
Abstract
Background
The Infectious Diseases Society of America (IDSA) treatment guidelines recommend vancomycin or daptomycin as first-line agents for the treatment of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia. 1 However, despite the administration of appropriate initial antibiotic therapy, a delayed response is frequently observed, with blood cultures remaining positive for multiple days.2-4 Persistent MRSA bacteremia represents a prevalent and challenging clinical scenario associated with unfavorable clinical outcomes, metastatic infection, and increased health care costs.5,6 In one prospective observational cohort (n=884) of hospitalized patients with S. aureus bacteremia, at 3 university-affiliated institutions, each additional day of bacteremia was associated with a 16% increase in mortality risk (P < 0.0001). 7 Another prospective observational study found that the 90-day mortality risk doubled in patients with >1 day of S. aureus bacteremia, even when active antibiotic therapy was initiated immediately; the authors suggested that persistent bacteremia should be redefined as ≥2 days of bacteremia despite active antibiotic therapy. 8 This definition of persistence has also recently been supported by another publication. 9
A widely used approach in the management of persistent MRSA bacteremia is dual therapy, which involves the addition of an antistaphylococcal beta-lactam antibiotic to standard monotherapy with vancomycin or daptomycin. The optimal timing, duration, and antibiotic combination for the treatment of persistent or high-grade MRSA bacteremia remain unknown. The Combination Antibiotics for Methicillin-Resistant Staphylococcus aureus infection (CAMERA-2) trial 10 was terminated early because of safety concerns after the addition of an antistaphylococcal beta-lactam antibiotic (ie, flucloxacillin, cloxacillin, or cefazolin), which did not result in significant improvement in the composite endpoint of mortality, persistent bacteremia, relapse, or treatment failure. In other studies, combination therapy with flucloxacillin resulted in rapid bacteremia clearance, and combination therapy with cefazolin was associated with decreased mortality risk.11,12 However, these studies used antistaphylococcal beta-lactam antibiotics without intrinsic activity against MRSA.
Ceftaroline, a fifth-generation beta-lactam antibiotic, is the only beta-lactam with intrinsic activity against MRSA, which exerts synergy when administered with another anti-MRSA agent.13-15 In addition, in vitro findings, such as the “seesaw effect,” where beta-lactam susceptibility may be improved in the presence of decreased glycopeptide and lipopeptide susceptibility, make this an attractive option. 16 Recent reports of salvage dual therapy with ceftaroline have shown positive clinical outcomes.17,18 However, these reports lacked comparator monotherapy groups. One small study (n=40) found a mortality benefit in patients receiving combination therapy with ceftaroline compared with standard monotherapy. 19
Objective
With these limited data comparing the clinical outcomes of patients receiving dual therapy with ceftaroline and standard monotherapy, additional studies are needed to elucidate the potential risks and benefits of dual therapy. This study compared the clinical outcomes of vancomycin or daptomycin monotherapy versus dual therapy with ceftaroline for the management of high-grade or persistent MRSA bacteremia.
Methods
Study Design
The study protocol was approved by the Human Research Review Committee of the University of New Mexico (UNM) Health Sciences Center. The requirement for informed consent was waived owing to the retrospective nature of the study. This was a single-center, retrospective, and observational cohort study in which patients were categorized into 2 groups. Those who received a single anti-MRSA agent (ie, vancomycin or daptomycin) for bacteremia treatment within 24 hours of blood culture positivity were assigned to the monotherapy group. Those who received either vancomycin or daptomycin in combination with ceftaroline at any point in their treatment course, for at least 24 hours, for active bacteremia treatment were assigned to the dual therapy group.
Study Population and Data Collection
Eligible patients were adults aged 18 years or older admitted to the UNM Hospital, a 646-bed tertiary care academic medical center in Albuquerque, New Mexico, from January 1, 2014, to June 30, 2021, and diagnosed with high-grade or persistent MRSA bacteremia. Patients were excluded if they were incarcerated or had not received initial monotherapy with either vancomycin or daptomycin within 24 hours of blood culture positivity.
Relevant patient demographics and clinical and treatment data were retrospectively obtained from electronic health records and entered into a secure electronic data form by the study investigators. To assess the level of comorbidities and the severity of illness at the time of bacteremia, we calculated the Charlson Comorbidity Index and Pitt bacteremia score for each patient. Investigators noted whether consultation with the infectious diseases (ID) team was attained as this is highly recommended but not required at our institution. The ID consultation is required for the use of daptomycin or ceftaroline.
Study Outcomes and Definitions
This study aimed to compare the clinical outcomes of vancomycin or daptomycin monotherapy versus dual therapy with ceftaroline for the treatment of high-grade or persistent MRSA bacteremia. Ceftaroline was dosed 600 mg every 8 hours, except in cases where renal adjustment was necessary. The primary outcome was 30-day mortality. Secondary outcomes included microbiological relapse and antibiotic-related adverse events, such as acute kidney injury (AKI), neutropenia, and C. difficile colitis.
High-grade MRSA bacteremia was defined as MRSA growth in ≥2 sets of blood cultures on a single day. Persistent bacteremia was defined as MRSA growth in blood cultures on ≥2 consecutive days. Bacteremia clearance was defined as a negative culture set on the nearest day following a positive culture.
Source control was defined as intravenous catheter removal, debridement (including amputation), drainage, valve replacement, or chest tube placement based on the infection source. Microbiological relapse was defined as new bacteremia (after >7 days of negative blood culture), with at least 1 set of positive blood cultures for MRSA; microbiological relapse was captured for up to 6 months after MRSA treatment completion.
To study the relationship between combination therapy and adverse events, we created a composite variable (ie, any antibiotic-related adverse event) that indicated whether a patient experienced one or more of the following: AKI, neutropenia, or C. difficile colitis. Acute kidney injury was defined as an increase in serum creatinine level (≥0.3 mg/dL within 48 hours of anti-MRSA antibiotic initiation, or ≥1.5 times from baseline). Neutropenia was defined as a new onset of an absolute neutrophil count of <1500 cells/mm3 while on anti-MRSA antibiotic therapy. In addition, C. difficile colitis was defined as symptoms plus a positive C. difficile polymerase chain reaction or enzyme-linked immunosorbent assay (ELISA) after anti-MRSA antibiotic therapy initiation and up to 30 days after treatment discontinuation.
Statistical Analysis
For descriptive statistics, univariate analysis of categorical variables was performed using the χ2 and Fisher exact tests. Yates continuity correction was used for the sparse variables. Univariate analysis of continuous variables was performed using 2-sample t tests for normally distributed variables and Wilcoxon rank-sum tests for non-normally distributed variables. Normality was assessed through visual inspection and formally using the Shapiro-Wilk test. Descriptive summaries of normally distributed continuous variables were reported using means and standard deviations, whereas medians and interquartile ranges were used for non-normal variables. All the hypothesis tests were conducted at an alpha level of .05.
Multiple logistic regression with inverse probability of treatment weighting (IPTW) was used to test the association between the treatment variable (dual therapy) and dichotomous outcome variables (eg, 30-day mortality, microbiological relapse, and any antibiotic-related adverse event). Dual therapy was modeled as a dichotomous covariate, indicating whether the patient was treated with a combination of ceftaroline and vancomycin or daptomycin.
The propensity score model used to estimate the average treatment effect weights was constructed using a gradient boosting machine by regressing the treatment variable on covariates shown to be associated with the outcome, as well as those that demonstrated evidence of confounding. Specifically, confounding covariates were defined as those that resulted in a significant change in the treatment variable coefficient estimate when included in a multiple regression model (eg, %Δβ≥20). Covariate balance after weighting was assessed using standardized mean differences (SMDs) between the dual therapy and monotherapy groups. Variables with an SMD <0.1 were considered balanced. Residual confounding from unbalanced variables was addressed by including these variables as covariates in the final weighted model.
Results
Patient Baseline Characteristics
We identified 160 patients with high-grade or persistent MRSA bacteremia during the study period. Three patients were excluded because of incarceration and 2 were excluded because of initial bacteremia treatment with an anti-MRSA agent other than vancomycin or daptomycin (Figure 1). The final study population comprised 155 patients. The subjects had a mean age of 54.5 years (SD 16.6) and were predominantly male (96/155, 61.9%). Most patients self-identified as white (111/155, 72%) and of non-Hispanic or Latino ethnicity (89/155, 57.4%). The most common comorbidities in the cohort were substance use disorders (78/155, 50.3%) and diabetes mellitus (73/155, 47.1%). Both groups demonstrated a balanced distribution of the Charlson Comorbidity Index and Pitt bacteremia score.
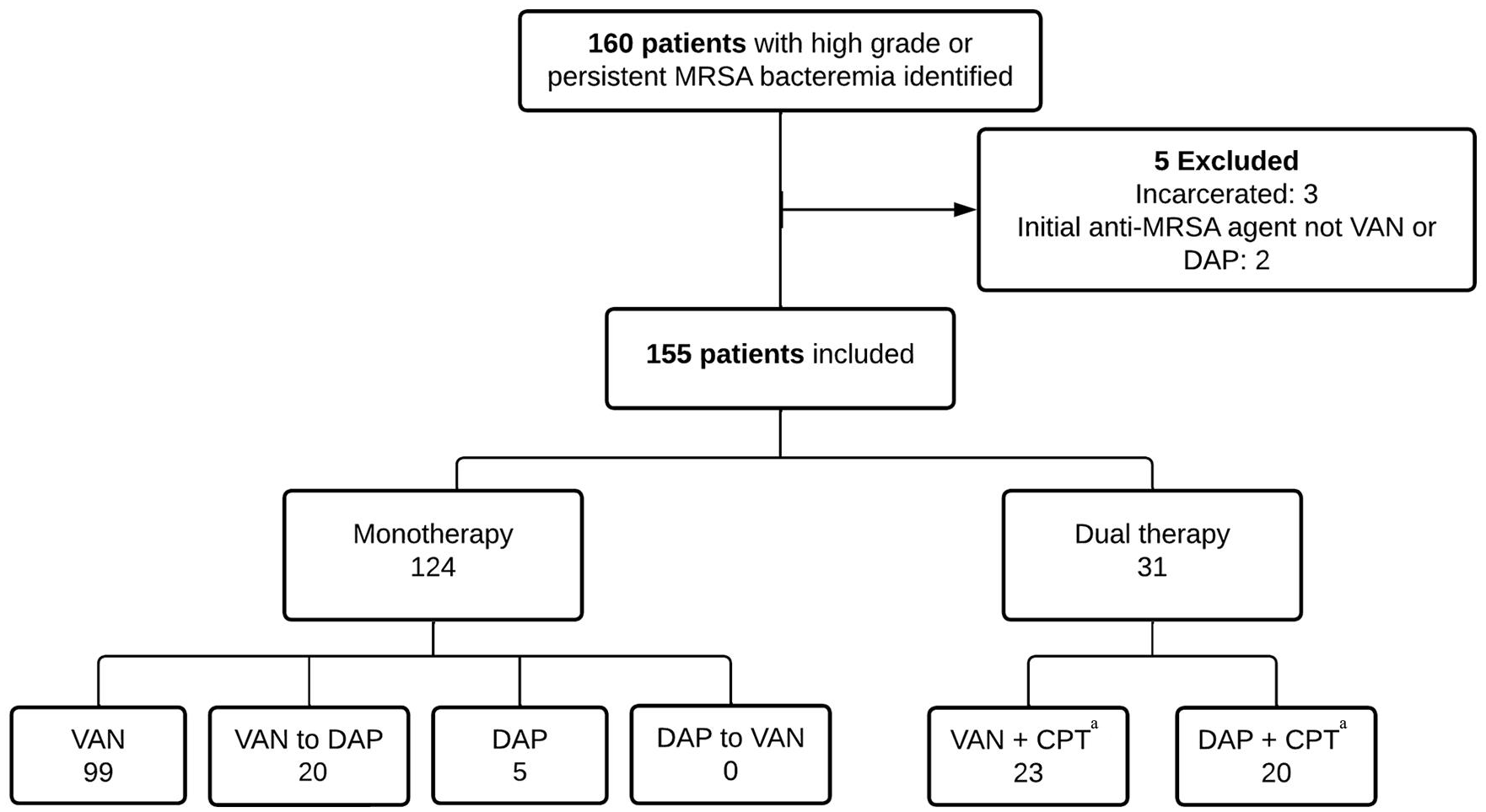
Study population.
The baseline characteristics were well balanced between the 2 groups, except for the occurrence of persistent bacteremia, ID consultation, and infective endocarditis diagnosis (Table 1). Most patients in the dual therapy group had persistent MRSA bacteremia (21/31, 67.7%) compared with those in the monotherapy group (36/124, 29%). All patients in the dual therapy group had ID consultations compared with those in the monotherapy group (103/124, 83.1%). Infective endocarditis was more commonly diagnosed in the dual therapy group (15/31, 48.4%) than in the monotherapy group (32/124, 25.8%).
Baseline Demographic and Clinical Characteristics of the Cohort (N = 155).
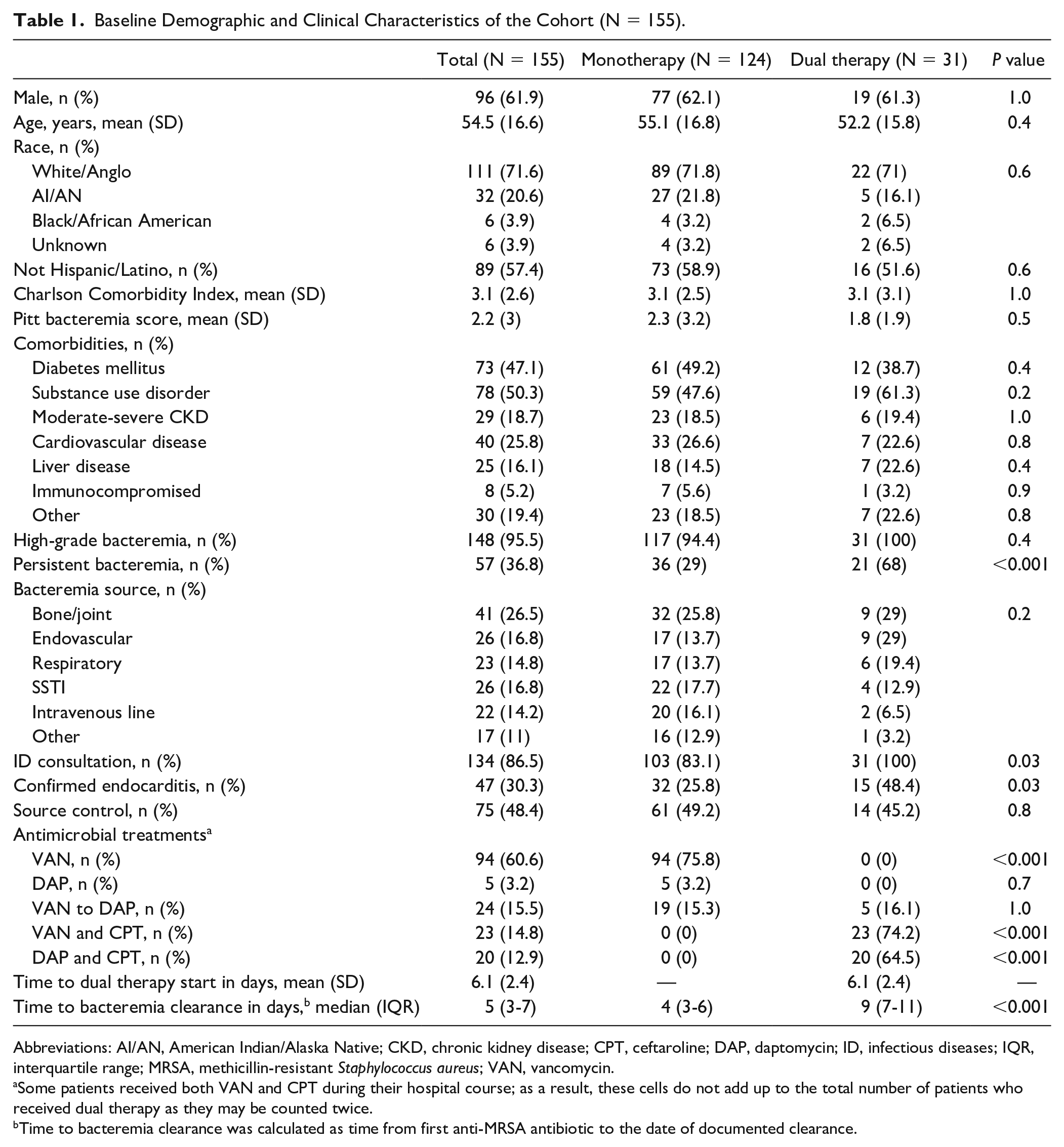
Abbreviations: AI/AN, American Indian/Alaska Native; CKD, chronic kidney disease; CPT, ceftaroline; DAP, daptomycin; ID, infectious diseases; IQR, interquartile range; MRSA, methicillin-resistant Staphylococcus aureus; VAN, vancomycin.
Some patients received both VAN and CPT during their hospital course; as a result, these cells do not add up to the total number of patients who received dual therapy as they may be counted twice.
Time to bacteremia clearance was calculated as time from first anti-MRSA antibiotic to the date of documented clearance.
Regarding the antimicrobial treatments in our cohort, the mean vancomycin trough level was therapeutic at 18.3 mg/L. The mean daily daptomycin dose was 8 mg/kg. The mean total daily ceftaroline dose was 1692 mg, with underdosing based on renal function observed in three patients. The mean time to dual therapy was 6.1 days (SD 2.4) and the median duration was 8 days (interquartile range [IQR] 4, 11).
Clinical Outcomes
The 30-day mortality rate in the monotherapy group was 23.4% (29/124) compared with 22.6% (7/31) in the dual therapy group, with no statistically significant difference between the 2 groups (P = 1.0). The microbiological relapse rate did not differ between groups (6.5%, P = 1.0). The most common antibiotic-related adverse event in our cohort was AKI, with a higher rate in the monotherapy group (24/124, 19.4%) than in the dual therapy group (3/31, 9.7%). Neutropenia (9/124, 7.3%) and C. difficile colitis (6/124, 4.8%) were reported only in the monotherapy group.
In IPTW analysis, there was no significant difference in the risk of 30-day mortality between patients receiving dual therapy and those receiving monotherapy (adjusted risk ratio [ARR] 1.38, 95% CI 0.64-2.41, P = 0.38). However, there was a lower risk of 30-day mortality for patients with an ID consultation (ARR 0.27, 95% CI 0.07-0.95, P = 0.04) and a higher risk of mortality with a higher Pitt bacteremia score (ARR 1.44, 95% CI 1.25-1.64, P < 0.001) and increased age (ARR 1.04, 95% CI 1.01-1.06, P = 0.001).
No significant association was observed between dual therapy and microbiological relapse (ARR 0.95, 95% CI 0.31-2.73, P = 0.93). Dual therapy was associated with a lower risk of any antibiotic-related adverse events (ARR 0.45, 95% CI 0.21-0.89, P = 0.02). Patients with persistent bacteremia had a higher risk of adverse events (ARR 1.88, 95% CI 1.25-2.49, P = 0.004). Table 2 lists the IPTW results for the dichotomous clinical outcomes.
The IPTW Regression Table for Dichotomous Clinical Outcomes.

Results are expressed as ARR (95% CI), P value. The AUROC for the mortality, microbiological relapse, and adverse event models were 0.88, 0.56, and 0.63, respectively.
Abbreviations: ARR, adjusted risk ratio; AUROC, area under the receiver operating characteristic; ID, infectious diseases; IPTW, inverse probability of treatment weighting.
Discussion
Severe MRSA infections, including bacteremia, remain a common health problem because of their significant morbidity and mortality.5,20,21 Persistent bacteremia has been associated with poor clinical outcomes, such as metastatic infections, with vancomycin failure rates of up to 50%.3,21,22 The prevalence of MRSA bacteremia was well demonstrated in this study in which 95.5% (148/155) of the cohort experienced high-grade bacteremia and 36.8% (57/155) had persistent bacteremia. The continued clinical threat posed by MRSA bacteremia highlights the need for the optimization of treatment strategies.
Current IDSA treatment guidelines advise source control in addition to dual antibiotic therapy in cases of persistent bacteremia or antibiotic failure. 1 Previous studies have demonstrated an association between dual therapy and improved clinical outcomes;11,18,19,23,24 however, few studies have specifically compared monotherapy with dual therapy with ceftaroline. Our study focused on evaluating differences in clinical outcomes between monotherapy and dual therapy with ceftaroline.
Our findings are consistent with previously published data, suggesting that dual therapy does not provide a mortality benefit over monotherapy, after controlling for confounding factors.10,25 However, the mean time to dual therapy initiation in our cohort was 6.1 days (SD 2.4). Considering the suggested updates to the definition of persistent bacteremia 9 , dual therapy in our cohort may have been initiated too late to provide a mortality benefit. Casapao et al 26 suggested that early initiation of dual therapy may result in a mortality benefit.
It is also worth noting that patients in this study received adequate doses of antibiotics. Patients receiving vancomycin achieved concentrations within the target therapeutic range. The average daily daptomycin dose was 8 mg/kg.
We found that patients who underwent ID consultations had a 73% lower risk for 30-day mortality. Consultation with an ID physician has been previously associated with a lower risk of death from MRSA bacteremia.27,28 Our results further emphasize the need for ID consultation in patients diagnosed with Staphylococcus aureus bacteremia to improve the clinical outcomes related to these infections.
Our study showed a safety signal for dual therapy and a lower risk of antibiotic-related adverse events. This contradicts the findings of Tong et al 10 in which the trial was terminated because of safety concerns in the dual therapy group. However, it is important to highlight that vancomycin was predominantly used over daptomycin (>90%) and that ceftaroline was not a beta-lactam antibiotic evaluated in that clinical trial, which may have contributed to the discrepant results. Although vancomycin is associated with a high risk of nephrotoxicity and may contribute to increased adverse event rates, the dual therapy group had a lower AKI rate (9.7%) than the monotherapy group (19%). Vancomycin was predominantly used in both treatment groups, with only 16.1% of the patients switched to daptomycin in dual therapy with ceftaroline. In addition, dual therapy was instituted for a relatively short average course (8 days), which may not allow enough time for adverse events such as neutropenia to manifest. Beta-lactam antibiotic-induced neutropenia usually occurs after at least 2 weeks of therapy. These results suggest that the choice of antibiotics may be more important in terms of safety. However, it may still be wise to limit the use of ceftaroline to cases of active bacteremia to minimize collateral damage due to prolonged antibiotic exposure.
No association was observed between microbiological relapse and dual therapy. Several previous studies have demonstrated the statistical significance of this clinical outcome when directly comparing dual therapy with the standard of care with vancomycin or daptomycin monotherapy. Alosaimy et al. 24 concluded that 60-day recurrence was significantly reduced when combination therapy with vancomycin or daptomycin and any beta-lactam was used, compared with monotherapy. Similarly, Johnson et al. 29 compared dual therapy with ceftaroline and daptomycin with the standard of care and found a statistically significant reduction in recurrence within 60 days. Apart from these studies, previously published data have failed to demonstrate a statistically significant effect on microbiological relapse.
Recurrent bacteremia is often associated with complicated infections, such as endocarditis, in which source control is not adequately achieved, leading to incomplete bacterial eradication despite appropriate antimicrobial therapy. In our cohort, a significantly higher proportion of patients in the dual therapy group were found to have endocarditis; however, the rate of source control was not significantly different between the groups. Therefore, it is plausible that no difference was observed in microbiological recurrence, given the similar rates of source control. Although our findings appear to be congruent with those of previously published literature, further studies are necessary to elucidate the clinical impact of dual therapy on microbiological relapse as we would expect to see higher rates of recurrence in patients with deep-seated infections without adequate source control.
Overall, this analysis enhances the current knowledge regarding the use of dual therapy for the treatment of MRSA bacteremia by providing further evidence that there is no significant difference in 30-day mortality between patients treated with dual therapy and standard monotherapy. Although dual therapy with ceftaroline does not confer a mortality benefit over monotherapy, it can be considered a safe alternative in cases of persistent or high-grade MRSA bacteremia. In addition, in the era of antibiotic stewardship, our results suggest that dual therapy with ceftaroline can be utilized without an increased risk of adverse events when administered for a short duration. This provides a viable strategy for optimizing antibiotic use in MRSA bacteremia. Our study also underscores the vital role of ID consultations in patient care. This highlights the value of collaboration between specialists in managing MRSA bacteremia cases.
This study has limitations that are largely centered on its small sample size and retrospective design, in particular, the small sample size coupled with rare outcomes, such as mortality and infrequent use of dual therapy, at our institution. In addition, 30-day mortality, microbiological relapse, and antibiotic-related adverse event outcomes may have been censored because patients could have sought medical care at other institutions after hospital discharge. In addition, the study design lends itself to potential selection bias because the patients were categorized into monotherapy and dual therapy groups based on specific criteria. Although the mean Charlson Comorbidity Index and Pitt bacteremia score were similar between the groups, the choice of therapy may have been influenced by various clinical factors that may not have been accounted for. Finally, with a mean Pitt bacteremia score of 2, both treatment groups lacked severely ill patients. This raises the question of whether our findings can be applied to individuals with a high degree of illness in which dual therapy may be beneficial.
Conclusion and Relevance
This single-center retrospective study suggests that dual therapy with ceftaroline for high-grade or persistent MRSA bacteremia, compared with monotherapy, did not yield a significant reduction in the 30-day mortality risk. However, when used for short durations (≤8 days), dual therapy appears to be safe with no increased risk of antibiotic-related adverse events, providing a strategic option for clinical practice. Our study also highlights the critical role of ID consultations in improving patient outcomes, with a 73% reduction in the mortality risk. These insights guide clinicians to consider the timing and duration of dual therapy and to reinforce antibiotic stewardship efforts. Large-scale, prospective, and randomized controlled trials are needed to provide conclusive evidence regarding the potential benefit of dual therapy with ceftaroline for MRSA bacteremia treatment beyond its adverse event profile.
Footnotes
Author Contributions
MGC conceived the original idea for this article and supervised this project. MGC, MLB, MJB, and BJ wrote the manuscript. CNR and CMT provided the initial patient data set. MGC, MJB, LMA, and JK collected data from electronic health records. MLB, BJ, and TFB provided advice on the study methods and design. MLB performed statistical analyses. All authors discussed the results; reviewed, edited, and provided critical feedback on the manuscript; and approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
As a result of the nature of this research, patients have not consented to having their data shared publicly.