
Abstract
Background:
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) report recommends initial bronchodilator therapy over inhaled corticosteroids (ICS) for most patients. However, real-world prescribing often diverges. Management is further complicated in hospitalized patients with suspected but unconfirmed chronic obstructive pulmonary disease (COPD), where providers must decide on therapy initiation and outpatient follow-up.
Objective:
To describe inhaler prescribing in suspected but unconfirmed COPD upon hospital discharge.
Methods:
This was an institutional review board–approved retrospective cohort study of patients of ages 40 years or older with a smoking history of at least 10-pack years, but without a prior COPD diagnosis, who presented with a suspected COPD exacerbation or acute respiratory failure secondary to suspected COPD. The primary outcome was inhaler prescribing at discharge. Secondary outcomes included confirmed COPD diagnosis, guideline concordance, hospital readmission for a COPD exacerbation, and ICS-related adverse events within 180 days.
Results:
Of the 51 patients included in the study, 29 (56.9%) were prescribed new inhalers, with 15 (29.4%) prescribed ICS-containing regimens. Following discharge, 15 patients (29.4%) completed pulmonary function testing, with 8 (15.7%) receiving a COPD diagnosis. Guideline concordance could not be assessed due to absent documentation. Eight patients (15.7%) were readmitted with a COPD exacerbation, and 13 ICS-related adverse events were documented. Limitations include the sample size and retrospective study design.
Conclusion:
This study found a high frequency of initial ICS prescribing for suspected but unconfirmed COPD, as well as limited follow-up and diagnostic reassessment. These findings highlight the need for system-level interventions to optimize discharge prescribing and ensure timely follow-up.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a persistent and progressive respiratory condition with significant health and financial consequences that are anticipated to increase over time. In 2019, COPD ranked as the third leading cause of death worldwide, 1 and by 2060, an estimated 5.4 million deaths globally could be attributed to the disease state and associated comorbidities. 2 In the United States, specifically, COPD is the sixth leading cause of death, responsible for over 150,000 deaths annually, and imposes a significant economic burden with projected direct costs exceeding $40 billion per year over the next 2 decades.3,4
Through 2022, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) report categorized newly diagnosed patients into groups A, B, C, or D based on symptom burden and exacerbation history to guide initial therapy selection. 3 Patients with no more than 1 moderate exacerbation and no hospitalizations, classified by the 2022 GOLD report as groups A and B, are recommended to receive bronchodilator monotherapy, consisting of a short-acting beta-2 agonist (SABA), a short-acting muscarinic antagonist (SAMA), or a long-acting bronchodilator, such as a long-acting beta-2 agonist (LABA) or long-acting muscarinic antagonist (LAMA), depending on symptom severity and response. Patients with at least 2 moderate exacerbations or at least 1 exacerbation leading to hospitalization are classified by the 2022 GOLD report into groups C or D based on presence of lower or higher symptom burden, respectively. For group C, LAMA monotherapy is recommended as the initial therapy. For group D, LAMA monotherapy, LABA-LAMA combination therapy for highly symptomatic patients, or LABA-inhaled corticosteroid (ICS) combination therapy for patients with blood eosinophils of at least 300 cells/microliter or concomitant asthma is recommended. Escalation to triple therapy (LABA-LAMA-ICS) is reserved for patients with persistent exacerbations despite dual bronchodilator or LABA-ICS therapy. 3 While the ABCD assessment tool was revised to the ABE assessment tool in 2023, the recommended treatment approach remains similar, with an emphasis on initial therapy with bronchodilators and the addition of ICS only for select patients. 2 However, dual bronchodilator therapy is now recommended instead of bronchodilator monotherapy, and LABA-ICS combination therapy is no longer recommended. Rather, patients requiring an ICS should receive triple therapy with LABA-LAMA-ICS. 2
Prior studies have emphasized initiating COPD treatment with bronchodilator therapy for a majority of patients. One landmark trial of patients with moderate to severe COPD and history of at least 1 prior exacerbation compared LABA-LAMA to LABA-ICS combination therapy. 5 The study found that dual bronchodilator therapy significantly reduced the annual rate of all exacerbations, as well as increased the time to first exacerbation. Similar results were observed when limiting the analysis to moderate or severe exacerbations. 5 Recent literature has reinforced this concept, as well as elucidated the role of ICS-containing regimens in patients with more severe disease and elevated blood eosinophils. Two landmark trials of patients with moderate to very severe COPD and history of at least 1 moderate to severe exacerbation compared triple therapy to dual therapy with either LABA-LAMA or LABA-ICS.6,7 Comparatively speaking, these two trials included a greater proportion of patients with very severe COPD and higher baseline eosinophil counts. The annual rate of moderate or severe exacerbations and time to first moderate or severe exacerbation was significantly reduced with triple therapy compared to both dual therapy groups. These results were maintained across all baseline eosinophil levels, although the authors noted that patients with an eosinophil count of 150 cells/microliter or greater experienced larger reductions in the study endpoints.6,7
Despite the currently available literature, previous studies have demonstrated persistent discordance between the GOLD report recommendations and real-world prescribing, including overtreatment of low-risk patients, premature initiation of triple therapy, and widespread overuse of ICS, including many patients receiving ICS as first-line treatment, all of which highlight opportunities for provider education and system-level interventions.1,8-12 Furthermore, with the known adverse effects of ICS, including increased risk of pneumonia and oral candidiasis, judicious use of these agents is imperative to minimize unnecessary risks to patients. 13
The diagnosis and treatment of COPD is further complicated for patients admitted with a suspected COPD exacerbation despite no prior documented history or spirometry testing. As spirometry is not commonly performed in the inpatient setting, clinicians are left with the challenging decision on whether to initiate maintenance COPD treatment, including which regimen to select, as well as coordinating outpatient follow-up for diagnostic testing to minimize disruptions in patient care. To our knowledge, no literature has evaluated treatment of this unique subset of patients; therefore, the objective of this study was to describe current inhaler-prescribing patterns in patients with suspected but unconfirmed COPD upon hospital discharge.
Methods
This was a retrospective cohort study conducted within an academic health system, comprised of an academic medical center and 4 community hospitals, between January 1, 2019, and December 31, 2022. Eligible patients were of ages 40 years or older; had a documented smoking history of at least 10 pack-years; had no prior International Classification of Diseases (ICD)-10-coded diagnosis of COPD (J44.9), chronic bronchitis (J41.0, J41.1, J42), or emphysema (J43.1, J43.2, J43.9); and were admitted with an ICD-10-coded diagnosis of either a COPD exacerbation (J44.1) or acute respiratory failure (J96.0, J96.00, J96.01, J96.02, J96.03) with documented suspicion of COPD in the electronic medical record. Patient inclusion was confirmed through structured review of the electronic medical record. Notably, patients found to have acute respiratory failure due to an unrelated etiology, such as COVID-19 or hypervolemia, were not eligible for inclusion in the study. Exclusion criteria included pregnancy, prior diagnosis of asthma, discharge to hospice, and death during hospitalization. The primary outcome was inhaler prescribing trends in patients with suspected but unconfirmed COPD at hospital discharge. Secondary outcomes, evaluated within 180 days of hospital discharge, included the proportion of patients with a confirmed diagnosis of COPD, the proportion of patients with confirmed COPD discharged with guideline-concordant inhaler regimens based on the 2019 to 2022 GOLD reports, hospital readmission for an acute exacerbation of COPD, and ICS-related adverse events, defined as pneumonia and oral candidiasis.
Descriptive statistics were utilized to analyze results. An exploratory analysis using Spearman’s correlation was conducted to identify factors associated with prescribing of new inhaler therapy, including ICS-containing regimens (insurance status, site of discharge, pulmonology service consultation, and involvement of the COPD pathway). This study was approved by the institutional review board and met the criteria for waiver of consent.
Results
Fifty-three patients were eligible for inclusion in the study. With 2 patients meeting exclusion criteria (n = 1 discharge to hospice, n = 1 death during hospitalization), a total of 51 patients were included in the final data analysis. Baseline characteristics for the study population can be found in Table 1. Prior to the index hospitalization, 34 patients (66.7%) were not prescribed any type of inhaler therapy, 13 patients (25.5%) were prescribed a short-acting bronchodilator as needed only, and 4 patients (7.8%) were prescribed a maintenance inhaler. Of the 4 patients using a maintenance inhaler at baseline, 1 was prescribed a LABA-LAMA combination inhaler, and 3 were prescribed LABA-ICS combination inhalers.
Baseline Characteristics (n = 51).
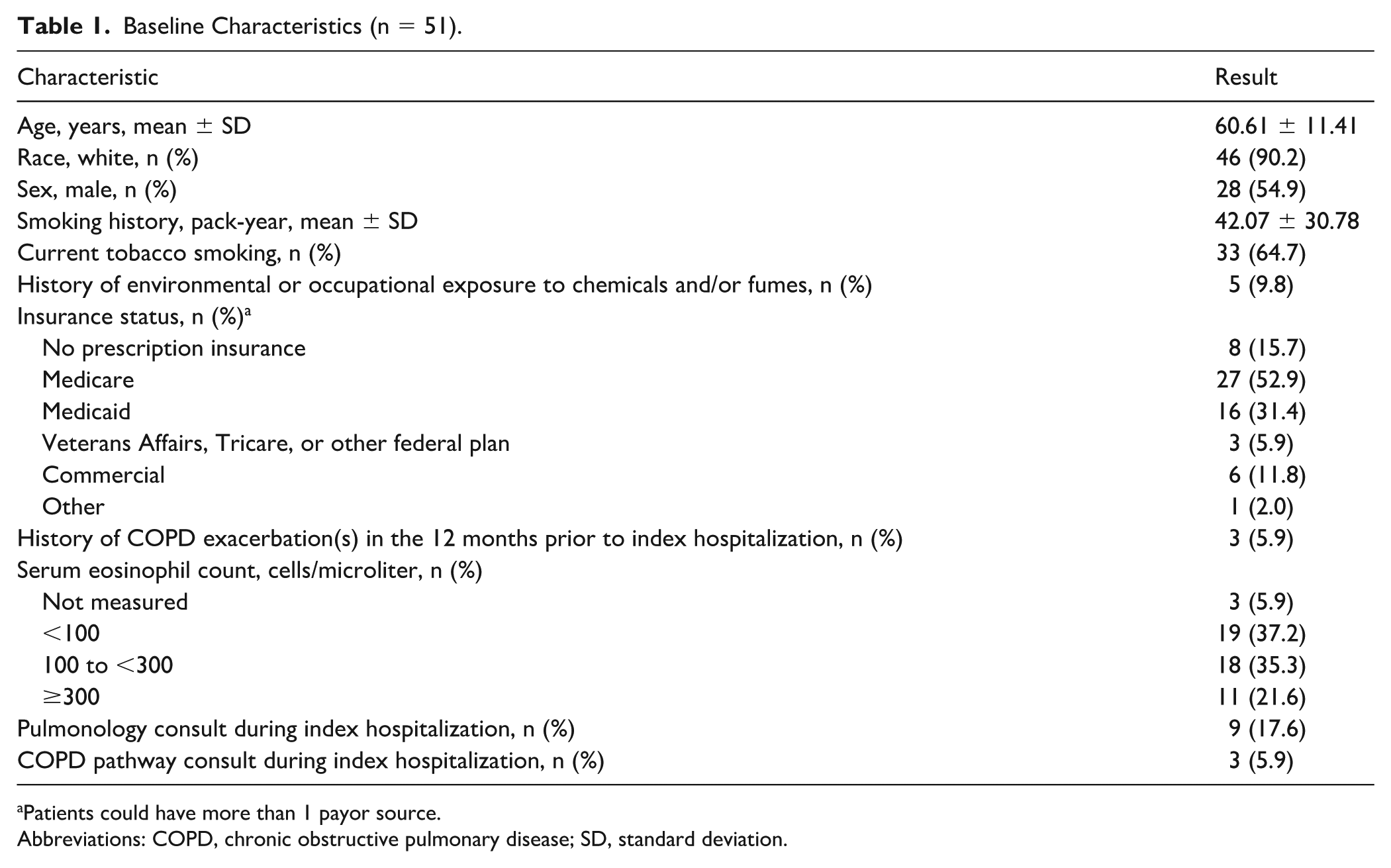
Patients could have more than 1 payor source.
Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation.
A summary of inhaler therapy on the discharge medication list, reflecting either newly prescribed therapy or therapy continued from home, as well as changes in inhaler therapy from admission to discharge, can be found in Table 2. Overall, 29 patients (56.9%) were prescribed new inhaler therapy on discharge, with 26 patients (51%) prescribed new maintenance inhaler therapy. Of the 29 patients prescribed new inhaler therapy on discharge, 15 patients (51.7%) were prescribed ICS-containing regimens. Blood eosinophil counts for patients receiving new ICS-containing regimens on discharge were 0 cells/microliter for 7 patients (46.7%), 100 cells/microliter for 4 patients (26.7%), and greater than 300 cells/microliter for 3 patients (20%). One patient (6.7%) receiving a new ICS-containing regimen on discharge did not have a blood eosinophil count obtained during the index hospitalization.
Inhaler Therapy on Discharge and Associated Changes From Baseline (n = 51).
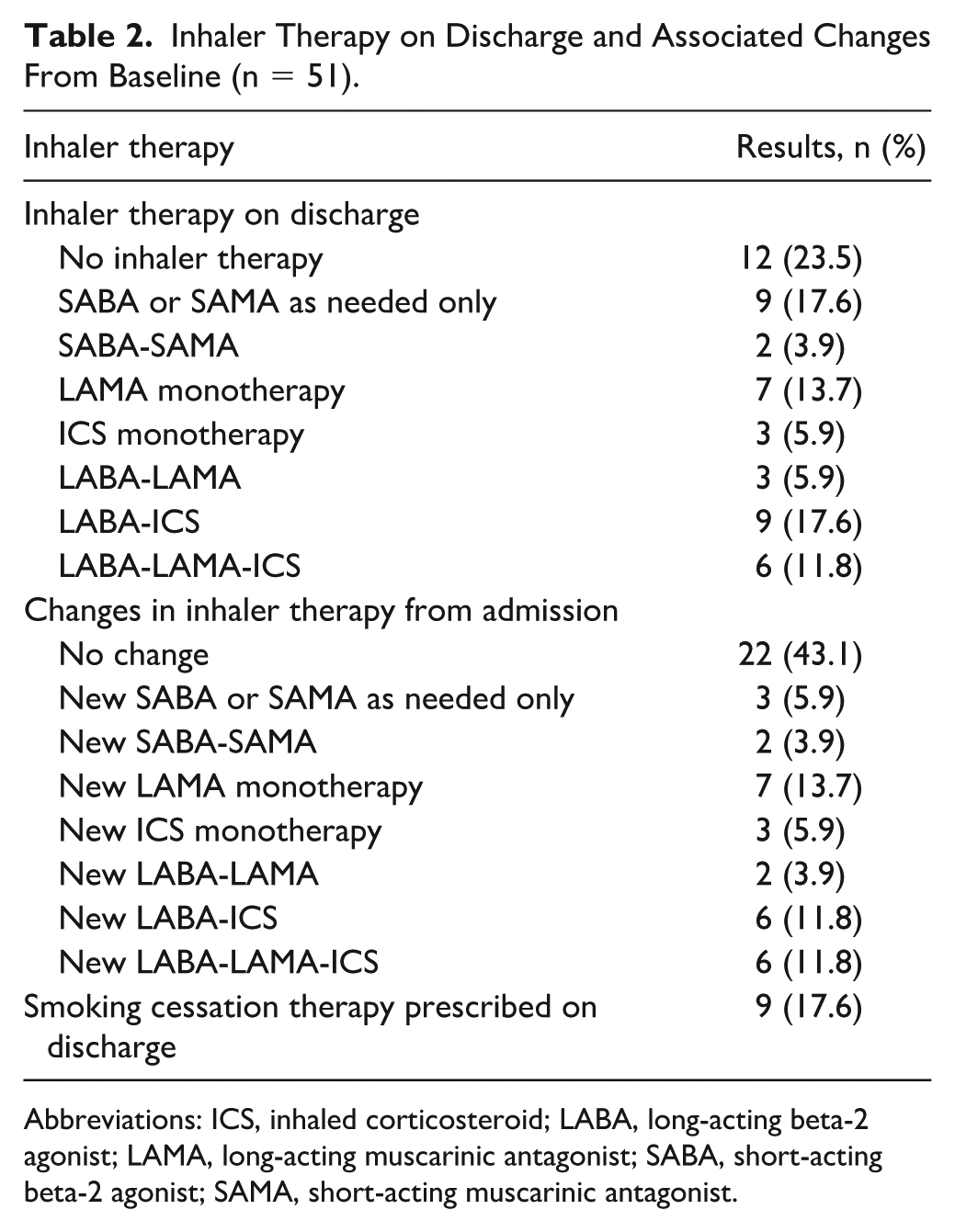
Abbreviations: ICS, inhaled corticosteroid; LABA, long-acting beta-2 agonist; LAMA, long-acting muscarinic antagonist; SABA, short-acting beta-2 agonist; SAMA, short-acting muscarinic antagonist.
Upon hospital discharge, 34 patients (66.7%) were either scheduled or received a referral for an outpatient follow-up appointment with a primary care provider or pulmonology specialist for a formal COPD assessment. Twenty-one patients (41.2%) completed a follow-up visit within 180 days of hospital discharge. Fifteen patients (29.4%) underwent pulmonary function testing (PFT), with 8 patients (15.7%) receiving a formal COPD diagnosis. The remaining 7 patients had PFT findings that were not consistent with a diagnosis of COPD.
Of the 8 patients receiving a formal diagnosis of COPD within 180 days of hospital discharge, the GOLD group was not specified in outpatient provider documentation; therefore, concordance of inhaler regimens prescribed on hospital discharge to the 2019 to 2022 GOLD report was unable to be assessed. Notably, 5 of these patients were prescribed LAMA monotherapy, 2 patients were prescribed the LABA-ICS combination therapy, and 1 patient was prescribed the LABA-LAMA-ICS combination therapy on hospital discharge. Of the aforementioned 15 patients prescribed new ICS-containing regimens on discharge, only 3 patients (20%) received a formal COPD diagnosis within 180 days of discharge.
Eight patients (15.7%) were readmitted with a COPD exacerbation within 180 days of hospital discharge, with 5 of these readmissions occurring within 30 days. Of the 8 patients readmitted, 2 received a formal COPD diagnosis following the index hospitalization. The remaining 6 patients either did not have follow-up planned upon hospital discharge or did not complete their planned outpatient follow-up visit. A total of 13 ICS-related adverse events across 11 patients were documented within 180 days of hospital discharge, with 9 reported cases of pneumonia and 4 reported cases of oral candidiasis.
Spearman’s correlation demonstrated no significant associations with assessed variables and prescribing of new maintenance inhaler therapy (n = 29) or new ICS-containing regimens (n = 15).
Discussion
To date, this is the first study to characterize prescribing trends in patients with suspected but unconfirmed COPD, where diagnostic uncertainty at the time of discharge poses challenges for optimal pharmacologic management. Over half of the study population were prescribed new inhaler therapy at discharge, with ICS-containing regimens representing the majority. A correlation analysis revealed no significant factors associated with prescribing new inhaler therapy, including ICS-containing regimens. Factors analyzed included insurance status, site of discharge, pulmonology service consultation, and involvement of the COPD pathway, a service led by a respiratory therapist with advanced training to provide individualized assessment, treatment recommendations, and coordination of outpatient follow-up. While none of these factors were significantly associated with prescribing patterns, prior literature has demonstrated the influence of financial restrictions due to the lack of insurance or insurance formularies,14,15 differences in institutional resources and support,15-18 and pulmonary specialist involvement17,19 on prescribing decisions. The absence of significant findings with the present study could be attributed to the limited sample size.
The overuse of ICS in COPD has been demonstrated in numerous studies despite guidelines recommending reserving its use for select patients. A retrospective analysis of nearly 1,500 patients diagnosed with COPD, groups A to D, for at least 1 year who were treated by pulmonary specialists demonstrated overall low concordance with guideline-recommended inhaler therapy in groups A, B, and C, as well as overuse of ICS across all groups. 8 Another retrospective, observational study using a clinical database of 318 primary care sites in the United Kingdom, comprising over 20,000 newly diagnosed patients, found that 45% were prescribed an initial ICS-containing regimen. 9 In a comparable study conducted within the Veterans Affairs system, 23.9% of patients with COPD were prescribed ICS-containing regimens without a documented indication, defined as asthma or history of frequent or severe exacerbations. 10 Notably, ICS were used in 29.5% of patients with spirometry-confirmed airflow obstruction and in 14.3% without, underscoring overuse even among those who may not meet diagnostic criteria for COPD. 10 In the present study, 29.4% of the entire study population, and 51.7% of the subset of patients prescribed new inhaler therapy, received new ICS-containing regimens upon hospital discharge. Notably, only 3 of these patients had documented eosinophilia of at least 300 cells/microliter, the threshold most associated with ICS benefit. 2 Furthermore, only 3 of these patients received a formal COPD diagnosis within 180 days of hospital discharge, raising concern for potential overuse or misuse of ICS.
It is important to note that judicious use of ICS-containing therapy in select patients with COPD is appropriate and supported by the literature. In addition to the reduction in moderate or severe exacerbations observed in the IMPACT and ETHOS clinical trials, triple therapy also demonstrated a significant reduction in all-cause mortality compared to LABA-LAMA combination therapy.6,7 While these benefits exist, it is imperative to recognize that the study populations in these trials differ substantially from the patients in the present study. In IMPACT, approximately 50% of patients had a history of at least 2 moderate exacerbations, and 25% had a history of at least 1 severe exacerbation within the previous year. In ETHOS, these findings were approximately 60% and 15%, respectively. In addition, approximately 60% of the study population in both trials had a serum eosinophil count of at least 150 cells/microliter.6,7 Combined, this reflects a population very distinct from the patients observed in the present study. Given the increased risk of adverse effects associated with ICS, including pneumonia and oral candidiasis, careful consideration should be given to ICS prescribing in less severe or unconfirmed COPD cases.1,2,13
This study also revealed a low rate of diagnostic follow-up for formal evaluation of COPD after hospital discharge. The 2022 GOLD report recommends outpatient follow-up within 4 weeks of hospital discharge to assess inhaler regimen and technique, symptom severity, and physical activity capacity. 3 It is recommended for these items to be reassessed and for spirometry testing to be performed within 3 to 4 months of hospital discharge. 3 In the present study, although two-thirds of patients were referred or scheduled for post-discharge evaluation, only 21 patients, less than half of the study population, completed an outpatient follow-up visit within 180 days of discharge. Furthermore, despite having an ICD-coded diagnosis of a COPD exacerbation or acute respiratory failure with documented suspicion of COPD, approximately only one-third of the study population completed spirometry testing. Of these 15 patients, 8 met diagnostic criteria for COPD, while 7 did not. Notably, 4 of the 7 patients without confirmed COPD were initiated on new maintenance inhaler therapy upon hospital discharge, with one initiated on triple therapy. The remaining 6 patients who completed an outpatient follow-up visit did not undergo spirometry testing within 180 days of discharge. As a result, patients may have remained on empiric therapy without diagnostic confirmation or opportunity for treatment optimization. This delay in diagnostic and therapeutic evaluation is not without consequences. One landmark study assessed the outcomes associated with prompt initiation of triple therapy following a COPD exacerbation, defined as within 30 days of the index event, and found that prompt initiation was associated with a decrease in subsequent exacerbations, as well as reductions in cost. 20 For each 30-day delay in therapy initiation, there was a 5% increase in the rate of subsequent exacerbations. 20 Collectively, the findings of this study highlight the importance of prompt follow-up and treatment optimization following COPD exacerbations.
In addition to loss of follow-up, none of the 8 patients who received a formal COPD diagnosis within 180 days of discharge had their GOLD group classification documented. This reflects a significant clinical documentation gap, as patients were often categorized by spirometric stage (GOLD 1-4) rather than GOLD group (A-D), despite GOLD group being more relevant for initial inhaler selection. Since symptom burden and exacerbation history, rather than FEV1 alone, drive treatment decisions and clinical outcomes, the absence of group classification precluded accurate evaluation of concordance with the 2019 to 2022 GOLD reports. Notably, 3 of these patients were prescribed ICS-containing regimens, with 2 patients prescribed LABA-ICS combination therapy, and 1 patient prescribed triple therapy. While a definitive assessment cannot be conducted due to the aforementioned omissions in outpatient documentation, it is reasonable to conclude that the two patients receiving LABA-ICS combination therapy did not meet criteria for ICS-containing regimens based on their blood eosinophil counts and exacerbation history. However, the remaining patient, with a blood eosinophil count of 500 cells/microliter and history of 3 exacerbations in the year prior to the index hospitalization, was a reasonable candidate for the triple therapy that was prescribed on discharge.
This study helps address a key gap in the literature but has limitations. First, the small sample size may limit the overall generalizability of the results, particularly with the low rates of outpatient follow-up for formal COPD evaluation. In addition, due to the retrospective nature of the study and documentation gaps, we were unable to objectively assess whether inhaler selection aligned with guideline recommendations. Lastly, the 2019 to 2022 COPD assessment tool was utilized in the study despite the release of more recent updates during the data-collection period. However, given the substantial lag in implementing evidence and clinical guidelines into practice 21 and the intent to follow up with patients for 6 months following their index hospitalization, the 2019 to 2022 COPD assessment tool was utilized to maintain consistency in interpretation of the results.
Conclusion
In conclusion, the findings of this study emphasize the need for interdisciplinary and system-level interventions to optimize discharge prescribing and outpatient follow-up in patients hospitalized with suspected but unconfirmed COPD. Opportunities within transitions of care, including implementation of a dedicated nurse or respiratory therapist navigator;22,23 utilization of a discharge checklist or care bundle;24,25 and coordination of outpatient referrals, follow-up, and pulmonary rehabilitation,24,26 could help to standardize care and ensure barriers are addressed surrounding hospital discharge. In addition, inpatient spirometry has been found to align with outpatient values. 27 Exploring opportunities for implementation of spirometry prior to discharge could serve as another tool to ensure timely diagnosis and subsequent treatment initiation. Lastly, provider education on the GOLD report is imperative to positively influence prescribing patterns and ensure appropriate use of ICS therapy. In parallel, education on appropriate de-prescribing of ICS in patients who have not, or are unlikely to, benefit is important to minimize medication exposure and avoid unnecessary adverse drug events. 13 Future studies should aim to enroll larger patient populations across multiple study sites to better characterize current prescribing trends and identify factors associated with prescribing new inhaler therapy, including ICS-containing regimens, in this understudied patient population.
Footnotes
Acknowledgements
The authors would like to acknowledge Danielle Harrison for assistance with data collection and J. Andrew Woods for reviewing an early draft of the introduction and methods sections of the manuscript. This research was previously presented in poster format at the American College of Clinical Pharmacy Annual Meeting in Dallas, Texas, in November 2023 and the American Society of Health-System Pharmacists Midyear Clinical Meeting in Anaheim, California, in December 2023.
Ethical Considerations
This study was approved by the Wake Forest University Institutional Review Board and met the criteria for waiver of consent (approval number: 00100089).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contribution
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available on request from the authors.