
Abstract
Objective
The anticholinergic syndrome (AS) is a constellation of signs and symptoms resulting from inhibition of acetylcholine at muscarinic receptors. 1 Key manifestations include mydriasis, dry skin and mucous membranes, tachycardia, hyperthermia, confusion, and delirium. Central, peripheral, and mixed subtypes are recognized. Anticholinergic syndrome typically results from therapeutic exposure, overdose, or drug interactions involving anticholinergic agents; reports involving antibiotics are exceedingly rare. 1
Vancomycin is a glycopeptide antibiotic widely used for catheter-related infections in patients with chronic kidney disease (CKD). 2 Its pharmacokinetics—limited lipophilicity, moderate volume of distribution, and almost exclusive renal elimination—require careful dose adjustment in individuals with reduced glomerular filtration or those undergoing hemodialysis. 3 Penetration into the central nervous system (CNS) is minimal, and reports of vancomycin-associated neurotoxicity are scarce, usually linked to rapid infusion or elevated serum concentrations. Described manifestations include encephalopathy, headache, altered mental status, confusion, seizures, and somnolence with sexual dysfunction.4,5
Patients with stage 5 CKD historically present a high risk of medication overdosing and inadequate drug administration due to fluid restrictions. 3
Vancomycin should ideally be infused slowly in diluted solution (2.5-5.0 mg/mL) at a rate not exceeding 10 mg/min. In fluid-restricted patients, solutions of 500 mg/50 mL or 1000 mg/100 mL may be used, though the wide range of acceptable volumes may contribute to preparation errors. Higher concentrations further increase the risk of infusion-related adverse events. 2
Case
A 61-year-old man (dry weight 41 kg) from Mexico with type 2 diabetes mellitus (managed with dapagliflozin), systemic arterial hypertension (on nifedipine), and stage 5 CKD on thrice-weekly hemodialysis (on B-complex vitamins and erythropoietin) presented on August 31, 2025, with pulsatile headache (visual analog scale [VAS] 7/10) and nausea.
Upon arrival to the emergency department, vital signs were: blood pressure 90/56 mm Hg, heart rate 80 bpm, oxygen saturation 80%, and temperature 38.0°C. He was alert and oriented; physical examination was otherwise unremarkable. Supplemental oxygen was initiated, raising saturation to 96%. Due to hypotension, norepinephrine infusion was started, along with antipyretic and analgesic therapy (acetaminophen). The patient was stabilized and admitted to the internal medicine ward on September 1, 2025.
On admission, he had a Glasgow Coma Scale score of 15, was alert and oriented, and hemodynamically more stable (BP 100/80 mm Hg, HR 80 bpm, SpO₂ 96%, T 37.0°C). Nephrology and infectious disease teams evaluated him for suspected catheter-related infection. He was prescribed oral acetaminophen 1 g every 8 hours as needed, tramadol 25 mg IV every 8 hours as needed (VAS >7), atorvastatin 40 mg daily, cholecalciferol 5000 IU daily, meropenem 500 mg IV every 24 hours, and vancomycin 1 g IV every 12 hours. Due to fluid restriction, vancomycin was infused over 60 minutes in 100 mL.
Catheter and blood cultures were obtained. Laboratory abnormalities included procalcitonin 131 ng/mL, potassium 5.6 mmol/L, urea 171 mg/dL, creatinine 9.2 mg/dL, creatinine clearance 5.53 mL/min, leukocytes 17 K/µL, C-reactive protein 15 mg/dL, and lactate 2.1 mmol/L. ECG revealed inverted T waves in V5–V6. Antihyperkalemic therapy was initiated, and the patient underwent hemodialysis. Staphylococcus aureus sensitive to vancomycin was isolated from the catheter culture.
By the end of the first and second hospital days, the patient was hemodynamically stable, afebrile, and no longer required supplemental oxygen. Inflammatory markers improved: procalcitonin decreased to 78 ng/mL; potassium 5.1 mmol/L; urea 89.9 mg/dL; creatinine 7.4 mg/dL; leukocytes 12 K/µL; CRP 5 mg/dL; and lactate 1.4 mmol/L.
However, after the third vancomycin dose, he developed panic sensations. After the fourth dose, he presented transient amaurosis, tachycardia (110 bpm), hyperthermia (39°C), xerostomia, xeroderma, worsening confusion, agitation, and panic. A drug-related adverse reaction was suspected; vancomycin was discontinued and he underwent hemodialysis. Symptoms resolved completely thereafter.
Ceftazidime 1 g every 24 hours was initiated to continue antimicrobial therapy. The patient remained stable and was discharged after 8 hospital days, following catheter replacement. The Naranjo algorithm score was 10, indicating a definite adverse drug reactions (ADRs) consistent with a mixed anticholinergic-type syndrome, not previously associated with vancomycin.
Discussion/Conclusions
In stage 5 CKD, vancomycin dosing must be individualized. Guidelines recommend a loading dose of 20 to 25 mg/kg followed by maintenance doses adjusted by therapeutic drug monitoring, usually with extended intervals (>24 hours) in patients with creatinine clearance <15 mL/min receiving intermittent hemodialysis. 6 Based on pharmacokinetic simulation (Figure 1a), the patient should have received approximately 500 mg at minimum every 48 hours. Instead, he received 8-fold the appropriate dose over the same period.
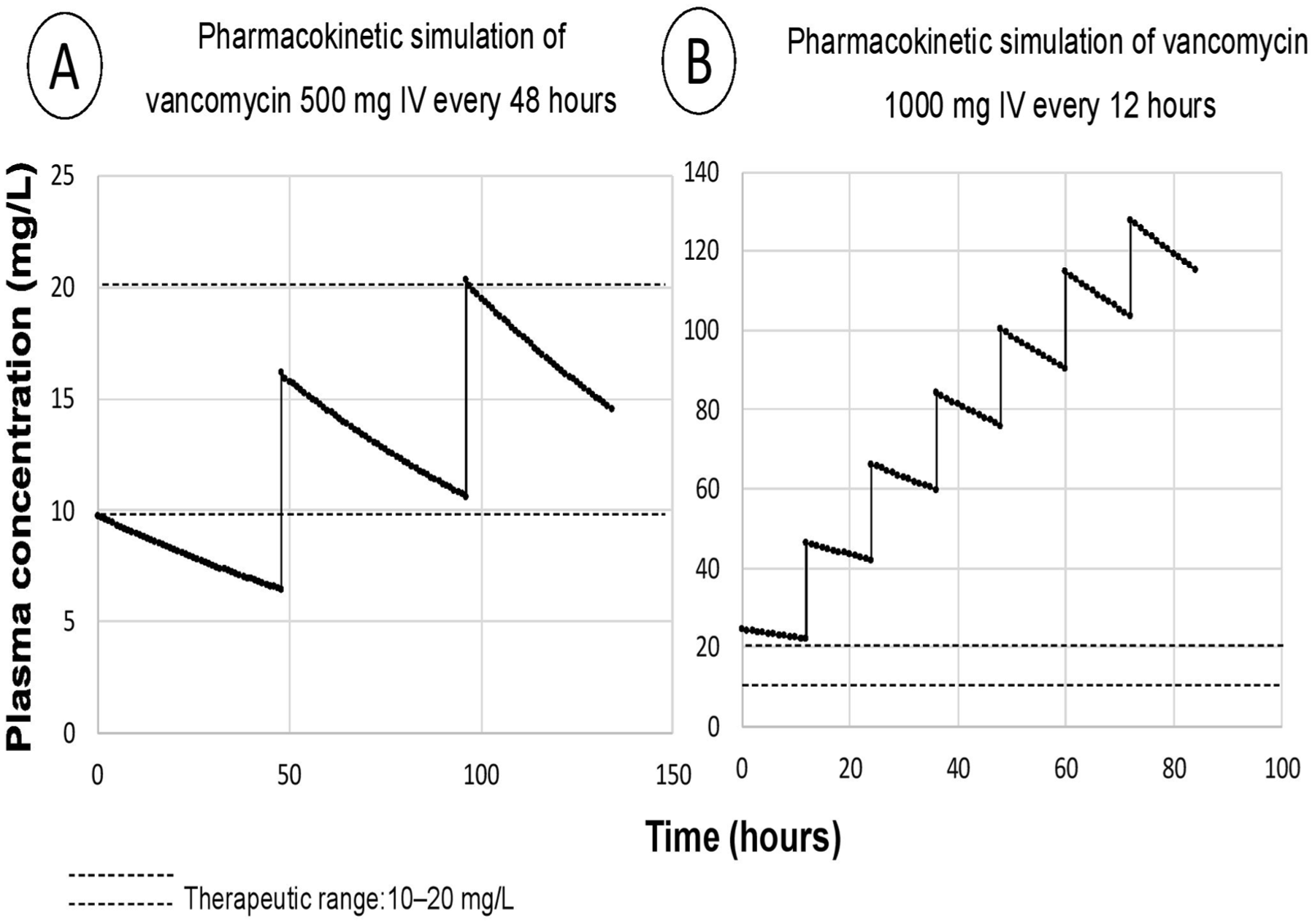
Pharmacokinetic simulations comparing 2 vancomycin dosing regimens in a patient with end-stage renal disease. (a) Predicted concentrations following 500 mg IV every 48 hours, remaining largely within the therapeutic range. (b) Simulated accumulation and supratherapeutic concentrations following 1000 mg IV every 12 hours, illustrating vancomycin overexposure.
The pharmacokinetic simulation for the regimen administered during hospitalization (Figure 1b) revealed clear vancomycin accumulation and extremely elevated vancomycin levels (peak 80 mg/L; valley 60 mg/L), correlating with the onset of mixed anticholinergic-type syndrome. Furthermore, the maximum recommended infusion rate is 10 mg/min; the patient received 16.6 mg/min, further increasing the risk of accumulation. 5
Because vancomycin is a hydrophilic macromolecule, its penetration into the CNS is limited. Central nervous system entry typically occurs only when the blood-brain barrier (BBB) is disrupted, such as during CNS infections. 7 Elevated systemic levels after oral vancomycin have been reported in critically ill patients—despite its lack of enteral absorption—suggesting increased gastrointestinal and systemic permeability in states of inflammation, renal impairment, high doses, or prolonged therapy. 8
Existing reports of vancomycin-induced neurotoxicity share 2 features: inflammatory states and toxic plasma concentrations. Examples include seizure episodes in a patient with neuroblastoma and extremely elevated vancomycin levels (peak 59.5 mg/L; valley 38.6 mg/L), 9 and encephalopathy associated with vancomycin alone or combined with cefepime in individuals with renal dysfunction.10,11
Central AS manifests with delirium, hallucinations, confusion, and agitation. 1 The patient developed confusion, agitation, and panic temporally associated with vancomycin administration; symptoms worsened after re-exposure and resolved after discontinuation. Although CKD can cause uremic encephalopathy, 12 the patient showed no clinical features of this condition, and symptoms appeared after hemodialysis. Glasgow Coma Scale scores and mental orientation were normal before vancomycin exposure.
The pulsatile headache is associated with renal replacement therapy and potential fluid overload, although its severity is influenced by the patient’s underlying clinical condition. Adherence to the prescribed hemodialysis regimen generally reduces this risk. Moreover, the confusion, agitation, and panic symptoms resolved following discontinuation of the medication, indicating the absence of any pre-existing condition that could account for these manifestations. The elevated levels of procalcitonin, C-reactive protein, and lactate, along with the initial hypotension observed in the emergency department, are indicative of septic shock, which in some cases can lead to sepsis-associated encephalopathy. This condition is characterized by neurocognitive dysfunction, including delirium, seizures, and persistent cognitive deficits. 13 These conditions were not present in the patient, and the septic shock was already in a remission phase, as evidenced by decreasing procalcitonin, C-reactive protein, and lactate levels, as well as the normalization of blood pressure and the absence of fever. Therefore, sepsis can be excluded as the primary cause. Hyperthermia was initially observed in the emergency department; however, it progressively declined alongside the improvement of septic shock and the administration of antipyretic therapy. The patient remained afebrile upon admission to internal medicine. Notably, the most significant elevation in body temperature occurred following the administration of vancomycin. In AS, inhibition of acetylcholine impairs sweating (thermoregulation) and induces vasodilation, preventing heat dissipation and resulting in hyperthermia and xeroderma. 1
Patients with CKD often present dermatologic alterations such as xerosis, hyperpigmentation, and uremic pruritus. 14 The patient reported the use of moisturizing creams and denied frequent episodes of uremic pruritus, and no diagnosis of xerosis had been established. The initial report of diaphoresis contrasted with the xeroderma observed hours later; a similar pattern was noted with the onset of xerostomia. Although xerostomia may occur as a manifestation of CKD, the patient described only extreme oral dryness and a metallic taste following the administration of vancomycin. The blockade of acetylcholine muscarinic receptors—primarily M3—in peripheral tissues inhibits the stimulation of exocrine glands, thereby leading to dryness of the skin and oral mucosa. 15
Anticholinergic drugs inhibit the ciliary muscle, and when the pupil is dilated (mydriasis), excessive light enters the eye. In addition, the iris sphincter muscle is unable to adjust the pupillary diameter to achieve proper focusing, resulting in visual impairment. 16 This event was observed in association with vancomycin administration. Among the differential diagnoses that could contribute to visual loss is diabetes mellitus 17 ; however, this condition was well controlled in the patient, who demonstrated adherence to treatment and consistently maintained glucose levels within normal ranges.
Tachycardia is a recognized sign of peripheral AS, 15 and in this case it occurred only after vancomycin accumulation. In contrast, potassium disturbances typically produce bradycardia. The electrocardiogram showed inverted T waves in leads V5–V6, a finding consistent with ischemic heart disease, ventricular dysfunction, or secondary alterations associated with CKD and systemic hypertension. However, these abnormalities did not correlate with the episode of tachycardia, which resolved completely following discontinuation of the medication.
A comparison of the clinical manifestations with various syndromes—such as serotonin syndrome, neuroleptic malignant syndrome, sympathomimetic toxidrome, and extrapyramidal symptoms—was conducted, and none consistently reproduced the patient’s pattern of findings, except for a mixed anticholinergic-type syndrome. 1 Posterior reversible encephalopathy syndrome was also excluded, as it typically presents with epileptic seizures.10,11
A drug–drug interaction (DDI) analysis was performed using Micromedex, covering the period from the patient’s admission to the onset of symptoms, in order to rule out any combined pharmacologic effect that could explain the observed manifestations. No DDIs were identified, reinforcing the conclusion that the most plausible cause of the neurological symptoms was the accumulation of the antibiotic. The only medication prescribed during hospitalization with the potential to induce similar manifestations was tramadol, as cases of serotonin syndrome have been reported with its use. 18 However, tramadol was prescribed but never administered to the patient, as his pain score remained below 7 on the VAS scale.
Carbapenem-associated neurotoxicity has been reported, particularly seizures linked to the use of imipenem. 19 In this case, the patient had been prescribed another carbapenem—meropenem—which is less frequently associated with neurotoxic effects. According to clinical practice guidelines, the dosing regimen administered was appropriate for the patient’s clinical condition. 6
A relationship was identified between the patient’s septic shock, underlying comorbidities, and the mixed anticholinergic-like syndrome associated with vancomycin. Acute or chronic systemic inflammatory states can significantly alter the permeability of the BBB. Continuous exposure to pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6 induces endothelial dysfunction and reduces the expression of tight-junction proteins in glial structural cells. 20 The most plausible mechanism by which vancomycin may induce neurotoxicity appears to be a dose-dependent adverse drug reaction that manifests in patients receiving supratherapeutic dosing and/or rapid infusion rates that raise plasma concentrations far above the therapeutic window. Individuals with a history of systemic inflammatory diseases, such as CKD, are at particularly high risk, as increased inflammation may promote BBB permeability, facilitating the passage of this glycopeptide into the central nervous system, where it can interfere with cholinergic activity.
Regarding the interaction between vancomycin and the receptor system, the effect appears to result from an indirect or noncompetitive mechanism leading to a mixed anticholinergic-like syndrome, as the ligand acetylcholine differs markedly from vancomycin in molecular weight and polarity. 2 Further research is needed to elucidate the mechanistic pathway and to clarify the association between these contributing factors. Although rare, such events highlight the continued relevance of case reports as valuable sources of clinical insight.
This case underscores the importance of pharmacist involvement in the pharmacotherapeutic management of hospitalized patients at high risk of overdosing, particularly those with CKD. 3 Ensuring safe medication use and identifying risks before they evolve into ADRs is essential. Institutional limitations prevented cerebrospinal fluid sampling unless medically indicated for suspected infection; therefore, pharmacokinetic simulations of plasma concentrations were performed by the Pharmacy Department’s research group. Given that the institution’s clinical pharmacy service is still under development, this case was evaluated retrospectively, after the adverse event occurred. This case report was submitted to the Ethics Committee of the “Dr. Ignacio Morones Prieto” High-Specialty Regional Hospital (IRB: CONBIOETICA-24-CEI-001-20160427).
In conclusion, vancomycin-induced neurotoxicity may occur in overdosed patients with underlying systemic inflammatory diseases such as CKD and can mimic a mixed anticholinergic-like syndrome. Infusion rate is as critical as dose. The Naranjo algorithm score was 10, indicating a definitive ADR associated with vancomycin use, consistent with a mixed anticholinergic-type syndrome not previously reported.
Supplemental Material
sj-docx-1-pmt-10.1177_87551225261417925 – Supplemental material for Vancomycin Overdose and Infusion Rate Error Leading to a Mixed Anticholinergic-Type Syndrome in a Hemodialysis Patient: A Case Report
Supplemental material, sj-docx-1-pmt-10.1177_87551225261417925 for Vancomycin Overdose and Infusion Rate Error Leading to a Mixed Anticholinergic-Type Syndrome in a Hemodialysis Patient: A Case Report by Waldo-Rodríguez Itzayana Guadalupe, Arriaga-García Francisco Javier, Romano-Moreno Silvia, Medellín-Garibay Susanna Edith, Martínez-Núñez Juan Manuel, Castro-Pastrana Lucila Isabel and Milán-Segovia Rosa del Carmen in Journal of Pharmacy Technology
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This case report was submitted to the Research Ethics Committee of the Hospital Regional de Alta Especialidad “Dr. Ignacio Morones Prieto” (IRB: CONBIOETICA-24-CEI-001-20160427) for publication.
Prior Poster or Abstract Presentation Information
This case has not been previously presented in any form.