
Abstract
Background
The use of oral anticoagulant therapy is rising steadily.1,2 Although warfarin is cheaper than new oral anticoagulants, it predisposes a high risk of bleeding, especially if the international normalized ratio (INR) values exceed 3.0.1,2 This circumstance causes dilemma among prescribers in determining the appropriate initiation dose for warfarin-naive patients due to the wide variation on dose response to warfarin.
Therefore, the need to determine warfarin dose initiation is crucial and requires careful monitoring. Different regimens of initiating warfarin have been developed in many studies aiming to achieve the therapeutic target of INR efficiently without causing any adverse events.1-3 Most of these conditions generally require INR values that range between 2.0 and 3.0 except for in the cases of heart valve replacements where a higher range of INR between 2.5 and 3.5 is usually recommended. 4 Certain conditions such as acute deep vein thrombosis requires quick stabilization of the INR to reduce harms and minimize the cost of anticoagulant therapy. In acute deep vein thrombosis, low-molecular-weight heparin (LMWH) or heparin is used together with warfarin. 4 In other conditions, such as those that involve the monitoring of atrial fibrillation and left ventricular clot, the time to establish the therapeutic target is not so crucial.5,6 Several warfarin initiation regimens involve a high loading dose (10 mg), followed by a maintenance dose based on INR values on a daily basis.1,7-10 Nevertheless, this regimen has not been applied for the Malaysian population. Most of the hospitals in Malaysia start their regimen with 5 mg daily on Day 1 and dose adjustment is done daily according to INR value.
Hence, a simple 3-day warfarin initiation regimen has therefore been developed to improve the management of warfarin with an emphasis on reducing the frequency of over-anticoagulation. In this regimen, the maintenance warfarin dose would be predicted from the INR value obtained on Day 4. Patients would be at higher risk of bleeding if the INR values reach ≥4.0 as this has been associated with a substantial risk of major bleeding events. 11 Although the association between the INR values of ≥4.0 and the increased risk of hemorrhage is well documented in the literature, this study used INR >3.2 as a cutoff point as bleeding risk to determine whether warfarin dose would need to be reduced or withheld.
Materials and Method
Study Design
A retrospective chart review study was conducted in Malaysia at Hospital Tengku Ampuan Afzan, a tertiary hospital in Kuantan, Pahang. Ethical approval for this study was obtained from the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (NMRR-18-3959-43976).
Patients
Patients in this study were sampled from those who received warfarin from July 1, 2017, until June 30, 2020, in Warfarin Medication Therapy Adherence Clinic (W-MTAC) and In-patients Anticoagulation Service (IPACS). The W-MTAC was established at Hospital Tengku Ampuan Afzan in 2010, and since then, this service has been extended to inpatients setting in IPACS on February 1, 2017. The sampling method used for this study was universal sampling. This study evaluated the ability of a 3-day regimen to achieve the INR value ≥50% from the baseline on Day 4 and the accuracy in predicting the weekly maintenance dose from INR value on Day 4. The risk of over-anticoagulation (INR > 3.2) and major bleeding were evaluated in both settings. All new patients above 18 years of age with a target INR of 2.0 to 3.0, using either Regimen 1 or Regimen 2 (see Table 1), with their INR measured on Day 4 and Day 11 were included. Pregnant patients and patients whose baseline INR was >1.3 were excluded from this study.
Initiation Dose for Warfarin Initiation According to the INR a .
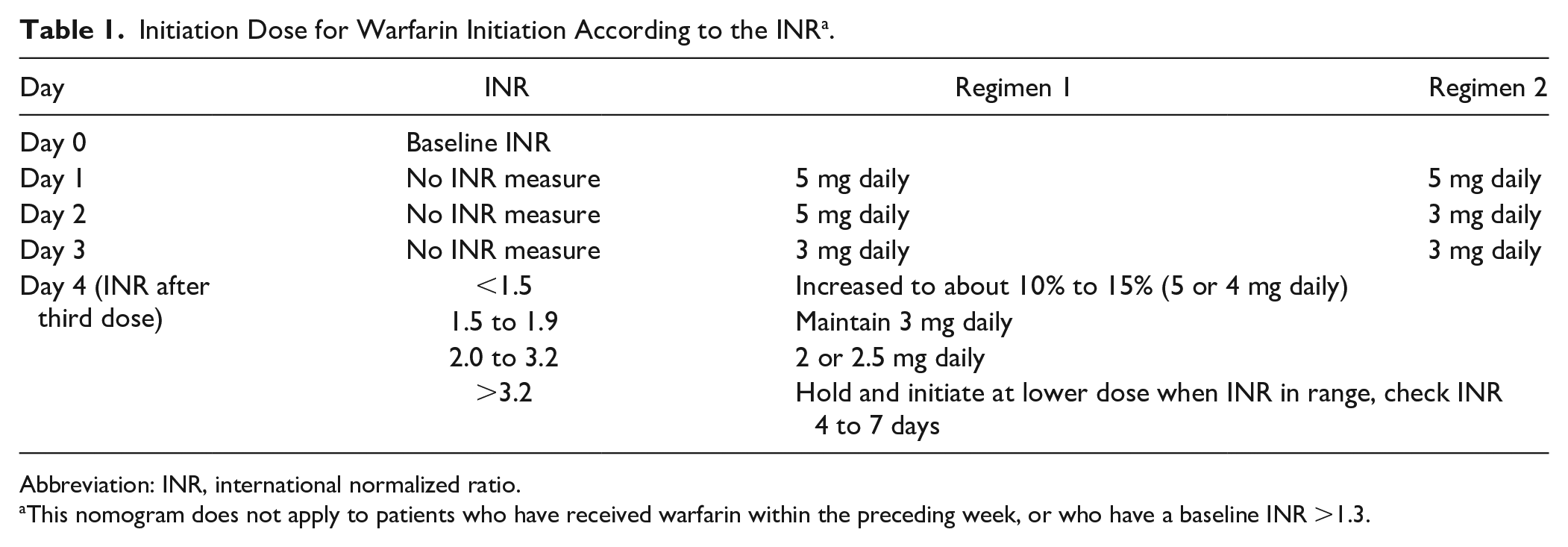
Abbreviation: INR, international normalized ratio.
This nomogram does not apply to patients who have received warfarin within the preceding week, or who have a baseline INR >1.3.
Warfarin Initiation Regimen
For the initiation of warfarin, the first day of warfarin treatment was designated as Day 1. Warfarin doses were given in the evening (6
Data Collection
The baseline clinical and laboratory characteristics, indication, warfarin doses and INR values, concomitant medications, and comorbid conditions of all patients recruited as participants in the present study were collected retrospectively. Over-anticoagulation was defined as having the INR value >3.2 as the dose adjustment would need to be done.
Statistical Analysis
Statistical analysis was performed using IBM Statistics SPSS version 21. Baseline characteristics were summarized using frequencies and percentage for categorical variables while means (M) standard deviations (SDs) were used for continuous variables. Correlations between the predicted and actual maintenance dose of warfarin were evaluated using the Pearson correlation coefficient (r2).
Outcome Measures
The primary outcome measure was the number of INR values that had reached ≥50% before the warfarin maintenance dose was given for 1 week and the percentage of patients who achieved the therapeutic INR at Day 11. Secondary outcomes included bleeding events that required medical attention, symptomatic thromboembolic events, and the correlation between the predicted and actual warfarin dose based on the Day 4 INR measured in Pearson correlation (r2). The maintenance dose was considered to have been achieved if no dose adjustment was made after patients had been given a weekly dose and INR reached the target on Day 11. The warfarin maintenance dose was expressed as a weekly dose of warfarin (in mg) and the INR achieved target range of 2.0 to 3.0. A value INR of more than ±0.2 from the target range was considered as a significant change in the INR value. The extended therapeutic range (target range ±0.2) was used as a therapeutic range in this study in accordance with the Warfarin Protocol published by the Ministry of Health, Malaysia. 12 No dose adjustment would be needed if the INR remained between 1.8 and 3.2. This extended range was adapted from the CHEST guideline, 13 which has recommended that no dose adjustment should be made for INR ≤0.5 above or below the therapeutic range.
Results
During the entire audit period, a total of 186 patients had been screened. However, only 165 patients were included because 21 patients who had been using different 3-day warfarin initiation regimen were excluded (see Figure 1). The mean (±SD) age was 57.2 ± 15.31 years (range = 18 to 83 years); there were 94 male patients. The demographic details of the study population are shown in Table 2. The indications for oral anticoagulation were atrial fibrillation in 86 patients and venous thromboembolism in 49 patients while 55 patients had bridge therapy either with LMWH or heparin. In addition, 13 out of 14 patients who had concomitant other drugs with warfarin showed drug interaction, which increased the INR. Most of the patients received antibiotics during their hospital stay at the ward. There was 1 patient who had received rifampicin which led to the reduction of the INR level.
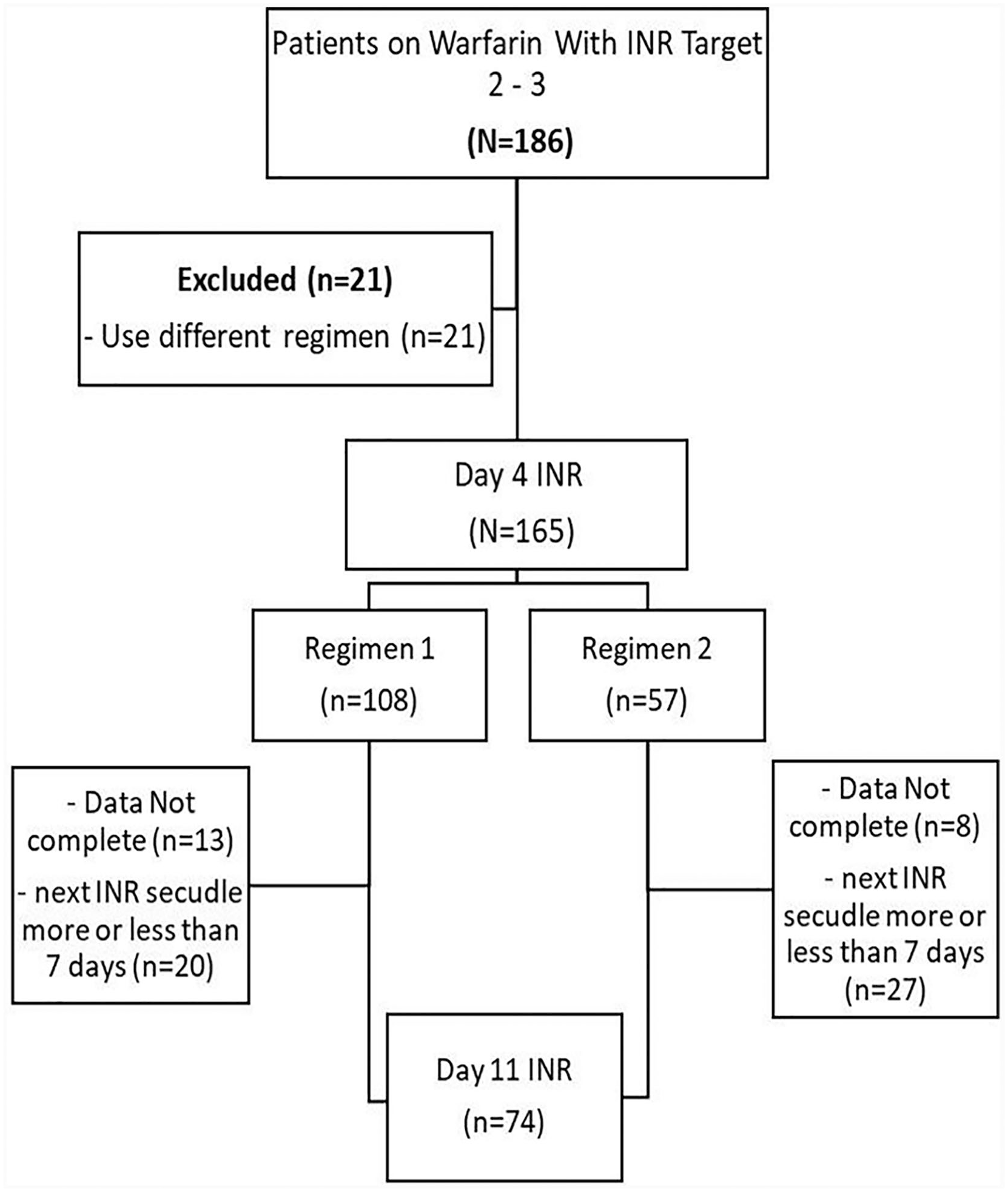
Selection process of eligible patients.
Demographic Details of Patients.
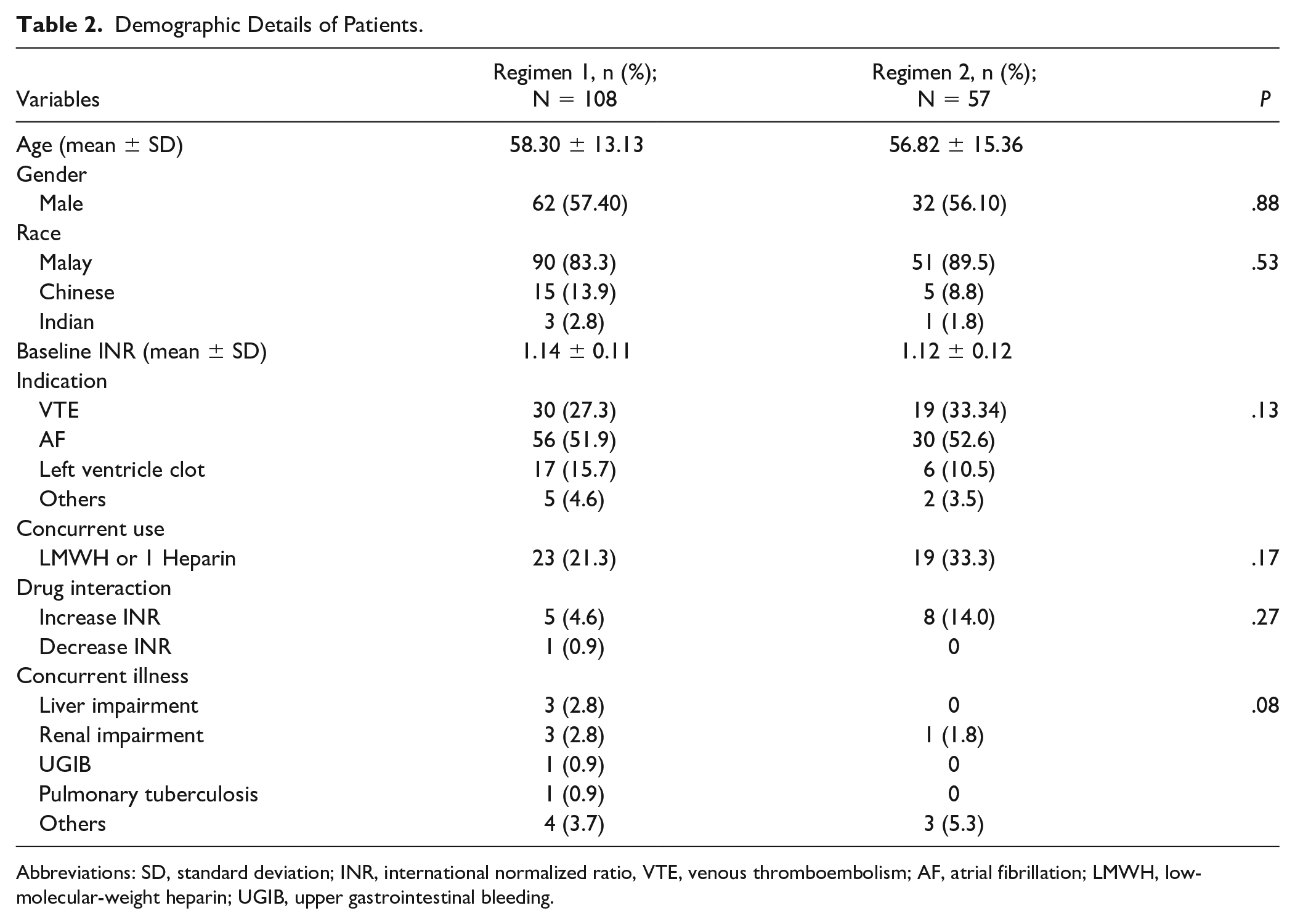
Abbreviations: SD, standard deviation; INR, international normalized ratio, VTE, venous thromboembolism; AF, atrial fibrillation; LMWH, low-molecular-weight heparin; UGIB, upper gastrointestinal bleeding.
INR on Day 4
The INR values after initiation of Regimen 1 and Regimen 2 are shown in Table 3. Overall, 53% of the patients achieved >50% of baseline INR with13 patients reaching INR >3.2 at Day 4. Out of the 13 patients, 2 patients had INR >10.0 after initiation dose of Regimen 1 and Regimen 2, respectively. This patient received Regimen 1 had renal impairment and use antibiotic, which can increase the INR, while another patient received Regimen 2 had other concurrent illness and had concomitant drug which can increase INR. These patients did not have any sign and symptom of bleeding which require medical attention.
The INR Value on Day 4 After Initiation of Regimen 1 and Regimen 2.
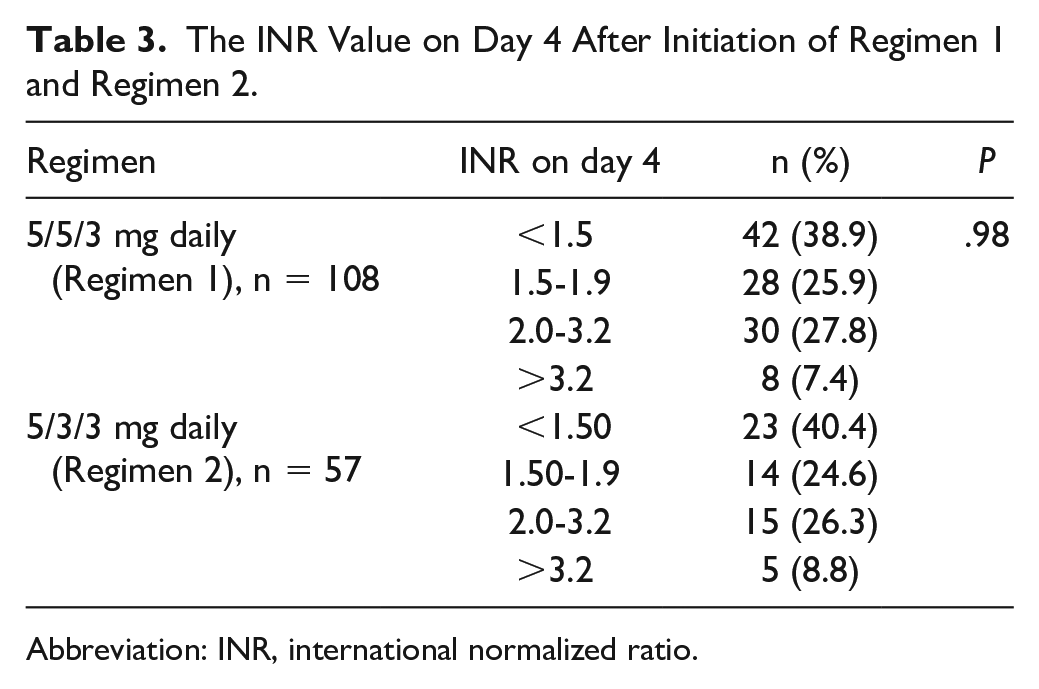
Abbreviation: INR, international normalized ratio.
INR on Day 11
Of 165 patients, 74 patients were included for prediction of 1-week warfarin dose. Approximately two thirds (70.3%) of the patients achieved the target INR while the dose for 15 patients (20.2%) and 7 patients (9.5%) needed to be increased and reduced, respectively. The mean values for the actual and the predicted weekly maintenance doses on Day 10 were 22.8 ± 0.5 mg (95% confidence interval [CI] = 21.7 to 23.9 mg) and 23.5 ± 0.5 mg (95% CI = 23.4 to 24.5 mg), respectively. The actual and predicted doses were found to be highly correlated (r2 = 0.75, P < .0001; see Figure 2). The predicted dose was equal to the actual dose in 26 patients (35.1%) while the dose for 30 patients had to be reduced and the dose for another 18 patients needed to be increased (see Figure 3).
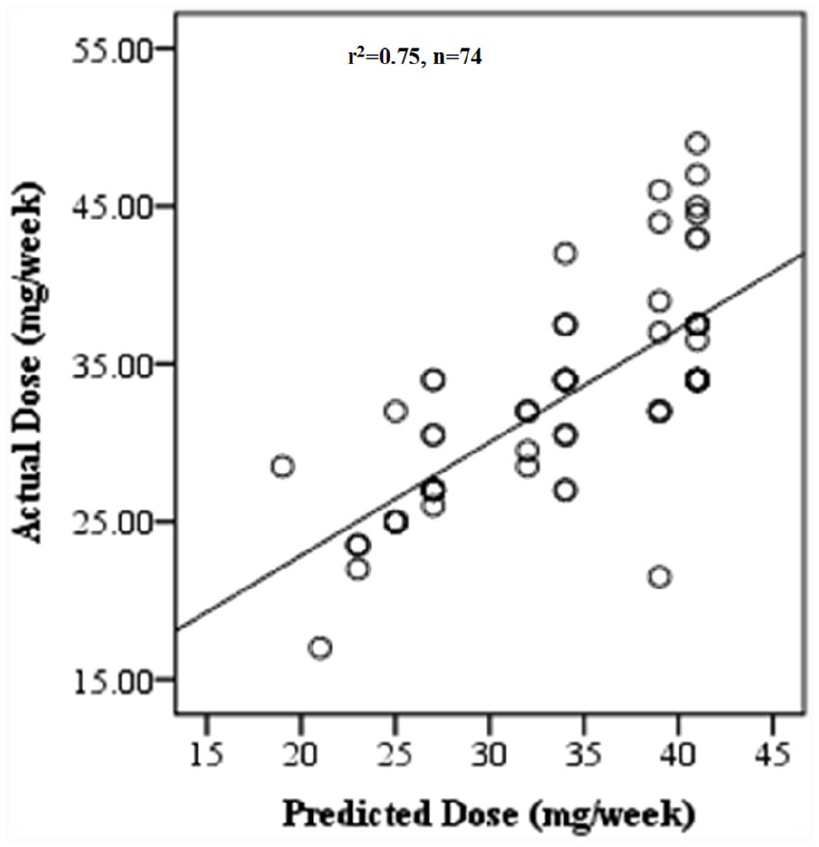
Correlation between the predicted and the actual weekly maintenance dose of warfarin.
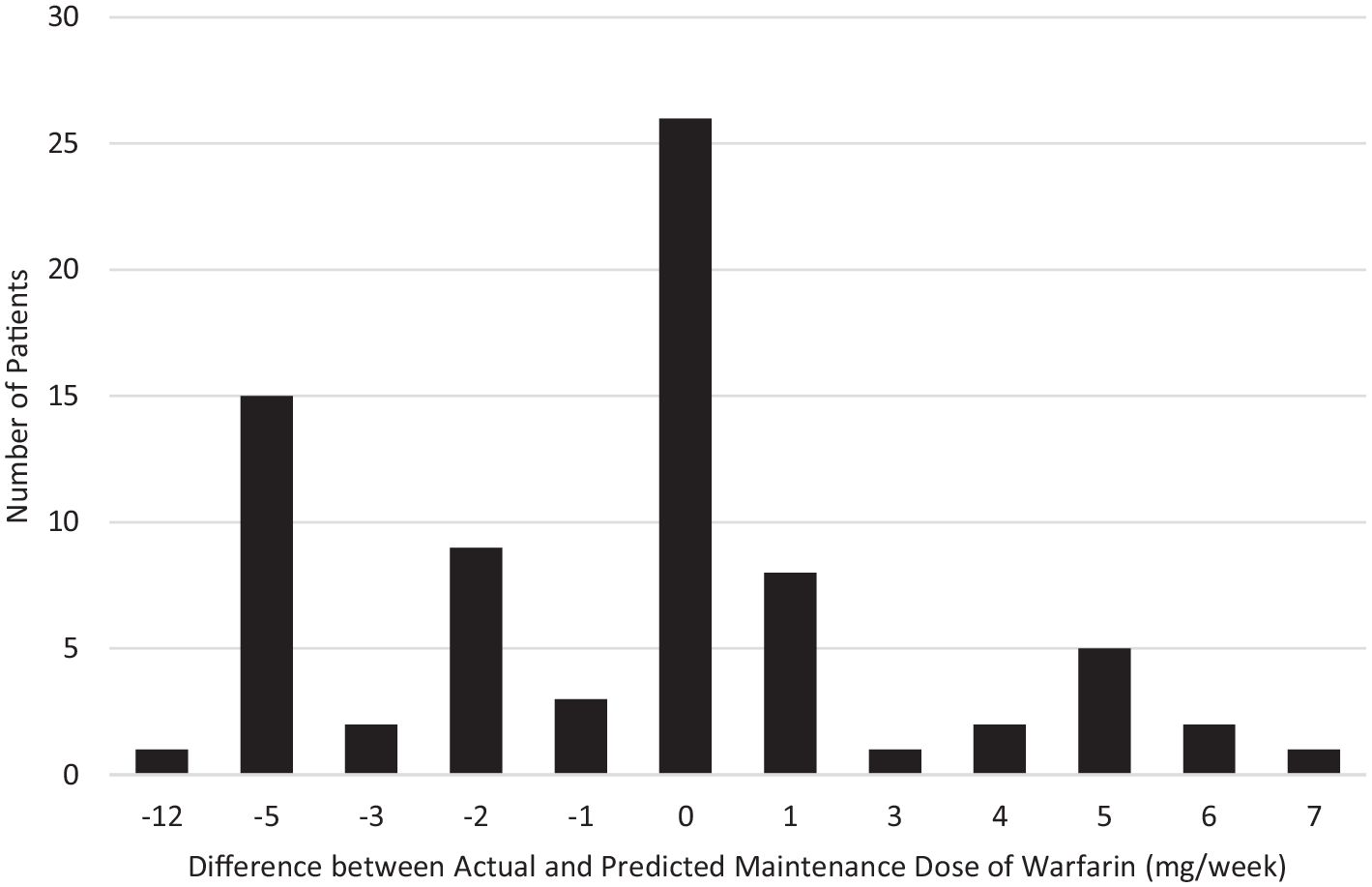
The difference between the actual and predicted maintenance dose.
Discussion
In Malaysia, there has been no guideline for the warfarin initiation that would safely and accurately predict the weekly maintenance dose of warfarin therapy. Hence, 88 facilities running MTAC Warfarin services in this country have been operating without any standard guideline and most of the prescribers initiate warfarin differently. As every prescriber knows, the lack of standardization in how warfarin is prescribed as an anticoagulant particularly at initiation part is a major problem. Many prescribers are attempting to find the solution is to prescribe new oral anticoagulant. However, because this could incur higher cost, many patients continue to use warfarin.
As a result of the increasing complexities of initiating and monitoring of warfarin therapy, many hospitals develop their own initiation or induction regimens. Achieving fast INR target is important not only for patients, but it is also essential for the health care providers to reduce the costs related to monitoring and any adverse events of warfarin. Thus, choosing the correct initiation regimen is critically important. Current evidence is still lacking in determining the safe initiation regimen especially in the Asian population. Furthermore, no study has been conducted to determine what is the suitable initiating dose for the Malaysian population. Therefore, this study was carried out to determine the suitable initiation regimen for initiating warfarin therapy and weekly dose based on the INR after the initiation regimen. Selection of first 3-day dose of initiation regimen is quite challenging. Kovac and colleagues 9 have shown that initiating a higher dose such as 10 mg would often cause supratherapeutic INR during treatment induction, 10 and recent guidelines have also not recommended the initiation of loading dose. 13 Past research has proven that Asian patients would need a lower dose compared with other ethnicities. 14 In our setting, the 10 mg dose had also been in practice before the introduction of IPACS, which also led to over-warfarinization. Patients would need to stay longer as close monitoring had to be done.
The supratherapeutic INR was also observed in our study as 13 patients had INR above 3.2, which required withholding and reducing of warfarin dose on Day 4. Several studies either used 4 mg daily for 3 days 15 or used the initiation dose of either 10 mg or 5 mg of warfarin.7,16,17 Throughout 6 months of observation in IPACS, 18 the initiation dose consisting of Regimen 1 or Regimen 2 was developed. Furthermore, the American College of Chest Physicians supports the induction dose which ranges from 2 to 5 mg per day and is adjusted according to the patient’s INR. 13 In clinical practice, higher loading doses of warfarin may increase the patient’s risk of bleeding due to excessive depletion of factor VII and protein C. This may place a patient in a hypercoagulable state, which may prolong hospital stay due to rapid rise in the INR value.
Approximately 53% of the patients in our study had INR that ranged between 1.5 and 3.2. None of the patients developed any adverse event on Day 4. Although LMWH or heparin had been administered in 55 patients, this did not influence the INR results. However, patients were considered to be at a higher risk of bleeding tendency. Overlapping with heparin or LMWH was recommended when patients have acute venous thromboembolism, which needs a rapid anticoagulant effect and the bridging would be continued for at least 5 days and until the patient’s INR is at least 2.0 for 2 consecutive days.4,19 In the present study, the warfarin dose for 13 patients receiving antibiotics needed to be reduced on Day 4 as their INR levels were above 3.2. There were no significant bleedings that required any intervention to reduce the INR. Warfarin therapy was withheld for 2 to 3 days until INR value came down to less than 2.0.
The mean values for the actual maintenance weekly dose on Day 10 was 22.8 ± 0.5 mg (95% CI = 21.7 to 23.9 mg) and was 23.5 ± 0.5 mg (95% CI = 23.4 to 24.5 mg) for the predicted dose, both of which were highly correlated (r2 = 0.75, P < .0001). Based on the actual weekly dose, the safe dose to archive INR target is 3 mg daily. A study conducted by Siguret and colleagues 17 had the mean value of the actual daily maintenance dose of 3.2 ± 1.7 mg, which is almost similar to the mean daily dose (3.2 ± 0.6 mg) in our study. Asian patients require low-dose warfarin because they are known to be more sensitive to warfarin. 20 Dang and colleagues 14 have recommended that patients who are of Asian ethnicity should start on lower doses (~50%) in comparison with White or African American patients. In their study, Lee and colleagues 21 used the mean warfarin dose of 3.30 ± 2.23 mg/day among Hong Kong Chinese patients. This was also similar with our population even though the patients in our study were mainly of Malay ethnicity. Despite its efficacy, managing warfarin therapy is challenging due to its narrow therapeutic range and variability of drug response among individuals. The warfarin dosing must be individualized based on each patient’s dietary intake, body weight, age, concomitant disease, drug-drug interaction, ethnicity, and genetics polymorphisms. Thus, choosing initiation regimen and determination of warfarin dose after the initiation is complicated and should be done carefully.
Strengths and Limitations
This study represents the first analysis of initiation regimens related to warfarin therapy in Malaysia. It is anticipated that these findings will help health care providers in selecting the proper dose to avoid any risk due to under or over-warfarinization. Our study has its limitations mainly due to its retrospective study design. In addition, the patients in the present study were predominantly male who were patients at a single center and these 2 factors might affect the generalizability of the results. Nevertheless, the main strength of our study is drawn from its local population-based study design that involved patients who were receiving warfarin therapy. This has shed some light on the issue and gives a better understanding of the local practice specifically in Malaysia and can be used generally as a standard guideline in managing warfarin therapy in Asia.
Conclusion
Our review findings suggest that both initiation regimens and prediction of weekly maintenance dose of warfarin in the present study was simple, safe, accurate, and suitable to be used in both ambulatory and inpatient settings for managing warfarin therapy in Malaysian population.
Footnotes
Acknowledgements
We would like to thank the Director General of Health of Malaysia for granting us the permission to publish this study, Pharmaceutical Service Division MOH, Tengku Ampuan Afzan Hospital. We thank W-MTAC and IPAC teams for their contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.