
Abstract
Introduction
The combination of vancomycin and piperacillin-tazobactam (VPT) provides broad spectrum antimicrobial coverage and is commonly used as an empiric regimen for hospitalized adults with serious infections. Vancomycin alone is known to cause nephrotoxicity, and the combination of vancomycin with piperacillin-tazobactam has been associated with an even higher rate of acute kidney injury (AKI).1,2 A meta-analysis reported rates of VPT AKI ranging from 5% to 65%, with an overall rate of 22.2%, which is a notably higher incidence than piperacillin-tazobactam alone or other antibiotic combinations. 3 In addition to the increased risk of overall AKI, the combination has also been shown to result in kidney injury faster in comparison with other combination regimens. 4 The mechanism of AKI in patients on VPT therapy is not well understood; proposed mechanisms include acute interstitial nephritis (AIN), acute tubular necrosis (ATN), pseudo-nephrotoxicity, and intratubular crystal obstruction.1,5
Historically, vancomycin has been dosed using a trough-based method, with a goal trough of 10 to 15 mg/L or 15 to 20 mg/L depending on infection type. 6 The 2020 consensus guidelines for the therapeutic drug monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus (MRSA) infections recommend dosing and monitoring vancomycin using area under the 24-hour time concentration curve (AUC) over minimum inhibitory concentration (MIC) with a monitoring target of 400 to 600. 7 These guidelines recommend one of two strategies for estimating AUC: 2-level first-order pharmacokinetic equations or Bayesian dosing software. 7 Model-informed precision dosing (MIPD) involves the use of pharmacokinetic models to individualize drug dosing. Bayesian dosing software utilizes MIPD in addition to measured drug concentrations to further improve pharmacokinetic predictions. 8
The transition from trough monitoring to AUC/MIC monitoring has occurred due to previous literature demonstrating lower rates of nephrotoxicity without compromising efficacy. 7 However, to the author’s knowledge, there are no studies evaluating the incidence of VPT AKI with MIPD/Bayesian versus 2-level first-order AUC calculations. The purpose of this study is to retrospectively evaluate if MIPD/Bayesian vancomycin dosing and monitoring resulted in less overall incidence of VPT AKI compared with first-order AUC monitoring.
Methods
Population
This was a single-center, observational, retrospective cohort study conducted at a 344-bed community hospital in Alabama and deemed exempt by institutional review board. Charts of patients ages 19 and older who received concomitant VPT for at least 48 hours between November 2019 to March 2020 (2-level AUC group) and May 2021 to October 2021 (MIPD/Bayesian group) were reviewed. Exclusion criteria included creatinine clearance (CrCl) <25 mL/min at the initiation of VPT, malignancy, pregnancy, prisoner, cystic fibrosis (CF), lack of pharmacy dosing consultation, or duplicate patients.
Within this community hospital, clinical pharmacists are consulted to dose vancomycin and have pharmacy and therapeutics approval to renally adjust most antibiotics, including piperacillin-tazobactam. Piperacillin-tazobactam was dosed at 3.375 g every 8 hours with an extended infusion of 4 hours in both study arms. Vancomycin loading doses were utilized across both study arms for critically ill patients with suspected or documented serious MRSA infections, as per guideline recommendations. 7 The hospital utilized a 2-level first-order AUC-dosing strategy for vancomycin starting in 2019. Initial dosing during this time was determined via first-order pharmacokinetic equations with population estimates for the volume of distribution and eliminate rate constant. AUCs were calculated using a peak and trough obtained at steady state, with first-order equations utilized within an Excel spreadsheet. Peak concentrations were ordered 1 to 2 hours after the end of the vancomycin infusion, and trough concentrations were ordered 1 hour before the next dose.
In 2021, the hospital converted to MIPD/Bayesian dosing for vancomycin utilizing DoseMeRx (Tabula Rasa Health Care, Moorestown, NJ, USA). Models utilized within DoseMeRx included a 1-compartment model developed on the general adult population (Buelga et al), 9 a 2-compartment model developed on the general adult population (Goti et al), 10 or a 1-compartment model developed on the obese adult population (Sabourenkov et al). 11 Bayesian dosing software was utilized for initial dosing as well as subsequent dosing strategies in this arm of the study. Patients dosed via MIPD/Bayesian typically had a single vancomycin level, and the pharmacy protocol stated that levels could be drawn prior to steady state. The single drawn sample could be ordered at any point within the dosing intervals, except for during the vancomycin infusion or 1 to 2 hours after the infusion. After inputting the vancomycin level in the dosing software, the clinical pharmacist then documented the predicted AUC at steady state from DoseMeRx.
Data Collection
The hospital’s electronic health record was reviewed, along with the Bayesian dosing software. The primary investigators reviewed all data for accuracy and to ensure no missing data were present. Data were extracted manually by the primary investigator. Patients were randomly screened and incorporated into the study based on inclusion and exclusion criteria.
Outcomes
The primary endpoint was the overall incidence of AKI. AKI was assessed by 3 different definitions: the Infectious Disease Society of America (IDSA), RIFLE (risk, injury, failure, loss of kidney function, and end-stage renal disease), and Kidney Disease Improving Global Outcomes (KDIGO). IDSA AKI is defined as an increase in serum creatinine (SCr) of 0.5 mg/dL or an increase of at least 50% from baseline in at least 2 consecutive measurements during treatment to 72 hours after therapy completion. 7 RIFLE staging of AKI was defined as a 2-fold increase in SCr or glomerular filtration rate decrease by 50%; urine output (UOP) <0.5 mL/kg/h × 12 hours. 12 The KDIGO criteria was defined as an increase in SCr by ≥0.3 mg/dL (≥26.5 mmol/L) within 48 hours; or increase in SCr to ≥1.5 times baseline. 13
Secondary endpoints included target attainment (defined as an AUC:MIC between 400 and 600; assuming an MIC of 1 mg/L 7 ), timing of AKI occurrence (if applicable), magnitude of SCr increase (if applicable), need for temporary dialysis, and intensive care unit (ICU) admission at any point during the hospital stay. To evaluate the patient’s therapy, usable levels, defined as any level that was not drawn during the vancomycin infusion or within 1 hour following the end of the infusion (distribution period) were recorded. The usable levels were then evaluated to see if target attainment was achieved with the initial regimen.
Variables
Each patient’s baseline SCr, estimated glomerular filtration rate, and CrCl were also documented. The Cockcroft-Gault equation was used to estimate CrCl in mL/min. Actual body weight was used to estimate CrCl if actual body weight was less than ideal body weight; adjusted body weight was used if a patient was overweight (greater than 120% of ideal body weight per institution protocol); and ideal body weight was used if normal weight (100%–120% of ideal body weight). Concomitant nephrotoxins were documented, including diuretics, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), vasopressors, aminoglycosides, amphotericin B, and nonsteroidal antiinflammatory drugs (NSAIDs). Each included patient’s Charlson comorbidity index variables were collected. 14 Each patient’s quick sepsis-related organ failure assessment (qSOFA) score was also documented. Collection also included whether the patient received a loading dose (≥20 mg/kg), the maintenance dose, dose interval, total daily dose of vancomycin, and total length of therapy for vancomycin (days). Piperacillin-tazobactam data included the dose, dosing interval, and length of therapy (days). The length of combined VPT therapy in days was also assessed. Data were also collected regarding the indication for using these antibiotics, such as infection of unknown source, respiratory infection, central nervous system infection, skin and soft tissue infections (SSTI), osteomyelitis, bacteremia, or other.
Data Analysis
The primary outcome analyses of the overall incidence of AKI were evaluated using chi-square. Additional categorical variables were assessed using chi-square or Fisher’s exact test, as appropriate. Time to AKI and other continuous variables were evaluated using Student’s t test. The P values were 2-sided and statistical significance was defined as P < 0.05. A convenience sample of 100 patients (50 patients in each group) was selected due to time constraints and limited access to institutional data. Statistical analyses were completed using IBM SPSS Statistics for Windows, Version 28.0 (Armonk, NY) (190).
Results
A total of 286 patients were screened for inclusion in this study. A total of 100 patients were included in this study, with 50 patients in the two-level first-order AUC group, and 50 in the MIPD/Bayesian modeling group (Figure 1). The average age of patients in the two-level AUC group was 57.8 years and 58.4 years in the MIPD/Bayesian group. The majority of patients included were male (62%), and there was no difference in total body weight between the 2 groups (83.1 vs 88.4 kg, P = 0.343). Baseline SCr was 0.9 mg/dL for the 2-level first-order AUC group and 1.0 mg/dL for the MIPD/Bayesian group. In the MIPD/Bayesian group, most patients had a single level drawn pre-steady state. The full baseline characteristics are given in Table 1.
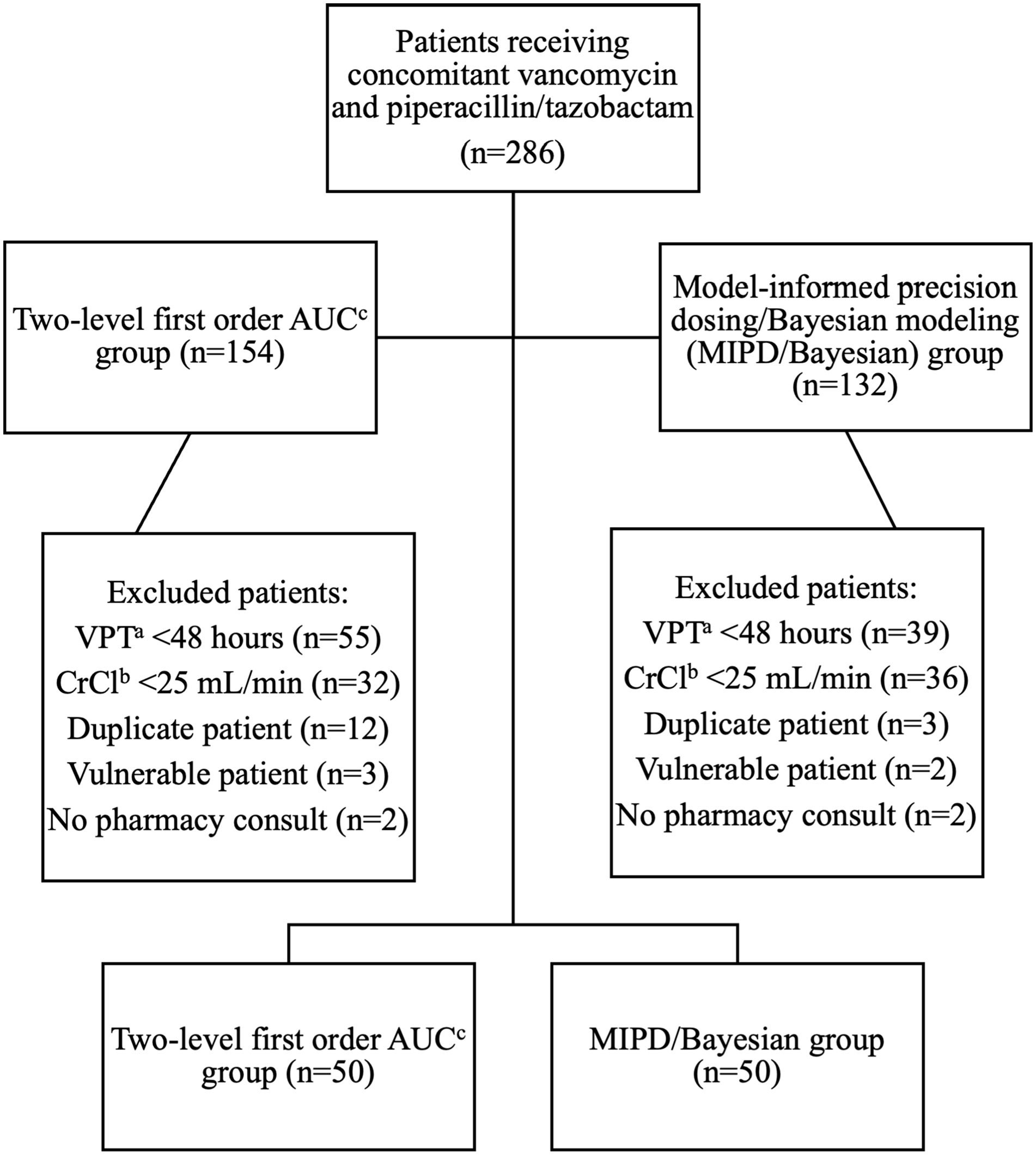
Inclusion pathway.
Baseline Characteristics.
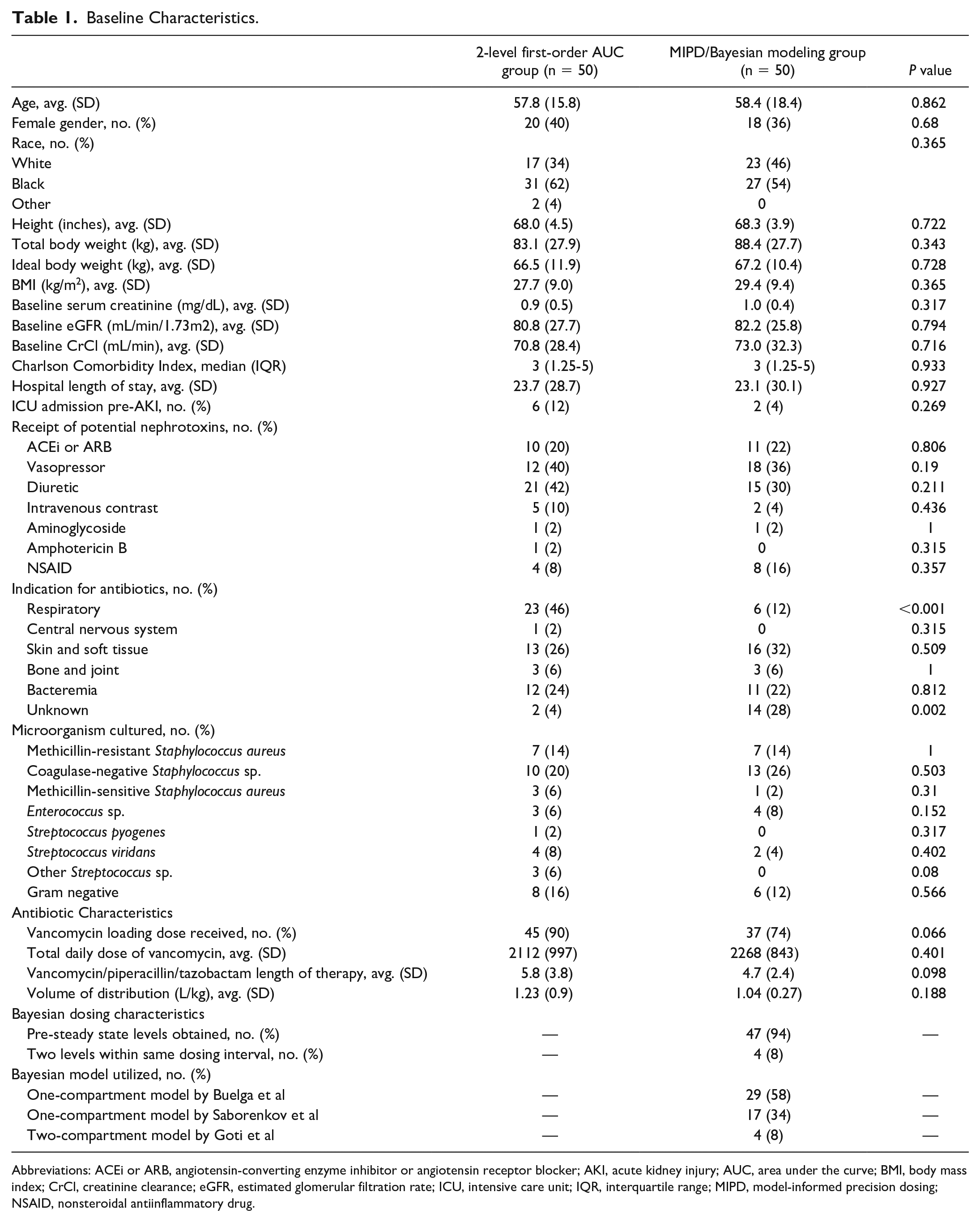
Abbreviations: ACEi or ARB, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker; AKI, acute kidney injury; AUC, area under the curve; BMI, body mass index; CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; ICU, intensive care unit; IQR, interquartile range; MIPD, model-informed precision dosing; NSAID, nonsteroidal antiinflammatory drug.
The primary outcome, the overall incidence of AKI, occurred in 14 patients (28%) in the 2-level first-order AUC group and in 6 patients (12%) of patients in the MIPD/Bayesian group (P = 0.046). A further breakdown of AKI by varying AKI definitions can be found in Table 2. After adjustment for confounders (age, body mass index, race, gender, number of concomitant nephrotoxins) via logistic regression, the odds of AKI were reduced with MIPD/Bayesian compared with 2-level first-order AUC dosing (adjusted odds ratio [aOR] = 0.269, 95% confidence interval [CI] = 0.090-0.801). Target attainment occurred in 9 patients (18%) of patients in the 2-level AUC group, while 23 patients (46%) in the MIPD/Bayesian group were predicted to achieve target attainment at steady state (P = 0.007). Among patients who developed AKI in the 2-level AUC group (n = 14), 9 patients either had therapeutic or subtherapeutic AUCs; 0 patients had supratherapeutic AUCs; and 5 patients had unknown AUCs due to lack of usable vancomycin levels. Among those who developed KDIGO AKI in the MIPD/Bayesian group (n = 6), 4 patients either had therapeutic or subtherapeutic AUCs and 2 patients had supratherapeutic AUCs. Additional secondary outcomes can be found in Table 2.
Secondary Outcomes.
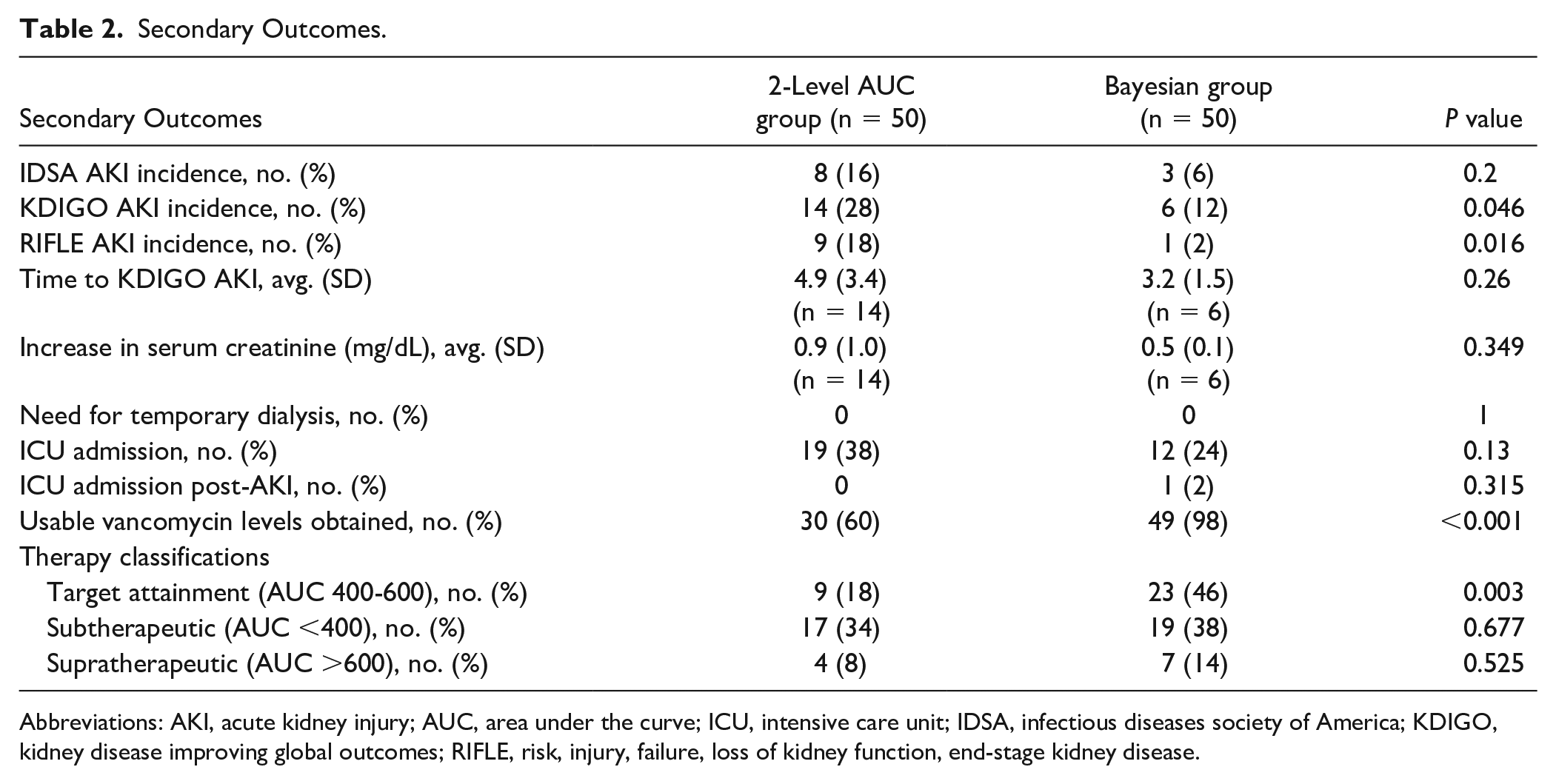
Abbreviations: AKI, acute kidney injury; AUC, area under the curve; ICU, intensive care unit; IDSA, infectious diseases society of America; KDIGO, kidney disease improving global outcomes; RIFLE, risk, injury, failure, loss of kidney function, end-stage kidney disease.
Discussion
Within this study, the incidence of AKI was reduced in patients who received vancomycin dosed by MIPD/Bayesian modeling compared with 2-level AUC dosing. There is a growing amount of literature to suggest that AUC-dosing of vancomycin may carry less risk for AKI. A recently published meta-analysis looked at trough-based versus AUC (either 2-level or Bayesian dosing software) and compared incidence of AKI for patients receiving vancomycin with or without other medications. 15 This meta-analysis found that when utilizing Bayesian software to dose vancomycin, there was a statistically significant reduction of AKI versus trough-guided dosing (OR = 0.182, 95% CI = 0.059-0.563). However, it did not specifically evaluate VPT therapy or compare the utilization of Bayesian software with the 2-level first-order method of calculating AUC. Another recent retrospective study found a reduction in AKI with Bayesian-dosed vancomycin compared with trough-guided dosing (aOR = 0.72, 95% CI = 0.58-0.89), though similar rates of AKI were seen when comparing Bayesian dosing with an AUC nomogram dosing strategy. 16
There are a few reasons why MIPD/Bayesian dosing may have resulted in a reduced incidence of AKI for patients on VPT within our study. The Bayesian dosing software provides several different models, including one for obese patients which was utilized for some of the included patients in this study. There were similar percentages of patients with supratherapeutic AUCs in both groups. However, patients in the Bayesian group study mostly had pre-steady state levels drawn, allowing dosing adjustments to be made sooner than in the AUC group, which required steady-state levels. Finally, model-informed precision dosing was utilized to determine initial dosing strategies in the Bayesian group, versus first-order pharmacokinetic equations using population assumptions in the 2-level AUC group. The difference in initial dosing strategy could also have contributed to our findings.
Our study also demonstrated an increased amount of usable vancomycin levels with Bayesian modeling, likely due to the ability to obtain a single drug concentration. One of the challenges posed by 2-level vancomycin monitoring includes the timing and usability of levels obtained during the dosing interval. An analysis of available Bayesian dosing software programs included an evaluation of using troughs as the 1 level gathered during a dosing interval versus 1 level at any time. 17 The authors reported that during the beta-elimination phase, using a trough versus other levels produced similar estimates of AUC. 17 Another study had similar findings when comparing 2-level monitoring versus 1-level Bayesian software-guided dosing. The authors found that vancomycin concentrations in the 1-level group were usable in 88.2% of patients compared with 48.3% of the 2-level monitoring group (P = 0.001). 18 Both of these results are important because it suggests the utility that 1-level Bayesian dosing does not rely on a specifically timed draw to best predict AUC and monitoring of patients.
Achieving the target AUC of 400 to 600 is important for vancomycin therapy to ensure adequate drug concentrations while mitigating the risk of toxicity. Our study found increased target attainment when utilizing MIPD/Bayesian modeling as compared with 2-level AUC calculations. A previous study compared 2-level linear AUC methods with single-level Bayesian modeling and observed target attainment rates of 50.3% (492/978) and 56.4% (552/978), respectively. 19 However, this study was performed in a single patient population in which 2 levels were obtained for all patients at steady state, and a level was subsequently hidden from Bayesian analysis for study purposes. As such, the study contrasts with our study, in which not all patients had usable vancomycin levels.
One of the strengths of this study is that it included a diverse patient population in terms of weight, source of infection, and so on. The 2 groups were generally well-matched in terms of baseline characteristics, Charlson comorbidity index, and ICU admission. Similar total daily doses of vancomycin were seen in each group, suggesting that the reduction in AKI seen with MIPD/Bayesian dosing was not simply due to a reduction in vancomycin exposure. Another strength of this study is that patients were not excluded if they were receiving other nephrotoxins. For both the 2-level AUC and MIPD/Bayesian groups, diuretics were the most frequently occurring potential nephrotoxin followed by diuretics, and then a vasopressor. This is reflective of the real-world use of these medications. Finally, we excluded patients with underlying renal dysfunction at baseline. This increases the internal validity of our findings, as any underlying kidney disease constitutes a known risk factor for the development of AKI. However, it should be noted that the results should not be applied to patients with underlying renal dysfunction.
This study does have several limitations. The first limitation is the retrospective nature of this study. The results would need to be applied with caution because the results are limited to the available information from the electronic health record at that time and the accuracy of documentation. For the 2-level AUC group, usable vancomycin levels were not available for every patient. As a result, the actual target attainment data for the 2-level AUC group is unclear. Furthermore, most vancomycin levels were obtained pre-steady state in the MIPD/Bayesian group; therefore, the AUC documented from Bayesian software represents the predicted AUC at steady-state and not the actual steady-state AUC. In the MIPD/Bayesian arm, the model utilized to select a regimen was the same model utilized to test the appropriateness of the regimen following drug levels, leading to potential self-affirming bias. The sample size was small, which means that the results may not translate into the larger population. The KDIGO AKI rate of 28% in the 2-level AUC group was higher than the overall VPT AKI occurrence rate of 22.2% in a previous meta-analysis. 3 A power analysis was not calculated a priori. In the 2-level AUC group, more patients were being treated for respiratory infections than in the MIPD/Bayesian group. In the MIPD/Bayesian arm, most patients had a single level drawn pre-steady state. Future studies should assess 1 versus 2 level Bayesian modeling, and the impact of pre-steady state versus steady state levels.
Conclusion and Relevance
In conclusion, this study demonstrated reduced incidence of AKI in patients receiving concomitant vancomycin and piperacillin-tazobactam when vancomycin was dosed with model-informed precision dosing with Bayesian modeling as compared with 2-level AUC dosing. For this patient population, MIPD/Bayesian dosing also resulted in greater target attainment defined as AUC 400-600, compared with the 2-level AUC group, as well as increased usable levels. Larger studies and data will be needed to confirm the benefit of MIPD/Bayesian dosing of vancomycin when used concomitantly with piperacillin-tazobactam.
Footnotes
Authors’ Note
This research was presented as a poster at the 2022 ASHP Midyear Clinical Meeting in Las Vegas, NV.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.