals that with limited supplies of remdesivir, treatment with a shorter, 5-day regimen could expand the number of patients treated.
Olender et al conducted a comparative analysis of remdesivir versus standard-of-care treatment in adults with severe COVID-19. 34 Data were analyzed in 2 parts: on 312 patients from a phase 3 remdesivir trial, and a retrospective cohort of 818 patients with severe COVID-19 treated with standard-of-care. The primary endpoint was the proportion of patients with recovery on day 14, and a key secondary endpoint was mortality. The authors observed that in patients with severe COVID-19, by day 14, remdesivir treatment was associated with a greater degree of recovery and reduced odds of death versus standard-of-care treatment.
Spinner et al assessed the efficacy of a 5-day and 10-day remdesivir treatment course compared with standard care in patients with moderate COVID-19. 35 A randomized, open-label trial of 584 patients was conducted in 105 hospitals in the United States, Europe, and Asia. Results indicate that compared with standard care, a 5-day course of remdesivir had a statistically significant difference in clinical status versus standard care, but the difference was of uncertain clinical importance. A 10-day course or remdesivir was not associated with a statistical difference compared with standard therapy.
Pasquini et al analyzed data collected retrospectively on hospitalized patients with severe COVID-19 with respiratory failure on mechanical ventilation in an intensive care unit (ICU). 36 Data on 51 patients were analyzed, of which 25 were treated with remdesivir for 10 days. The study group was composed of patients treated with remdesivir, and patients not treated with remdesivir were considered the control group. Statistical analyses indicated lower mortality among patients who had been treated with remdesivir. The authors concluded that the use of remdesivir was associated with a significant beneficial effect for patients on survival; however, the relatively low number of participants weakened the statistical power of the study.
In addition, several clinical trials have been registered in the United States and globally.15,37,38 (Clinical trial registration is the practice of documenting clinical trials in a clinical trials registry before they are performed.) 39 Definitive determination of efficacy and safety will require ongoing randomized, placebo-controlled trials of remdesivir therapy.
What Is Remdesivir’s Indication for Use?
At the time of this writing, remdesivir is an investigational drug and does not have an official FDA-approved indication. 13 Largely based on early research reports that revealed promising results for remdesivir as a treatment for COVID-19, it has been referred to as “standard therapy” for patients hospitalized with COVID-19 requiring supplemental oxygen therapy. 40
Based on the FDA’s initial EUA, remdesivir is to be used in patients with suspected or laboratory-confirmed COVID-19, which includes adults and children hospitalized with severe disease. Severe disease is defined as patients with an oxygen saturation (SpO2) of 94% or less on room air, requiring supplemental oxygen, requiring mechanical ventilation, or requiring extracorporeal membrane oxygenation (ECMO). 41
On August 28, 2020, as part of ongoing efforts to fight COVID-19, the FDA expanded the EUA for remdesivir. The scope has been broadened to include treatment of all hospitalized adult and pediatric patients with suspected or laboratory-confirmed COVID-19, irrespective of their severity of disease. 42
The National Institutes of Health (NIH) have published treatment guidelines to inform clinicians on how to care for patients with COVID-19. 43 Guided by a panel of experts (referred to as “the Panel”), the recommendations in the guidelines are based on expert opinion and scientific evidence, which includes the findings of several clinical trials investigating remdesivir as a treatment option for COVID-19. 44
The use of remdesivir for patients with COVID-19 may vary depending on the patient’s condition and clinical context of the patient’s care. What follows are recommendations for the use of remdesivir based on the opinion of the Expert Panel.
For patients with mild or moderate COVID-19, there are insufficient data to recommend either for or against the use of remdesivir to treat patients.
In hospitalized patients with COVID-19 who require supplemental oxygen, clinical judgement is needed, and the use of remdesivir should be prioritized, because supplies may be limited (recommendation level BI).
For hospitalized patients who require supplemental oxygen, but do not require oxygen therapy through a high-flow device, noninvasive or invasive mechanical ventilation, or ECMO, remdesivir is recommended for 5 days or until discharge from the hospital, whichever comes first (recommendation level AI).
If a patient who is on supplemental oxygen while receiving remdesivir progresses to high-flow oxygen therapy, noninvasive or invasive mechanical ventilation, or ECMO, the course of remdesivir should be completed.
For patients who require oxygen delivery through a high-flow device, noninvasive or invasive mechanical ventilation, or ECMO, the Panel does not make a recommendation either for or against starting remdesivir, due to uncertainty whether starting remdesivir confers clinical benefit in these patients.
For patients with COVID-19 who have not shown clinical improvement after 5 days of therapy, there are insufficient data on the optimal duration of remdesivir therapy; some experts recommend extending the total remdesivir treatment duration to up to 10 days (recommendation level CIII).
The complete COVID-19 treatment guidelines may be viewed on the NIH’s website. 44 In addition, an explanation of the rating system with representative codes for recommendations and evidence may be found on the NIH’s website. 45
What Are the Contraindications for the Use of Remdesivir?
Remdesivir is contraindicated for any patient with known hypersensitivity to any product ingredient. 25 The inactive ingredients of remdesivir include sulfobutylether-β-cyclodextrin sodium salt (SBECD), Water for injection USP, and may include hydrochloric acid and/or sodium hydroxide for adjusting pH. 25 SBECD is used in the formulation as a solubilizing agent due to the limited aqueous solubility of remdesivir. 46 As a potential contraindication, SBECD is renally excreted and patients with moderate or severe renal impairment may have SBECD exposures. 46
Reference has been made of a contraindication on initiating remdesivir therapy with concomitant use of vasopressors,
46
but the clinical implications are not clear. According to the European Medicines Agency, The current contraindication on starting remdesivir therapy concomitant vasopressors use is based on this being an indication of end organ failure, where there are no safety data. However, the use of vasopressor at low/medium doses for inotropic support due to the use of sedation and paralytics while on the ventilator is allowed. On the other hand, once a patient initiates treatment with remdesivir, subsequent use of pressors is not a reason for discontinuation of remdesivir.
47
Evidence is scant regarding this aspect of remdesivir in therapy and until more evidence is presented, caution is warranted by clinicians when drawing conclusions on the role of vasopressors and the use of remdesivir.
Can Remdesivir Be Used in Patients With Renal Impairment?
Based on current information, no specific studies have been conducted with remdesivir in use patients with renal impairment.46,47 Patients with estimated glomerular filtration rate (eGFR) ≥30 mL/min have received remdesivir for treatment of COVID-19 with no dose adjustment. 25
According to the FDA’s Fact Sheet for Health Care Providers, remdesivir is not recommended in adult and pediatric patients (>28 days old) with eGFR <30 mL/min. This also applies to full-term neonates (≥7 days to ≤28 days old) with serum creatinine ≥1 mg/dL unless the potential benefit outweighs the potential risk. 25
Sing et al assert, A close look on eGFR is necessary while administrating remdesivir, especially in patients with known renal impairment and discontinuation is required if eGFR falls to 50% from baseline. Although the parent compound remdesivir has only minor renal excretion, but since urine is found to have 49% of its metabolite GS-441524, impaired renal impairment may theoretically increase plasma exposure to this metabolite. Nevertheless, given the benefit-risk ratio in patients with COVID-19, no dose modification is currently recommended in patients with mild and moderate renal impairment, although it is contraindicated in patients with severe renal impairment (eGFR <30 mL/min).”
46
A risk/benefit assessment may be necessary for patients with impaired renal function that may clinically benefit from remdesivir, despite the current eGFR thresholds. 48
As stated previously, remdesivir formulations contain SBECD to enhance solubility. According to Jorgensen et al, Formulations containing SBECD have historically been cautioned against in patients with renal impairment, although clinical data suggest SBECD accumulation does not increase the risk of acute kidney injury. There are no recommendations for dose adjustments in patients with mild to moderate renal impairment at this time.
48
Can Remdesivir Be Used in Patients With Hepatic Impairment?
There are no specific studies conducted with remdesivir in patients with hepatic impairment.46,47 According to the FDA’s Fact Sheet for Health Care Providers, it is not known if dosage adjustment is needed in patients with hepatic impairment, and remdesivir should only be used in patients with hepatic impairment if the potential benefit outweighs the potential risk. 25
Singh et al report that remdesivir is believed to be rapidly cleaved by hydrolases and thus the effect of hepatic impairment on remdesivir plasma levels is likely low. Given the benefit-risk ratio, no dose modification is currently recommended in patients with COVID-19, though it is contraindicated in patients with alanine aminotransferase (ALT) >5 times upper limit of normal or severe hepatic dysfunction. 46
What Are the Adverse Effects Associated With Remdesivir?
Remdesivir has several ongoing investigations into safety and efficacy, so at this time, not all of the safety risks are known. Also, when reviewing studies for potential problems, it has been asserted that it can be difficult to distinguish adverse effects from symptoms of COVID-19. 49 Based on current evidence, what follows are potential adverse effects of remdesivir.
Infusion-related reactions have been observed during or around the time of remdesivir infusion, and may include low blood pressure, nausea, vomiting, sweating, and shivering. 43 In general, adverse effects of intravenous administration may include brief pain, bleeding, bruising of the skin, soreness, swelling, and possible infection at the injection site. 50
Laboratory abnormalities reported include transient increase in liver enzymes, prothrombin time and blood sugar in small number of subjects in research studies. 33
The increases in levels of liver enzymes observed in patients who have received remdesivir may be a sign of inflammation or damage to cells in the liver. 25
Allergic reactions may include low blood pressure, changes in heartbeat, shortness of breath, wheezing, swelling of the lips, face, or throat, rash, nausea, vomiting, sweating, or shivering. 50
Lower grade gastrointestinal adverse effects like nausea and diarrhea have also been reported in a small number of cases. 49
Are There Drug to Drug Interactions With Remdesivir?
At the time of this writing, there are no published drug-drug interaction studies with remdesivir. 51
The FDA has issued a warning to health care providers that coadministration of remdesivir and chloroquine phosphate or hydroxychloroquine sulfate may result in reduced antiviral activity of remdesivir and is not recommended. 52 Furthermore, the FDA states that clinical significance has not been ascertained, and further evaluation is needed.
In vitro assessments have been conducted of remdesivir as a substrate for drug metabolizing enzymes and peptide transporters. 25 This indicates that the pharmacokinetics and pharmacodynamics of remdesivir may be affected alone or in concert with other drugs. As expressed by Muntané, “The interplay between drug metabolizing enzymes and transporters is one of the confounding factors that have been recently shown to contribute to potential complex drug interactions.” 53
In technical terms, in vitro, remdesivir is a substrate for drug metabolizing enzymes CYP2C8, CYP2D6, and CYP3A4, and is a substrate for Organic Anion Transporting Polypeptides 1B1 (OATP1B1) and P-glycoprotein (P-gp) transporters. In vitro, remdesivir is an inhibitor of CYP3A4, OATP1B1, OATP1B3, BSEP, MRP4, and NTCP. 47
Although suggestive of potential drug interactions, the clinical relevance of these in vitro assessments has not been clearly established. 25
Yang has published guidance regarding remdesivir metabolism and drug-drug interactions, yet states that the guidance can be confusing or even contradictory. 51
The Liverpool Drug Interaction Group was established in 1999 by members of the Department of Pharmacology at the University of Liverpool to provide a freely available drug-drug interaction resource for drugs used to treat HIV infection. 54 It has since advanced to include drug interaction information for the treatment of hepatitis B, hepatitis C, primary biliary cholangitis, and various cancers. The organization has recently expanded the Website to include drug interactions checking with experimental COVID-19 therapies.51,54
Is There a Pediatric Dosage for Remdesivir?
Pediatric dosage of remdesivir is specified by the patient’s weight in kilograms, and whether the patient is on invasive mechanical ventilation and/or ECMO. Dosage is expressed in milligrams per day with specified infusion parameters. Health care professionals may obtain information on individualized pediatric dosing in greater detail from the FDA’s Fact Sheet for Health Care Providers released on May 1, 2020, and revised August 2020. 25
Is Remdesivir Safe in Pregnancy?
No adequate and well-controlled studies of remdesivir use in pregnant women have been conducted. It is recommended that remdesivir be used during pregnancy only if the potential benefit justifies the potential risk for the mother and the fetus. 25
In nonclinical reproductive toxicity studies, remdesivir demonstrated no adverse effects on embryo-fetal development when administered to pregnant rats and rabbits at systemic exposures (AUC) of the predominant circulating metabolite of remdesivir (GS-441524) that were 4 times the exposure in humans at the recommended human dose (RHD). 25
A cohort study was conducted by Pierce-Williams et al of 64 pregnant women with severe or critical COVID-19 infection hospitalized at 12 US institutions. Remdesivir was used in 25% of the women. No adverse drug events were reported specific to remdesivir. There were no reports of maternal deaths, stillbirths, neonatal deaths, vertical transmission, and one report of maternal cardiac arrest, after a prolonged disease course. 55
What Monitoring Is Needed in Patients Using Remdesivir?
Similar to a drug product’s package insert for approved drugs, the FDA’s Fact Sheet for Health Care Providers provides technical information about remdesivir, specifically on patient monitoring recommendations. 25 Given the limited experience with remdesivir at the recommended dose and duration, the following are recommendations for patient monitoring:
Patients should have appropriate clinical and laboratory monitoring to aid in early detection of any potential adverse events while receiving remdesivir.
The decision to continue or discontinue remdesivir therapy after development of an adverse event should be made based on the clinical risk/benefit assessment for the individual patient.
Patients undergoing remdesivir therapy should be monitored for symptomatic improvement, serum chemistries, hematology, ALT, aspartate aminotransferase (AST), bilirubin, alkaline phosphatase, creatinine, and creatinine clearance.
Monitor renal and hepatic function prior to initiating and daily during therapy with remdesivir. 28
Monitor serum chemistries and hematology daily during therapy. 28
Conclusion
This review reveals a multitude of issues for health care professionals to consider for remdesivir in the treatment of COVID-19. Scientists and clinicians are in the initial stages of knowledge acquisition regarding remdesivir’s efficacy and effectiveness, safety, and dosing, particularly in special populations such as children and the elderly, pregnant women, and patients with renal and hepatic impairment. In several areas, available data are insufficient to support evidence-based treatment guidance for the use of remdesivir in patients infected with the novel coronavirus, SARS-CoV-2. Ongoing placebo-controlled clinical trials with diverse populations utilizing larger sample sizes continue to be the most advisable informative source of outcomes, adverse events, and potential clinical applications of remdesivir administered to COVID-19 patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.