
Abstract
Background:
Dexamethasone use in patients hospitalized with COVID-19 significantly reduces mortality; however, it commonly results in hyperglycemia. Optimal treatment of dexamethasone-induced hyperglycemia is not well established.
Objective:
The study purpose was to assess the difference in blood glucose (BG) control between insulin glargine, neutral protamine hagedorn (NPH) insulin, and insulin glargine plus NPH insulin for dexamethasone-induced hyperglycemia in patients with type 2 diabetes (T2DM) and COVID-19 infection.
Methods:
This retrospective study was conducted in adult inpatients with T2DM and COVID-19 infection who received 6 mg of dexamethasone once daily and insulin during the 5-day study period. The primary outcome was the difference in mean point-of-care (POC) BG levels between study insulins. Secondary outcomes included the incidence of hyperglycemia and hypoglycemia, length of stay, and the percent difference between the mean daily inpatient and home basal insulin doses (for patients who were receiving basal insulin prior to admission in the insulin glargine and insulin glargine and NPH insulin groups only).
Results:
Ninety-six patients were included in the analysis (67 insulin glargine, 10 NPH insulin, and 19 insulin glargine plus NPH insulin). The difference in mean POC BG level was not different among groups (254 ± 60 mg/dL vs 234 ± 39 mg/dL vs 250 ± 51 mg/dL, respectively; P = 0.548). There were no significant differences in the secondary outcomes.
Conclusions:
No difference in the mean POC BG level was observed. Dexamethasone-induced hyperglycemia was poorly controlled in patients with T2DM and COVID-19 infection.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes coronavirus disease 2019 (COVID-19). COVID-19 is a highly contagious virus that has resulted in hospitalizations and over 6.5 million deaths across the world as of October 2022. 1 COVID-19 is known to cause a pneumonia-like disease with opacities seen on radiographic images, microvascular thrombosis, a state of inflammation, and, in advanced cases, inflammatory organ damage. 2 Due to these inflammatory processes, glucocorticoids have become the mainstay of therapy in preventing the progression of the disease. The Randomized Evaluation of COVID-19 Therapy (RECOVERY) trial found dexamethasone, at a dose of 6 mg intravenously or orally daily for up to 10 days, significantly reduced the 28-day mortality rate compared to the usual care group. 2 In addition, previous studies have shown that patients with uncontrolled diabetes who are hospitalized with COVID-19 have an increased risk of in-hospital mortality.3,4
Glucocorticoid use is associated with an increased incidence of hyperglycemia in patients with or without infection.2-4 While demonstrating a mortality benefit in the RECOVERY trial, hyperglycemia was the most frequent serious adverse reaction reported with the use of dexamethasone. 2 Higher doses and prolonged duration of glucocorticoid therapy have been shown to increase the incidence of hyperglycemia. 5 Glucocorticoid-induced hyperglycemia is multifactorial, resulting from inhibition of glucose uptake in muscle, increased hepatic gluconeogenesis, and increased insulin resistance in skeletal muscle. 6
The American Diabetes Association (ADA) recommends treatment of glucocorticoid-induced hyperglycemia based on the type of glucocorticoid used. In patients receiving intermediate-acting glucocorticoids, neutral protamine hagedorn (NPH) insulin is recommended. 7 NPH insulin has a similar onset and duration of intermediate-acting steroids, such as prednisone. 3 Alternatively, long-acting insulins, such as insulin glargine, are the standard of care for patients receiving long-acting glucocorticoids. 7
A few studies evaluated the treatment of glucocorticoid-induced hyperglycemia in non-COVID-19 patients. Previous studies demonstrated conflicting results on the effects of NPH insulin on glucose control in glucocorticoid-induced hyperglycemia. One study found the addition of NPH to a patient’s home insulin regimen was superior to basal insulin once daily for the treatment of glucocorticoid-induced hyperglycemia. 8 Other studies demonstrated no significant difference in the mean blood glucose (BG) level between groups receiving NPH insulin and insulin glargine in patients receiving intermediate-acting glucocorticoids.9,10 Previous studies have investigated the treatment of glucocorticoid-induced hyperglycemia with NPH insulin, but research is needed to determine the optimal regimen for treating dexamethasone-induced hyperglycemia. This study aimed to compare BG control between insulin glargine, NPH insulin, and insulin glargine plus NPH insulin in patients with type 2 diabetes mellitus (T2DM) receiving dexamethasone once daily for COVID-19 infection.
Methods
This institutional review board–approved, retrospective, multicenter, observational cohort study was performed from March 2020 to August 2021 at an 11-hospital health system, which includes a 794-bed academic medical center. Medical records of patients positive for COVID-19, who received 6 mg of dexamethasone during inpatient stay and NPH insulin or insulin glargine, were screened for inclusion. Patients aged 18 years or older were included if they received 6 mg of dexamethasone once daily for at least 5 days, had T2DM, and had received NPH insulin and/or insulin glargine. Using a health-system-based protocol, patients positive for COVID-19 who required oxygen therapy either through nasal canula or continuous positive airway pressure and had an oxygen saturation <94% within 10 days of symptom onset were eligible to receive dexamethasone. Exclusion criteria included patients with type 1 diabetes mellitus, receipt of a steroid other than dexamethasone, admission to the intensive care unit (ICU), administration of an insulin drip, continuous enteral nutrition or tube feed, continuous nothing-per-oral diet orders for >24 hours throughout the study duration, administration of total parenteral nutrition, and pregnancy.
Patients were divided into 3 cohorts: insulin glargine, NPH insulin, and the combination of insulin glargine and NPH insulin. Providers use their discretion in the selection of a type of insulin and dose; the health system does not have any guidelines in place. The primary outcome was the difference in mean point-of-care (POC) BG levels during hospitalization, which was defined by the average of fasting, prelunch, predinner, and bedtime BG readings. Secondary outcomes included the incidence of hyperglycemia (BG >180 mg/dL), incidence of hypoglycemia, hospital length of stay (LOS), and the percent difference between the mean daily inpatient and home basal insulin doses (for patients who were receiving basal insulin prior to admission (PTA) in the insulin glargine and insulin glargine and NPH insulin groups only).
Data collected at baseline from each patient’s electronic medical record (EMR) included basic demographics, hemoglobin A1c (HgbA1c), home insulin requirement, non-insulin antihyperglycemic medications, admission BG, components of the Charlson Comorbidity Index (CCI), and hospital LOS. Data points collected from the index day to day 5 of hospitalization included POC BG levels, number and level of hypoglycemic episodes, number of hyperglycemic episodes per patient, receipt of inpatient insulin (basal, bolus, sliding scale), and inpatient non-insulin antihyperglycemic medications.
The percent difference in mean daily inpatient and home basal insulin doses was defined as the difference between the mean daily inpatient and home basal insulin doses divided by the mean daily home basal insulin dose. The CCI is a previously validated tool used to classify a patient’s comorbid disease states that may confound outcome results. 11 The index day was defined as the first day of dexamethasone and insulin administration. Basal insulin is defined as insulin glargine or NPH insulin. Bolus insulin is defined as insulin lispro. Hypoglycemia was defined using the ADA guideline definition: level 1 (mild) hypoglycemia is a glucose concentration of 54 to 70 mg/dL, level 2 (moderate) hypoglycemia is a BG concentration <54 mg/dL, and level 3 (severe) hypoglycemia is a BG concentration <54 mg/dL accompanied by altered mental status and/or physical functioning that requires help from another person. 7
A sample size of 67 patients per arm was calculated to achieve 80% power using an alpha of 0.05, to detect a 20 mg/dL (±40 mg/dL) difference in the mean POC BG level. 10 All potentially eligible patients were randomized prior to screening for inclusion to ensure equitable selection of patients among study sites. Nominal data were analyzed using Chi-square test of association, and continuous data were analyzed using Kruskal-Wallis or analysis of variance test, as appropriate. Categorical data were presented as n (%) while continuous data were presented as median (interquartile range) or mean ± standard deviation. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 28.0.1.0 (IBM Corp, Armonk, New York). All tests of significance were 2-tailed with an a priori significance level of P < 0.05.
Results
A total of 1033 patients were randomized and screened for eligibility. Ninety-six patients met inclusion criteria: Sixty-seven received insulin glargine once daily, 10 received NPH insulin once daily, and 19 received both insulin glargine and NPH insulin once daily (Figure 1). The primary reason for exclusion was admission to the ICU (n = 350). Table 1 outlines the demographic and clinical characteristics of the patients included in this analysis. Body mass index was similar between the groups. Most patients were white males. There are notable differences in the baseline characteristics. The insulin glargine and NPH insulin combination group was significantly younger with a higher HgbA1c and admission BG levels than the other groups. This group also had a significantly lower CCI. Table 2 outlines non-insulin antihyperglycemic medications patients received PTA and during inpatient stay. Across all groups, the most common PTA non-insulin antihyperglycemic medications included metformin, sulfonylureas, sodium-glucose cotransporter-2 inhibitors, and glucagon-like peptide-1 receptor agonists. More patients in the insulin glargine group were prescribed non-insulin antihyperglycemic medications during admission than the other groups although this difference was not significant.
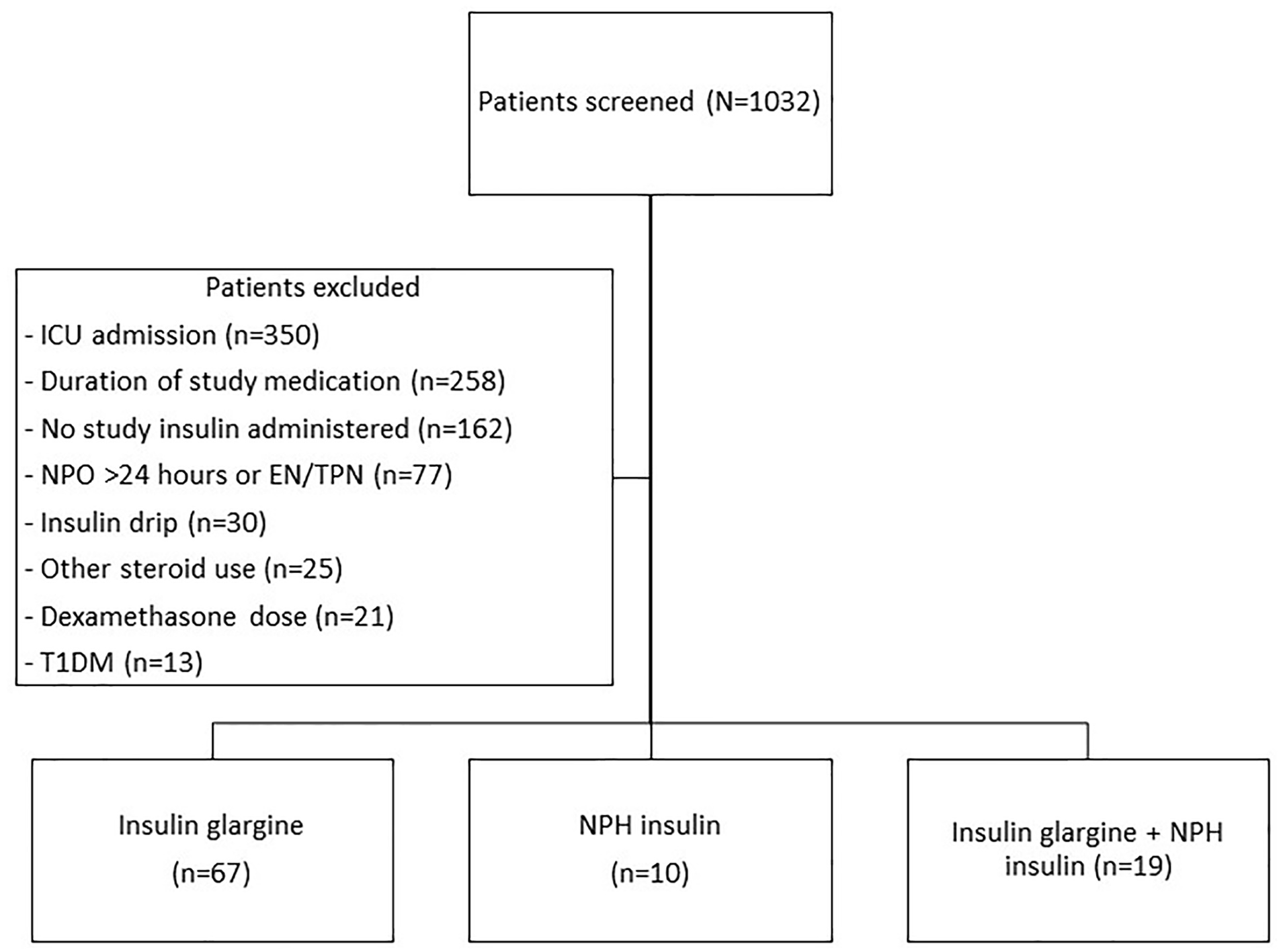
Patient enrollment.
Baseline Characteristics.
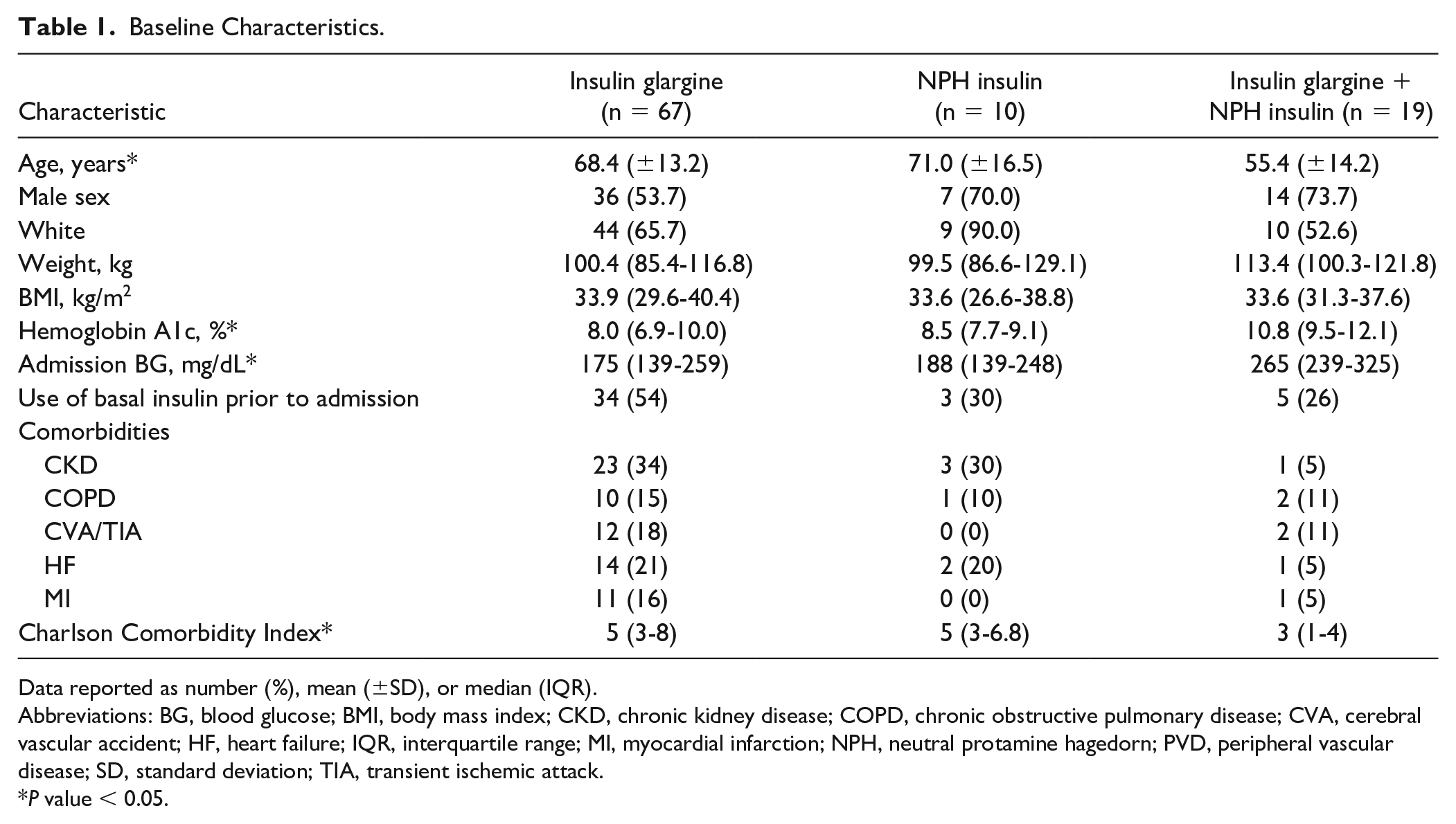
Data reported as number (%), mean (±SD), or median (IQR).
Abbreviations: BG, blood glucose; BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular accident; HF, heart failure; IQR, interquartile range; MI, myocardial infarction; NPH, neutral protamine hagedorn; PVD, peripheral vascular disease; SD, standard deviation; TIA, transient ischemic attack.
P value < 0.05.
Prior to Admission and Inpatient Use of Non-Insulin Antihyperglycemic Medications.
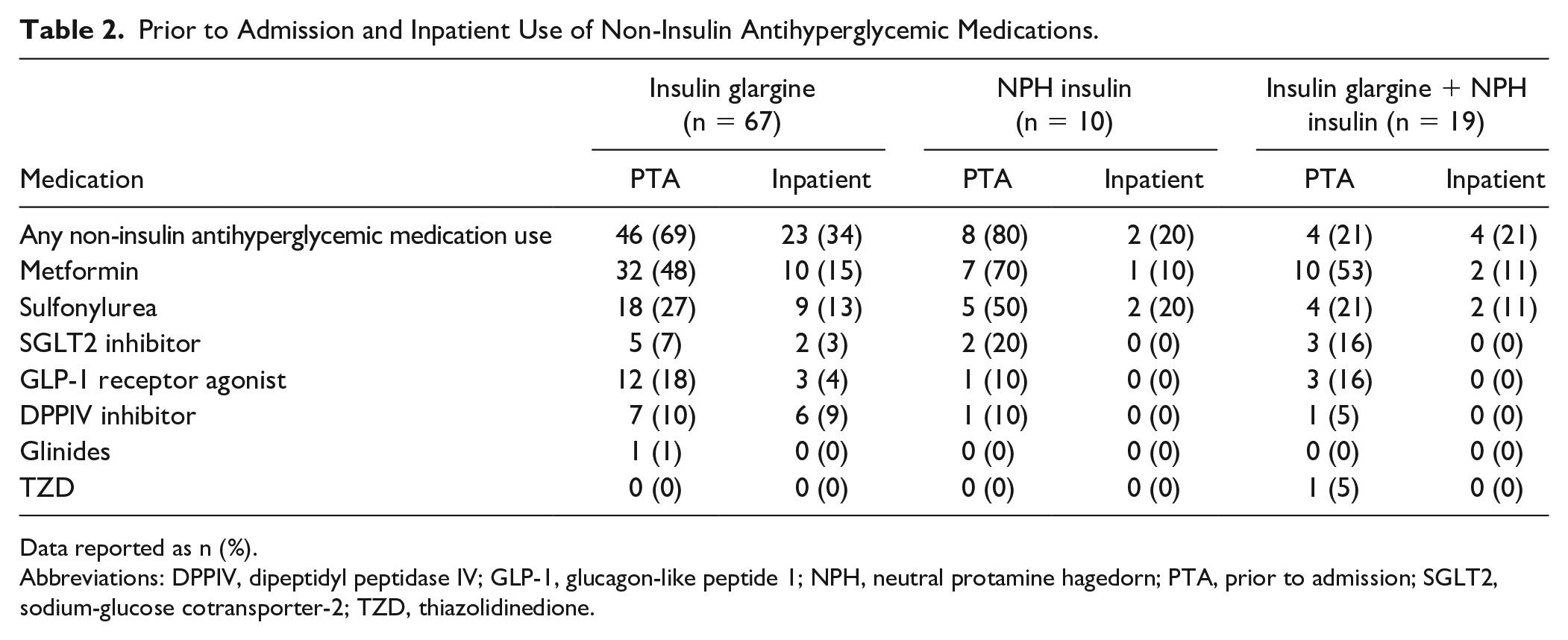
Data reported as n (%).
Abbreviations: DPPIV, dipeptidyl peptidase IV; GLP-1, glucagon-like peptide 1; NPH, neutral protamine hagedorn; PTA, prior to admission; SGLT2, sodium-glucose cotransporter-2; TZD, thiazolidinedione.
Primary and secondary outcome results are provided in Table 3. There was no difference in the mean POC BG level between the insulin glargine (245 ± 60 mg/dL), NPH insulin (234 ± 39 mg/dL), and insulin glargine plus NPH insulin (250 ± 51 mg/dL) groups, P = 0.548. BG levels were significantly elevated among all groups during the study period. All patients experienced at least 1 episode of hyperglycemia, with a median of 15 (11-18), 16 (14-17), and 15 (13-17) episodes per patient, respectively (P = 0.0746). There was a trend toward more hypoglycemic events in patients receiving NPH insulin (2 [20%]) and insulin glargine plus NPH insulin (3 [15.8%]) than in those receiving insulin glargine alone (8 [11.9%]; P = 0.702). Of note, 5 of the 8 patients who experienced a hypoglycemic event in the insulin glargine group also received a non-insulin glucose-lowering agent while in the hospital. None of the patients in the NPH insulin or insulin glargine plus NPH insulin groups who experienced a hypoglycemic event received a non-insulin glucose-lowering agent while in the hospital. Most patients who had a hypoglycemic event experienced level 1 hypoglycemia, 1 patient per group experienced level 2 hypoglycemia, and no patients experienced level 3 hypoglycemia.
Outcomes.
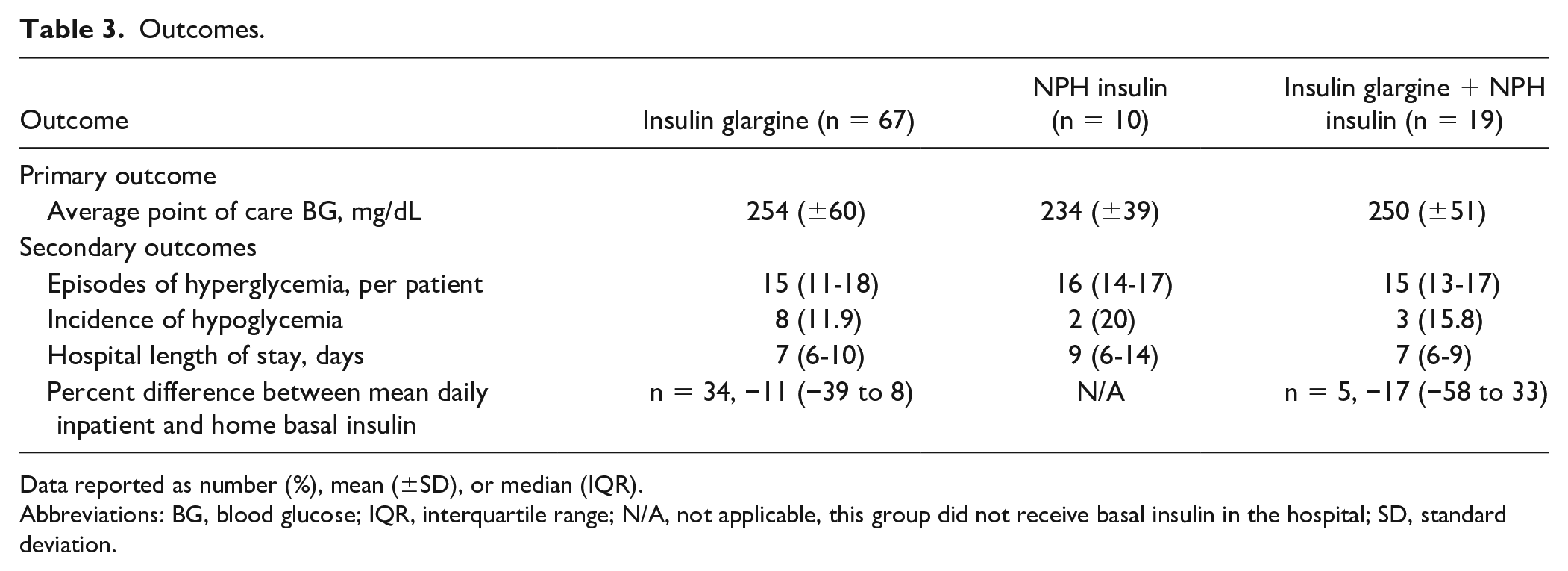
Data reported as number (%), mean (±SD), or median (IQR).
Abbreviations: BG, blood glucose; IQR, interquartile range; N/A, not applicable, this group did not receive basal insulin in the hospital; SD, standard deviation.
There was no observed difference in median LOS between the insulin glargine, NPH insulin, and insulin glargine plus NPH insulin groups (7 [6-10] days vs 9 [6-14] days vs 7 [6-9] days, respectively; P = 0.494). The percent difference in mean daily inpatient and home basal insulin doses was not different between the insulin glargine group and the insulin glargine and NPH insulin group (−11% vs −17%; P = 0.733). The average weight-based daily dose of insulin was highest in the insulin glargine group (0.3 units/kg), followed by the insulin glargine plus NPH insulin group (0.2 units/kg), and NPH insulin group (0.2 units/kg) (P = 0.138).
Discussion
The purpose of this analysis was to compare the difference in efficacy of insulin glargine and NPH insulin for the treatment of dexamethasone-induced hyperglycemia. Most of the patients in this analysis were treated with insulin glargine (70%), as recommended by the ADA guidelines. 7 No difference in the primary outcome of POC BG levels was observed in the current study. The use of dexamethasone resulted in higher insulin use during inpatient stay among patients in this study. The inpatient doses of basal insulin for patients who received both insulin glargine and NPH insulin were higher than PTA basal insulin doses.
Glucocorticoids have become the mainstay in treatment to slow disease progression in COVID-19 due to the mortality benefits seen in previous studies. 2 Although glucocorticoids reduce the mortality rate in patients with COVID-19, their use is commonly associated with uncontrolled hyperglycemia. Approximately 25% of the patient population in the RECOVERY trial had a past medical history of diabetes. 2 Of the serious adverse reactions reported with dexamethasone use, 50% of those were hyperglycemic events although no information was available if the patients had concomitant diabetes.
The ADA guidelines recommend long-acting insulins, such as insulin glargine, for glucocorticoid-induced hyperglycemia due to long-acting steroids in patients with diabetes. 7 The pharmacokinetic properties of insulin glargine are congruent with the pharmacokinetic properties of long-acting steroids, like dexamethasone. Dexamethasone has an estimated peak glycemic effect 3 hours following administration and a duration of effect lasting up to 36 hours.12,13 Insulin glargine has an onset of action 2 to 3 hours after administration and lasts about 24 hours. 3 Although these are guideline recommendations, the authors did not identify any studies specifically evaluating the optimal BG management of patients receiving dexamethasone. The National Inpatient Diabetes COVID-19 Response Group that is based in the United Kingdom recommends NPH insulin given twice daily to allow for more flexibility in dose adjustments. The weight-based starting doses would be reduced in the frail, elderly, or patients with renal insufficiency. If a patient is already on long-acting insulin, the group recommends a 20% increase in dose. 14 This project contributes to the growing body of literature on management of dexamethasone-induced hyperglycemia in patients with COVID-19.
In the current analysis, there was no observed difference in the primary outcome of POC BG level between study groups. All patients in this project had poorly controlled dexamethasone-induced hyperglycemia. These findings are consistent with previous retrospective analyses that found no difference in BG control between groups. Ruiz de Adana et al 9 and Dhital et al 10 found that BG levels were not significantly different between groups and were significantly elevated in both insulin glargine and NPH insulin groups. Results of the current study conflict with those of the study by Khowaja et al which did detect a significant difference between groups. 8 This is likely due to the small sample size of the current study. 8
Several studies showed conflicting results when investigating if insulin glargine or NPH insulin had superior BG control for use in glucocorticoid-induced hyperglycemia.8-10 Khowaja et al 8 showed that patients who received NPH insulin via a protocol, in addition to their outpatient insulin regimen, compared to once-daily basal insulin had improved BG levels when treated with glucorticoids. The current study allowed for insulin dosing by provider discretion rather than a protocol, which may have contributed to the nonsignificant results. While Khowaja et al showed a statistically significant difference in BG with the addition of NPH insulin compared to once-daily basal insulin, investigators also demonstrated poorly controlled BG for both groups (226 mg/dL vs 269 mg/dL, respectively, P < 0.0001). Notably, most patients received prednisone, in contrast to our cohort of COVID-19 patients who received dexamethasone. With an estimated peak glycemic effect of 8 hours following administration and a duration lasting 12 to 16 hours, the effects of intermediate-acting prednisone mimic the effects of NPH insulin (peak 5-7 hours; duration 12-16 hours).3,12
Ruiz de Adana et al 9 found no difference in BG control between NPH insulin and insulin glargine for the treatment of intermediate-acting glucocorticoid-induced hyperglycemia. Interestingly, this study included the intermediate-acting glucocorticoids methylprednisolone and deflazacort, which in combination with NPH insulin is in alignment of ADA guideline recommendations. 7 Dhital et al 10 reported a similar average POC BG level between NPH insulin and insulin glargine in the management of prednisone-induced hyperglycemia in hospitalized patients with or without T2DM (167 mg/dl vs 165 mg/dL, respectively; P = 0.79). The current data reveal that short-acting and intermediate-acting glucocorticoid-induced hyperglycemia may be treated with NPH insulin or insulin glargine. Previous studies that have evaluated the treatment of glucocorticoid-induced hyperglycemia did not have many patients receive dexamethasone or other long-acting glucocorticoids. Evidence is lacking to support the use of either type of insulin for the treatment of dexamethasone-induced hyperglycemia. Thus, this current study aimed to fill this gap in literature.
Given the “triple insult” of dexamethasone-induced impaired glucose metabolism, COVID-19-induced insulin resistance, and impaired insulin production due to COVID-19, it is assumed that there would be an increase in inpatient basal insulin doses compared to home basal insulin doses. 14 Previous studies in non-COVID-19 populations found that insulin requirements increased over time throughout the inpatient stay in patients receiving short-acting glucocorticoids. Dhital et al 10 found that the mean total daily insulin requirement increased 20% in patients receiving insulin glargine and 12% in patients receiving NPH insulin from day 1 to day 6 of hospitalization. The current analysis demonstrated a reduction in basal insulin doses from home to inpatient setting. This cohort included patients from the early periods of the pandemic when little was known about COVID-19 and its impact on BG levels. Perhaps providers wanted to be more cautious with the prescribing of basal insulin.
Although this project did not find a difference in BG control, it did reveal insulin-prescribing patterns of providers within the health system. Patients in the insulin glargine plus NPH insulin group were significantly younger, with higher HgbA1c values, lower CCI, and higher admission BG levels. Thus, it appears providers may be more willing to use 2 basal insulin products in younger patients with significantly elevated BG levels compared to older, higher-acuity patients.
Limitations to this analysis include the retrospective nature, specifically with regard to documentation accuracy. Home insulin requirements were obtained through the health system’s EMR utilizing the home medication list. No uniform pharmacy medication reconciliation process is in place at the health system, leading to potential for errors. As basal insulin dose requirements were examined, total daily insulin dose, including sliding scale and bolus insulin, was not considered. Oral antihyperglycemic agents were also re-initiated in some, but not all, patients, which could have confounded our results regarding BG control. The diet that was ordered during hospitalization was not recorded. The type of diet (ie, regular, carbohydrate-controlled, clear fluids, and so on) could also confound the results. Most of the patients within the analysis were white males, which may be difficult to generalize to a more diverse patient population. Our project did not reach power with only 96 patients, where 201 patients would be needed to detect a difference in the primary outcome. Had patients who were admitted to the ICU been included, the power requirement would have been met. The investigators were attempting to control for possible confounders between patient populations of different acuity. Additionally, the groups in this project were not evenly matched. This led to the possibility of confounding factors between groups, including differences in age, HbA1c, and CCI values. This project did not show a difference in the mean POC BG level between groups likely due to a small sample size, which may be prone to type II error.
Conclusion and Relevance
In conclusion, no difference in POC BG levels was observed between insulin glargine, NPH insulin, and insulin glargine plus NPH insulin for the treatment of dexamethasone-induced hyperglycemia in patients with COVID-19 and T2DM. Dexamethasone-induced hyperglycemia was poorly controlled in the insulin glargine, NPH insulin, and insulin glargine plus NPH insulin groups. Further studies are needed to evaluate the optimal insulin regimen for the treatment of dexamethasone-induced hyperglycemia.
Footnotes
Authors’ Note
Results were presented at the Ohio Pharmacy Resident Conference on May 20, 2022, and the American College of Clinical Pharmacy Global Conference on October 17, 2022.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.