
Abstract
Keywords
Introduction
Reducing hospital readmission rates is one of the main priorities of health care systems, partly because of the high economic impact. 1 The ratio of unscheduled readmissions of <30 days after discharge is a quality indicator of the efficiency of hospital care, whereas readmissions beyond this duration are associated more with disease- and patient-related factors. 2 For this reason, there is currently increasing interest in studying the factors that may cause these readmissions and may require intervention.3,4 The overall readmission rate in Spain in 2017 (latest available data) was 8.01%. 5 As for the rate of potentially avoidable readmissions (PAR), there are no official data in Spain, but according to the literature, it is estimated to be around 20%. 6
Regarding the influence of pharmacotherapy, several studies justified that drug-related problems (DRPs) cause both admissions and readmissions. The results of these studies are quite heterogeneous, reporting incidences of drug-related admissions ranging from 0.2% to 43.3%.7-9 Furthermore, in a meta-analysis, it was observed that the elderly are 4 times more at risk of admission for adverse drug reactions (ADRs), and 88% of these ADRs would have been preventable. 10 In another study, Thomas et al 11 noted that 61% of readmissions were associated with DRPs. In a 2018 systematic review that included 19 studies on the prevalence of readmissions associated with DRPs, a median of 21% (interquartile range = 14% to 23%) of readmissions related to drug therapy was observed, with cancer and a high Charlson Comorbidity Index being risk factors. The medications most frequently involved were antibiotics, diuretics, vitamin K antagonists, and opioids. 12 In Spain, between 10% and 46% of the elderly hospitalized or attending an emergency department are a result of an ADR. It is estimated that ADRs are responsible for up to 30% of hospital admissions in elderly patients, with the main cause of ADRs being inappropriate prescription of medications and suboptimal monitoring of prescribed treatments.13-16
Although there is scientific evidence supporting the design of interventions led by a clinical pharmacist in reducing readmissions, 17 the potential of combining these programs with patient stratification systems according to their risk of PAR remains to be determined. The present study aimed to determine whether a pharmaceutical care (PC) program at discharge in polymedicated patients at high risk of PAR according to the HOSPITAL score 3 improves the 30-day readmission rate (30-dRR).
Methodology
Study Design and Participants
This was a prospective, quasi-experimental, controlled intervention study, conducted in Spain over 11 months (March 2019 to February 2020) in a tertiary hospital with more than 1200 beds. Before patient recruitment, we worked together with the Hospital IT Service, which integrated the HOSPITAL score into the electronic health record (EHR) alert system. This integration allowed daily automatic stratification of all admitted patients according to the risk of PAR.
Patients included in the intervention group underwent a PC program and pharmacotherapeutic follow-up at discharge, whereas the control group underwent standard PC in hospital (medication reconciliation on admission and daily pharmaceutical monitoring and validation of treatment). The control group was a retrospective cohort of chronic patients at high risk of PAR, with admission episodes to the hospital during 2018. Both groups matched the following inclusion criteria: age >18 years, complex chronic patients at high intervention level (classified by the primary care health system), polymedicated (>5 medications), and at high risk of PAR (HOSPITAL score ≥7). Patients with active oncological disease, admitted for surgical procedures or institutionalized were excluded. The follow-up period was 30 days after discharge.
The PC and pharmacotherapeutic follow-up program consisted of 2 phases and was carried out in collaboration with primary care pharmacists:
During the hospital stay: ○ Pharmacotherapeutic anamnesis. ○ Assessment of treatment complexity by calculating the 65-item Medication Regimen Complexity Index adapted to Spanish (MRCI-E).
18
○ Medication reconciliation on admission, review of treatment, and preparation of recommendations for the doctor in charge to optimize the patient’s pharmacotherapy. ○ Daily pharmaceutical monitoring and validation of treatment. ○ Medication reconciliation and delivery of treatment plan on discharge, contact telephone and email for consultation resolution. ○ Oral and written training on high-alert medications for patients with chronic illnesses (HAMCs) according to the Institute for Safe Medication Practices in Spain.
19
○ Resolution of discrepancies between discharge report and electronic prescription.
After discharge from hospital: ○ Telephone follow-up on days +7 and +21 postdischarge. ○ Preparation of a report for the Primary Care Pharmacy Service (SFAP, by its Spanish acronym) that includes the following: list of medication, changes and pharmacotherapeutic recommendations made, DRP detected during admission, and discrepancies not resolved at discharge. ○ SFAP review of the adequacy of the treatment, focusing on whether the changes introduced could lead to any safety issues. ○ Preparation of a report for the family physician on the recommendations of the Hospital Pharmacy Service, together with those derived from the SFAP review.
This study was approved by the Hospital’s Ethics and Research Committee (19/005).
Data Collection
The patients’ demographic, analytical, pharmacotherapeutic, and medical data were obtained from the clinical history and electronic prescription. In the case of the patients included in the intervention group, pharmacotherapeutic data were also obtained from the clinical interview after the patient signed an informed consent form to participate in the study. For the control group, a list of complex chronic patients at high risk of PAR according to the HOSPITAL score with hospitalization episodes during 2018 was extracted from the EHR, and the predefined inclusion criteria were assessed in each patient. Discharge reports and the electronic prescription were reviewed to obtain the pharmacotherapeutic information (pharmaceutical form, dosage, posology, and additional instructions) necessary to calculate the MRCI-E at admission and discharge.
Measures
The risk of PAR was assessed according to the HOSPITAL score, which consists of parameterizable items that can be obtained from the EHR: sodium levels, hemoglobin, number of admissions in the previous 12 months, length of hospital stay, oncological versus nononcological patient, type of scheduled versus emergency admission, and procedures performed during admission (catheterization, colonoscopy, endoscopy, computed axial tomography, etc). 3 Because the HOSPITAL score was integrated into the EHR, patients at high risk of PAR (HOSPITAL score ≥7) were automatically identified daily. To evaluate the main objective, the rate of unscheduled readmission 30 days after discharge was calculated in each group (Number of patients with readmission at 30 days/Total number of patients). For the analysis of the secondary objectives and evaluation of the impact of the intervention on pharmacotherapy, the complexity of the treatment was calculated using the MRCI-E, which considers the number of medications (over-the-counter medications were also included), pharmaceutical form, frequency of administration, dosage, and additional instructions. 19 Combined medications were counted as a single medication for the total calculation and the calculation of the MRCI-E. We also collected the number of HAMCs according to the Institute for Safe Medication Practices in Spain. 19 In the case of HAMCs, the number of active ingredients was considered. The total number of medications, the number of HAMCs, and the MRCI-E were calculated for each patient on admission and 30 days after hospital discharge, and the following indicators were designed:
Δ MRCI-E: MRCI-E 30 days after discharge − MRCI-E on admission.
Δ Medications: Number of medications 30 days after discharge − Number of medications on admission.
Δ HAMC: HAMC number 30 days after discharge − HAMC number on admission.
Covariates
We recorded age, sex, number of pharmaceutical interventions (PIs) per patient, and degree of acceptance of the interventions by the physicians (PIs accepted/Total PIs). The PIs were obtained from the Access database of the Pharmacy Service, where all the PIs performed during the pharmaceutical validation of the treatment of admitted patients and their acceptance since 2017 are recorded.
Sample Size
Accepting an α risk of 0.05 and a β risk of 0.2 in a 2-sided χ2 test, 268 individuals were necessary per group to detect an absolute reduction of 10% in 30-dRR in the intervention group compared with the control group. The anticipated drop-out rate is 15%.
Statistical Analyses
The baseline demographic and pharmacotherapeutic characteristics (number of medications, HAMC, and MRCI-E on admission) of each group were compared descriptively. The results of continuous variables were expressed as means (SD) and categorical variables as proportions. For the comparison between the control and intervention groups, the χ2 test was used for categorical variables; for continuous variables, t tests were used for independent samples if they were normally distributed and Mann-Whitney U tests if they were nonnormally distributed. To evaluate factors associated with readmissions 30 days after discharge, odds ratios (ORs) with 95% CIs were estimated using multivariate logistic regression. The level of statistical significance was established as a P value <0.05, and data were analyzed using STATA, version 15 (StataCorp LLC).
Results
A total of 163 patients were enrolled in the intervention group during the study period, of which 27 (16.6%) were losses (11 were discharged out of pharmacists’ working hours; 9 died during hospital admission or the follow-up period; and 7 were referred to social health centers or another hospital at discharge). The mean (SD) age was 80 (12) years, and for pharmacotherapeutic variables, a mean (SD) of 15 (4) medications per patient, 5 (2) HAMCs, and a MRCI-E score of 37 (16) were observed. The baseline demographic and pharmacotherapeutic characteristics of both groups are shown in Table 1.
Demographic and Baseline Characteristics of the Patients. a
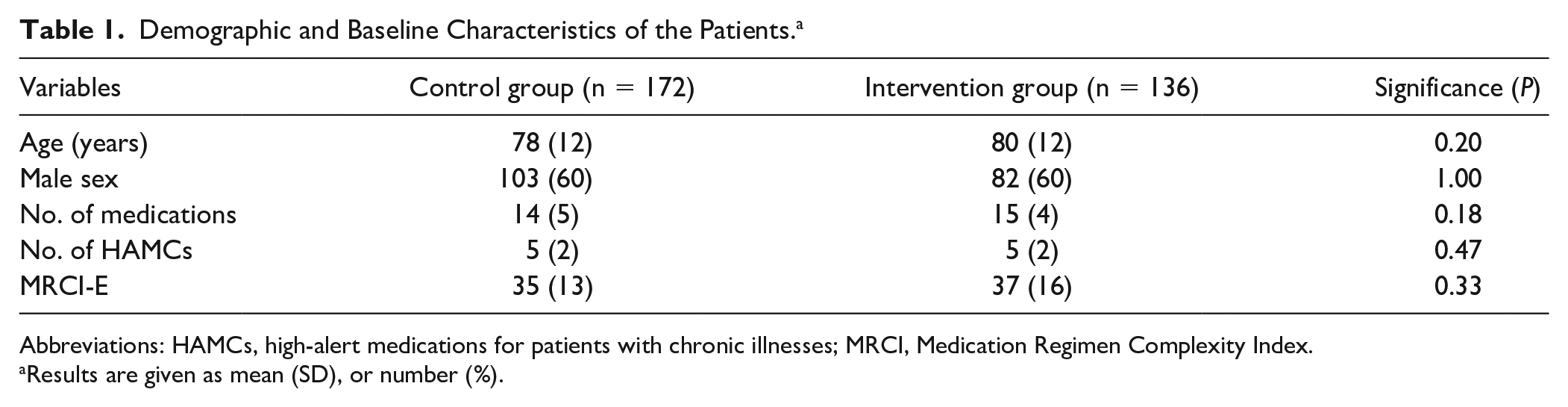
Abbreviations: HAMCs, high-alert medications for patients with chronic illnesses; MRCI, Medication Regimen Complexity Index.
Results are given as mean (SD), or number (%).
Outcome Indicators 30 Days After Discharge From Hospital
The 30-dRR was 18.4% in the intervention group, whereas in the control group, it was 25.6%. Concerning the pharmacotherapeutic variables, it was observed that in the intervention group, the MRCI-E index score was reduced by a mean of −4.18 points accompanied by a reduction in the total number of medications (−0.90) and the number of HAMCs (−0.63). There was an increase in the MRCI-E index score in the control group by an average of +2.24 points, accompanied by an increase in the total number of medications (+0.38). The results are shown in Table 2.
Outcome Indicators 30 Days After Discharge. a
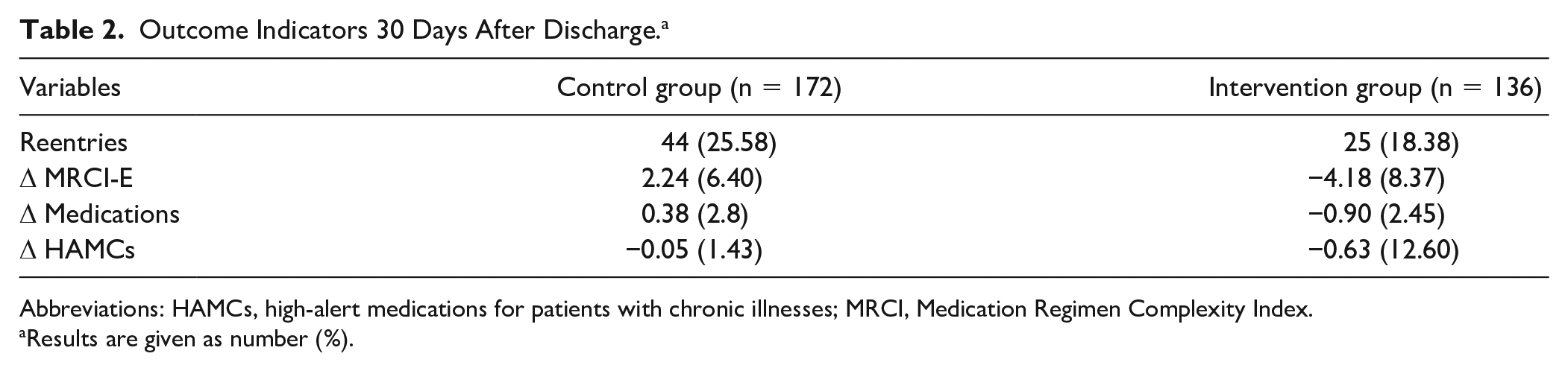
Abbreviations: HAMCs, high-alert medications for patients with chronic illnesses; MRCI, Medication Regimen Complexity Index.
Results are given as number (%).
Comparative analysis between both groups showed that the PC program significantly reduced the MRCI-E index score after hospital discharge (−6.42; 95% CI = −8.07 to −4.76) as well as the total number of medications (−1.28; 95% CI = −1.88 to −0.68) and the number of HAMCs (−0.58; 95% CI = −0.90 to −0.26). Compared with 30-dRR, the PC program did not show a significant reduction in the risk of readmission (OR = 0.66; 95% CI = 0.38 to 1.14). The results are shown in Table 3.
Statistical Analysis of Outcome Indicators 30 Days After Discharge Between Intervention and Control Groups. a
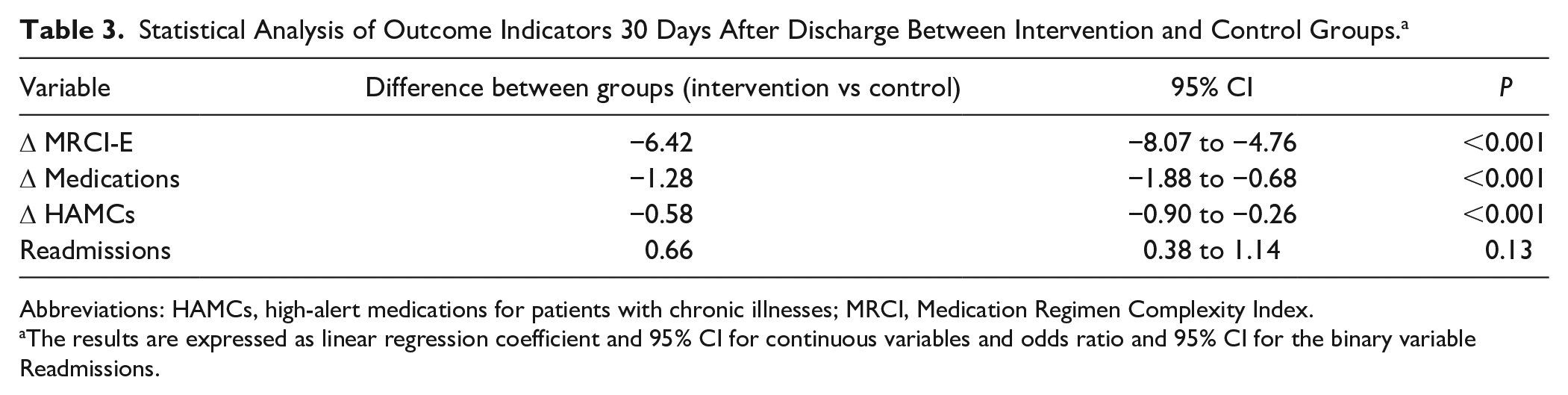
Abbreviations: HAMCs, high-alert medications for patients with chronic illnesses; MRCI, Medication Regimen Complexity Index.
The results are expressed as linear regression coefficient and 95% CI for continuous variables and odds ratio and 95% CI for the binary variable Readmissions.
Regarding the number of PIs performed per patient, in the control group, the mean (SD) was 1.72 (1.84), with a degree of acceptance of 37.84%, whereas in the intervention group, it was 3.16 (2.89), with a degree of acceptance of 69.30%. The results are shown in Table 4.
Statistical Analysis of the Pharmaceutical Interventions. a
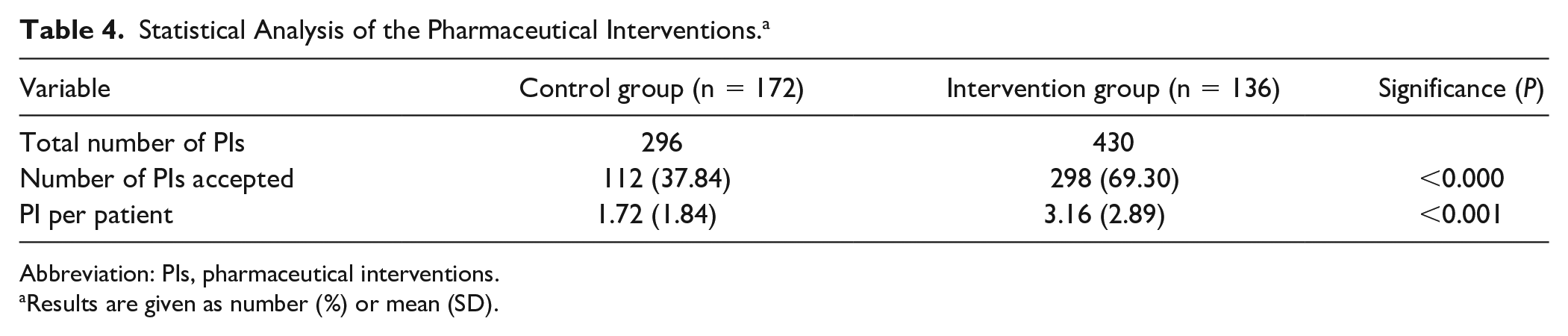
Abbreviation: PIs, pharmaceutical interventions.
Results are given as number (%) or mean (SD).
Factors Related to Readmissions 30 Days After Discharge
The number of medications on discharge (OR = 1.07; 95% CI = 1.01-1.14) was the only factor associated with readmissions 30 days after discharge in the multivariate logistic regression analysis. The results are shown in Table 5.
Factors Related to Readmissions 30 Days After Hospital Discharge.
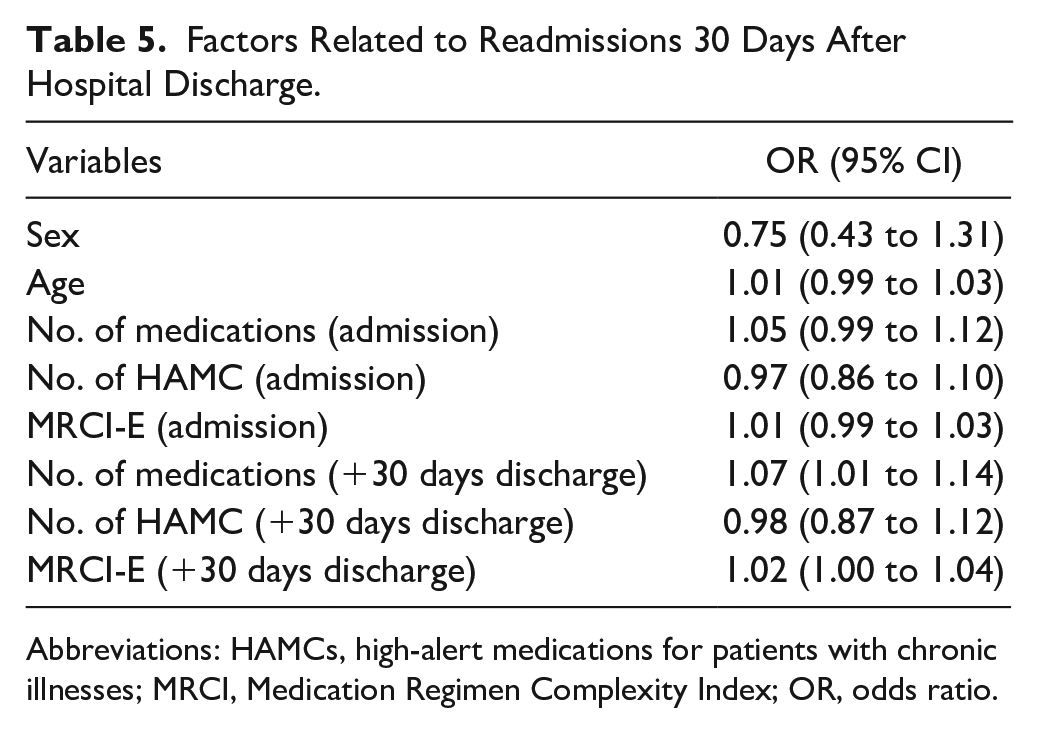
Abbreviations: HAMCs, high-alert medications for patients with chronic illnesses; MRCI, Medication Regimen Complexity Index; OR, odds ratio.
Discussion
The study results show a relevant impact of the PC program on reducing polypharmacy and treatment complexity (MRCI-E) after hospital discharge. This may be partly because the PC program not only focused exclusively on medication reconciliation, but also conducted a thorough review of treatment adequacy focusing on deprescribing opportunities. Moreover, pharmacotherapeutic continuity after discharge, coordinated with primary care pharmacists, was also one of the key points of the PC program and contributed to increasing the impact and degree of acceptance of the PI. In the scientific literature, an experience of coordination between pharmacists at different levels of care shows that because of their position in the health system, pharmacists can act as liaison figures with other professionals, facilitating the exchange of information, the resolution of discrepancies detected, or clarifying doubts that the patient may have. 20
Regarding PAR, a trend was observed in the reduction of 30-dRR, although statistical significance was not reached. In a 2017 systematic review and meta-analysis that analyzed the impact of PI carried out in care transitions on 30-dRR, an OR of 0.67 (95% CI = 0.58-0.74) was observed. 21 To interpret this result, we must also consider that in our study the patients had a high baseline risk of PAR (HOSPITAL score ≥7), which implies an estimated risk of readmission of 22.8%. 3 However, in the intervention group, the 30-dRR was lower (18.4%) than that expected according to the HOSPITAL score.
Conversely, in our study, we observed that a greater number of medications prescribed on discharge was associated with a higher risk of readmission at 30 days. Concerning the MRCI-E as a risk factor for readmission, different studies have demonstrated this relationship.22-24 However, it is true that they do not identify MRCI-E as a better predictor of readmission risk than the number of medications. In our case, there was no evidence that the MRCI-E was associated with a higher risk of readmission at 30 days.
As is evident from the literature,17,20,25 the study results highlight the relationship between polypharmacy and the risk of 30-day readmission. Therefore, PIs that achieve a reduction in polypharmacy and contribute to improving treatment efficacy and safety will potentially affect patient health outcomes.
Limitations
One limitation of the study is that the control group is a retrospective cohort of patients rather than a parallel cohort. Despite this, no relevant factors could modify the results because both groups were homogeneous in terms of baseline and demographic characteristics and there were no differences in routine clinical practice. Another limitation is that the estimated sample size could not be reached because we had to finish the study earlier as a result of the COVID-19 pandemic. Additionally, the pharmacy team’s working hours were not continuous over nighttime or weekends, and it led to patient losses as a result of hospital discharges out of the pharmacist’s working time.
Conclusion and Relevance
The integration of the HOSPITAL score in the EHR makes it possible to automatically stratify the risk of PAR of hospitalized patients and, therefore, to select those at greatest risk at the time of hospital discharge. It should be noted that coordination between pharmacists at both levels of care (Hospital and Primary Care) helps overcome some of the barriers that hinder the continuity of pharmacotherapeutic care at discharge.
In this study, it has been observed that PI reduces polypharmacy and complexity of patient treatment. Also, there is an association between a greater number of medications on discharge and a higher risk of readmission after 30 days. Although this study has not shown statistically significant evidence that the intervention reduces the 30-dRR, it has been observed that this rate is lower in the intervention group and is below the expected rate according to the HOSPITAL score. Future studies should examine the relationship between PIs and patient health outcomes as well as the impact on quality of life and satisfaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Foundation for Biomedical Research of the Hospital 12 de Octubre. No further funding was provided.