
Abstract
Introduction
Multidrug-resistant (MDR), defined as organisms resistant to at least 1 antibiotic from 3 different antibiotic classes, and difficult-to-treat (DTR) organisms, defined as organisms that show nonsusceptibility to all first-line antimicrobial agents, represent an escalating public health crisis, leading to significant morbidity and mortality.1,2 Management and outcomes for these infections are often hampered due to resistance to empiric agents and logistical constraints associated with expanded susceptibility testing. 3 This problem is exacerbated when MDR or DTR organisms present as part of complex polymicrobial infections as commonly seen in deep-seated intra-abdominal infections (IAIs) or osteoarticular infections. Given the complexity and deep-seated nature of these infections, they often require multiple antimicrobials for prolonged durations, necessitating outpatient parenteral antimicrobial therapy (OPAT) and/or requiring agents with suboptimal risks of adverse drug events (ADEs). 4 As such, there is a growing need for antimicrobial regimens that offer simplified dosing, improved safety, and efficacy against resistant pathogens to facilitate antimicrobial stewardship and improve patient adherence.
Eravacycline is a fully synthetic fluorocycline approved for use in complicated IAIs.5 -8 Beyond labeled indications, real-world studies have demonstrated efficacy in other, non-urinary sites as well.9 -11 Eravacycline exhibits broad in vitro activity against Gram-positive cocci (including methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus [VRE]), anaerobes, and MDR Gram-negative rods (GNRs). Furthermore, it is attractive as an antimicrobial stewardship consolidation option for complex polymicrobial infections due to activity against carbapenem-resistant Enterobacterales (CREs), carbapenem-resistant Acinetobacter baumannii (CRAB), and other non-lactose fermenting GNRs such as Stenotrophomonas maltophilia. Pharmacokinetically, eravacycline has a favorable profile with an elimination half-life of roughly 20 hours, allowing for daily infusions in the outpatient setting.8,9,12,13 Despite these attributes, the clinical role of eravacycline remains a subject of debate due to its high volume of distribution (321L).
Current guidelines and guidance recommendations reflect a lack of clinical evidence rather than definitive evidence of eravacycline failure. While patients with these infections have not been excluded from previous trials, MDR pathogens have not constituted a large majority of these cohorts. Given the clinical, stewardship, and practical advantages offered by expanded eravacycline use in this patient population, additional real-world data are required to validate its efficacy. The objective of this study was to evaluate the efficacy and safety of eravacycline for the treatment of infections caused by culture-confirmed MDR or DTR organisms.
Methodology
Study Cohort and Setting
This was a retrospective, observational study at a large academic medical center of adult patients treated with eravacycline between January 1, 2017, and November 1, 2024. Data were collected and analyzed by infectious diseases (ID) trained pharmacists. The study was reviewed and approved by the local Institutional Review Board (IRB) and granted exemption with a waiver of informed consent due to its minimal risk to participants and retrospective nature.
Patients
Patients were included if they were ≥18 years of age and received eravacycline for at least 72 hours for the treatment of a culture-confirmed infection caused by an MDR (defined as resistance to at least 3 classes of antimicrobials) or DTR (defined as CRAB, VRE, or trimethoprim/sulfamethoxazole-resistant S. maltophilia) organism. Exclusion criteria included infection caused by non-MDR or DTR organisms, mortality within 72 hours of eravacycline initiation, or receipt of less than 72 hours of eravacycline treatment.
Outcomes
The primary endpoint of this study was 30-day all-cause mortality. Secondary outcomes included 60-day microbiological relapse, defined as re-growth of the same organism, and 30-day all-cause readmission from the end of eravacycline therapy, microbiological eradication, and adverse drug effects (ADEs). The ADEs in this study were limited to suspected antibiotic-associated diarrhea, and elevations in liver function tests (LFTs) were defined as an increase to 2 times the baseline value at any point during therapy.
Statistical Analysis
Descriptive statistics were utilized for all variables. Continuous variables were reported as means with standard deviation (SD) or medians with interquartile ranges (IQR) based on data distribution. Categorical data were reported as frequencies and percentages.
Results
Demographics
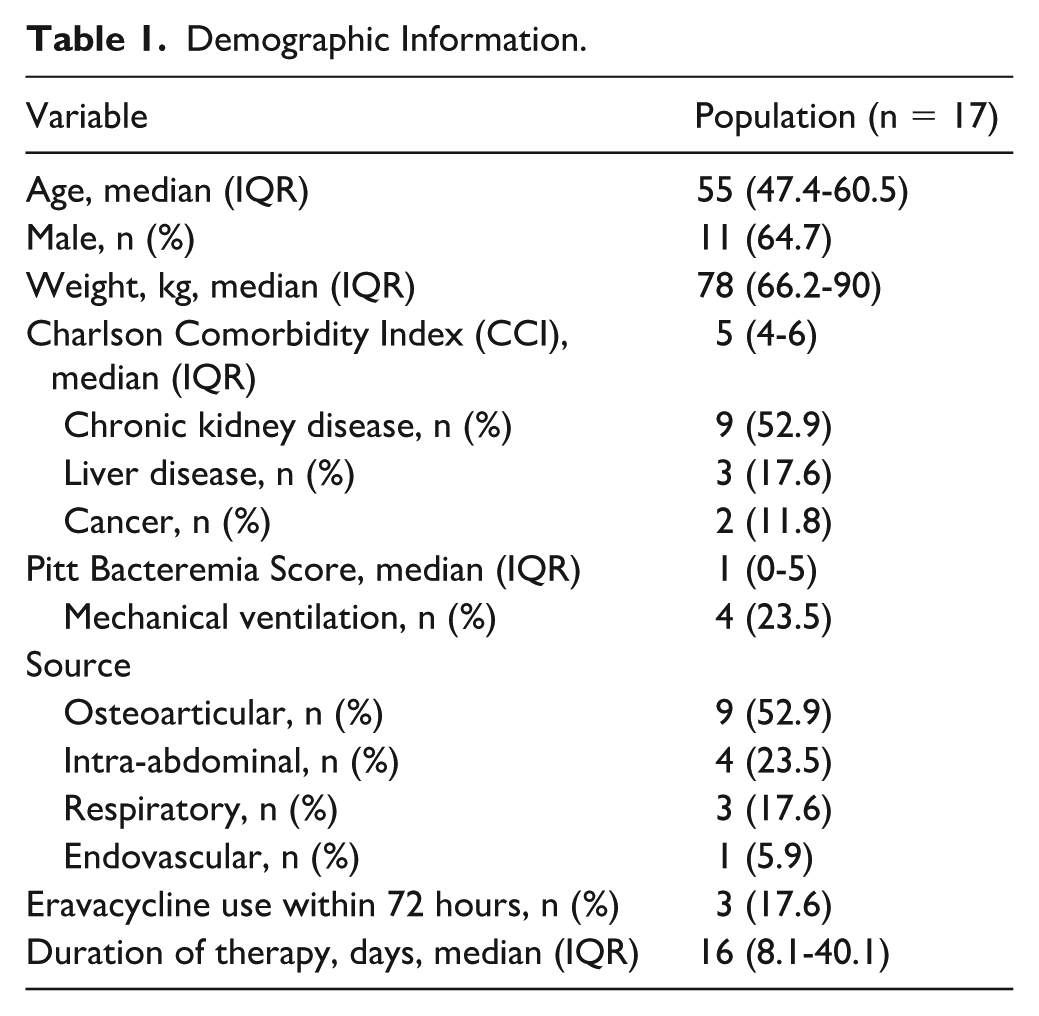
A total of 19 patients were screened, and 17 met the inclusion criteria for final analysis. The cohort had a high burden of comorbid conditions, with a median age of 55 years and a median Charlson Comorbidity index (CCI) of 5 (IQR = 4-6). Baseline severity of illness was variable, with a median Pitt Bacteremia Score of 1 (IQR = 0-5). Source of infection was determined by site of microbiologic testing and subsequent growth of organism(s) leading to eravacycline therapy. The most common sources of infection were osteoarticular (52.9%), followed by IAI (23.5%) and respiratory (17.6%) (Table 1).
Demographic Information.
Microbiology
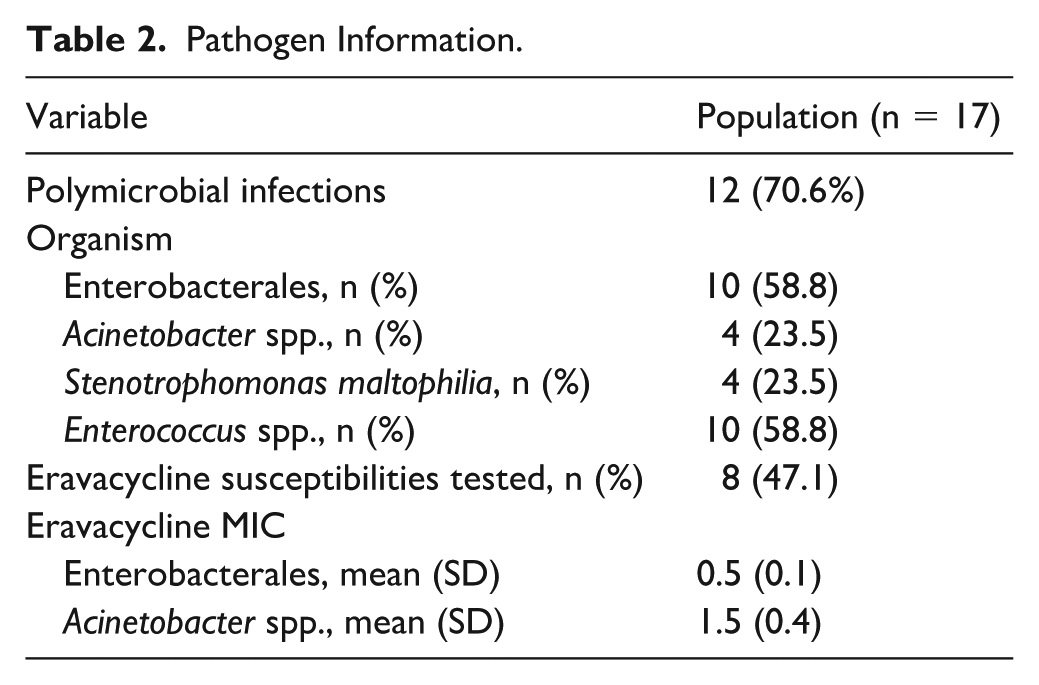
Most infections were polymicrobial (70.6%) and nosocomial (52.9%), defined as index culture collection >48 hours after admission (Tables 1 and 2). The most frequently isolated pathogens were VRE and Enterobacterales spp. (58.9% each), followed by Acinetobacter baumanii and S. maltophilia (23.5% each). Among the CRE organisms, 2 had confirmed carbapenemase enzymatic resistance patterns, including Klebsiella pneumoniae carbapenemase (KPC) or a New Delhi metallo-beta-lactamase (NDM) identified. Two patients had organisms with extended-spectrum beta-lactamase (ESBL), CTX-M genes detected via polymerase chain reaction (PCR) testing without corresponding carbapenemases. No enzymatic resistance was detected in the other CRE organisms. Eravacycline susceptibilities were available in 47% of isolates, with a mean minimum inhibitory concentration (MIC) of 0.5 ± 0.25 µg/mL. Notably, all tested CRE isolates showed MICs below the Food and Drug Administration (FDA)-approved susceptibility breakpoint of ≤0.5 µg/mL. 14 While there are no established susceptibility breakpoints for A. baumanii or S. maltophilia, the MIC90 ranges in existing literature have been described at 0.5 to 2 µg/mL and 1 to 4 µg/mL, respectively.15,16 Three of the isolates tested for eravacycline susceptibility in this review were CRAB. Two of the isolates had an MIC of 0.25 µg/mL, and 1 was 1 µg/mL (Table 2). Of note, none of the S. maltophilia isolates had MICs available.
Pathogen Information.
Treatment and Source Control
All patients included received a median weight-based dose of eravacycline of 1 mg/kg every 12 hours. There were no notable drug-drug interactions among patients receiving eravacycline. The median duration of therapy was 16 days (IQR = 8.1-40.1). Of note, there was a significant delay between initiation of eravacycline and index culture collection, with a median time to start of 6 days (IQR = 3.4-9.3) (Table 1). Definitive source control was only achieved in 4 (23.5%) patients. This may have been driven largely by inoperable infections, desire for medical management, or inability to achieve source control despite surgical intervention.
Outcomes
The primary outcome of 30-day all-cause mortality occurred in 3 patients (17.6%). Among patients eligible for 60-day relapse, who demonstrated culture clearance and no 30-day mortality, 1 patient (7.7%) had infection relapse. Similarly, only 2 patients (18.2%) were re-admitted within 30 days of the end of eravacycline treatment (Table 3).
Outcomes.
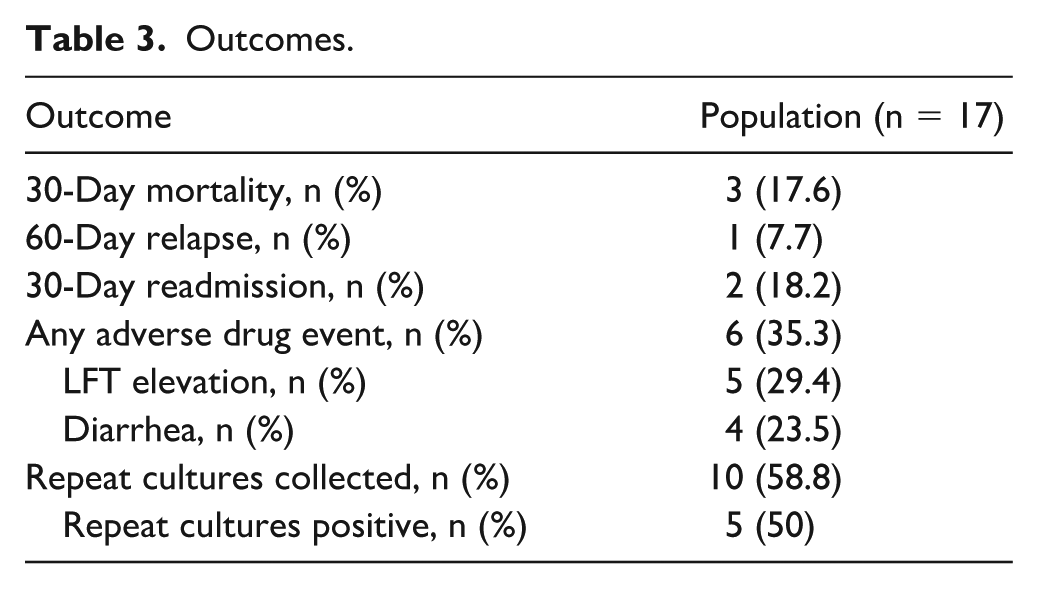
Of the 10 patients with repeat cultures collected, 5 (50%) demonstrated microbiological eradication. Adequate surgical source control was achieved in only 4 (23.5%) patients. Notably, none of the patients in whom the pathogen was not eradicated achieved adequate source control.
Adverse drug events occurred in 6 patients (35.3%). These events comprised of elevations in LFT (29.4%) and diarrhea (23.5%). No patients discontinued therapy due to ADEs (Table 3).
Discussion
This study represents one of few focused evaluations of eravacycline specifically targeting infections caused by confirmed MDR or DTR organisms. Where clinicians are often forced to rely on drug combinations with significant adverse effects as “best available therapy,” our findings offer insights into eravacycline performance in complex and DTR patient populations.
The high volume of distribution has led to some questions on the clinical utility of eravacycline for infections such as bloodstream infections (BSIs), despite real-world data demonstrating clinical effectiveness including a pooled analysis of bacteremic patients from the IGNITE 1 and IGNITE 4 trials. 17 The 2024 Infectious Diseases Society of America (IDSA) Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections recommends eravacycline for infections aside from bloodstream or urinary tract infections caused by CRE only when β-lactams are not available or unable to be tolerated due to lack of clinical evidence. 18 However, the guidance is even more reserved in the setting of CRAB and S. maltophilia, where IDSA recommends minocycline or tigecycline over eravacycline, citing limited clinical evidence of 1 retrospective analysis of CRAB pneumonia showing longer durations of mechanical ventilation and higher 30-day mortality compared to alternative regimens. 19 However, these data may be confounded by baseline differences in bacteremia incidence, and multiple other retrospective analyses have found favorable outcomes associated with eravacycline use in patients with CRAB.10,11,20 -22 Similarly, the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines currently do not recommend eravacycline for CRE or CRAB, citing the lack of clinical data supporting its use, despite its enhanced in vitro activity.23 -25
The primary finding of a 17.6% 30-day mortality rate, while higher than some existing literature, may still support eravacycline use due to the study cohort’s high-risk of death at baseline, up to 32% based on median CCI. 26
Furthermore, the present study offers several important insights into the clinical utility of eravacycline in a large academic medical center. First, this cohort had a higher percentage of isolates with eravacycline MIC results, especially for Gram-negative organisms. At the study institution, eravacycline is not part of the routine antimicrobial susceptibility report and is only run by request from the ID service. This delay in susceptibility testing, combined with the salvage nature of eravacycline therapy in this patient population, is likely to explain the delay in therapy for patients included in the study and may signal a predisposition to poor outcomes. Due to the potent in vitro activity of eravacyline against Enterococcus spp., susceptibilities were not routinely tested likely explaining the low rate of MIC availability. Like other available surveillance data, we found high rates of in vitro activity of eravacycline for CRE and CRAB. Another strength of this study was the inclusion of only infections caused by MDR or DTR organisms, a plurality of which were polymicrobial in nature. The safety and efficacy of eravacycline have previously been evaluated in the real-world setting in which MDR or DTR organisms comprised only a small percentage of infections. A study by Patino et al 27 evaluated clinical outcomes of eravacycline for infections caused by MDR pathogens, but to our knowledge, this is the first evaluation of eravacycline combining MIC data and clinical outcomes in infections caused by MDR or DTR organisms.
Interestingly, the most frequently encountered infectious source was osteoarticular which has been underrepresented in past clinical trials and real-world data.5,6,10 This was followed by IAI which is the FDA-labeled indication for eravacycline. While tetracycline derivatives have historically shown good bone penetration and variable joint concentrations, there is limited information on newer generation fluorocyclines. 28 The relatively low rate of infection relapses (7.7%), particularly given that definitive source control was achieved in a minority (23.5%) of patients, our data add support to eravacycline use in osteoarticular infections.
However, the results may necessitate a nuanced view given the cohort complexity and predominance of polymicrobial infections. While eravacycline acted as the backbone for MDR and DTR organisms, the contribution of concomitant antimicrobials cannot be fully excluded. Furthermore, there was a median delay of 6 days from index culture to initiation of eravacycline and low rates of definitive source control. The observed mortality rate likely reflects these factors, rather than a failure of the molecule itself. This aligns with the data presented by Kunz Coyne et al, 29 who demonstrated delayed initiation as an independent predictor of poor outcomes in immunocompromised hosts.
Like other real-world analyses of eravacycline utilization, the observed ADE rate was low and was dominated by diarrhea and LFT elevations, both of which are often observed in hospitalized patients and are multifactorial in nature (Table 3).
There are several limitations to this study which limit generalizability and ability to draw robust conclusions, primarily stemming from the small sample size, non-comparative design, and retrospective nature. As such, there was a heavy reliance on documentation in the medical record which may not have comprehensively described treatment rationale and introduced confounders to various outcomes. Similarly, the single-center retrospective design limited comprehensive follow-up, as readmissions or regimen changes managed at outside medical institutions could not be captured. Additional limitations of low rates of source control and significant delays in initiating eravacycline therapy may have impacted outcomes beyond efficacy of the antibiotic. Given the significant delay in eravacycline initiation, we were unable to capture or quantify the impact of preceding antimicrobial therapy or patient clinical trajectory. Likewise, the delay in initiation of eravacycline therapy may have been due to its use in a salvage nature. As such, patients in this cohort may have been predisposed to poor outcomes such as mortality, relapse, and multifactorial ADEs such as transaminitis and diarrhea due to delays in therapy. Another important limitation was the lack of consistent eravacycline susceptibility testing, which may reflect real-world practice gaps and be a cause for treatment delay, resulting in uncertainty between in vitro activity and clinical outcomes. Finally, the heterogenic nature of infectious sources and variable rates of source control may confound the results. Furthermore, the exclusion of patients who met a mortality outcome within 72 hours of initiation of eravacycline introduces both immortal time and selection bias, possibly precluding a direct causal assessment of drug efficacy. Future research is needed to evaluate outcomes in complex infections as an initial therapeutic option.
Conclusions
In the present study of complex patients with MDR and DTR infections, eravacycline demonstrated a safety profile consistent with previous literature and achieved clinical stability in most patients despite significant delays in therapy initiation and limited source control. This preliminary, observational data may signal a potential role for eravacycline in the management of complex osteoarticular infections caused by resistant pathogens, indicating the need for further investigation through prospective studies. In addition, while the data support robust in vitro activity, more frequent utilization of susceptibility testing in patients with CRE, CRAB, and S. maltophilia may reduce the time to appropriate therapy and further improve outcomes.
Footnotes
Acknowledgements
None.
Ethical Considerations
This study was reviewed and determined to be exempt by the Augusta University Institutional Review Board (2261393-1).
Consent to Participate
The requirement for informed consent to participate has been waived by the Institutional Review Board.
Consent for Publication
Not applicable.
Author Contributions
DTA and JE contributed to conceptualization, methodology, and writing – review & editing. DTA contributed to data curation, formal analysis, investigation, project administration, resources, supervision, validation, visualization, and writing – original draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
Data may be made available upon reasonable request to the corresponding author.