
Abstract
Background:
During hospital admission and discharge, investigational drugs administered due to participation in clinical trials are at risk for medication errors if not accurately documented.
Objective:
The primary objective of this study is to assess whether investigational drug service (IDS) pharmacy-led investigational medication reconciliation during outpatient investigational drug dispensing improves the rate and accuracy of investigational drug documentation in the electronic health record (EHR) medication list.
Methods:
This retrospective study was conducted at Rady Children’s Hospital Orange County and compared investigational drug dispensing encounters in the pre-IDS period (August 1, 2022-July 31, 2023) to the IDS period (November 1, 2023-October 31, 2024). Differences between periods were estimated using binomial generalized estimating equations to obtain absolute risk differences, with robust standard errors to account for multiple prescriptions within patients.
Results:
Of 174 dispensed prescriptions, the investigational drug was documented on the EHR medication list for 27 of 90 drugs in the pre-IDS period (30.0%) and 80 of 84 drugs in the IDS period (95.2%; P < .001). Complete and accurate documentation increased from 6.7% to 95.2% for formulation, 21.1% to 94.0% for dose, 28.9% to 95.2% for route, 27.8% to 94% for frequency, and 7.8% to 95.2% for investigational drug alert (all P < .001).
Conclusions:
Baseline documentation of investigational drugs on the EHR medication list was low. Investigational drug service pharmacy-led documentation was associated with significant improvement in documentation rate and accuracy.
Keywords
Introduction
Several studies have demonstrated the importance of medication reconciliation during transitions of care.1-4 Suboptimal communication at the time of hospital admission and discharge may result in discrepancies in the patient’s medication list. 1 Inaccurate medication lists may lead to prescribing and administration of incorrect dose, route, or frequency; duplication of therapy; drug interactions; adverse drug reactions; or omission of therapy.2,3 Analysis of medication histories documented for pediatric patients found 13% to 19% of medication histories had at least one medication discrepancy.3,4 According to Heath et al, 4 up to 60% of the medication discrepancies for pediatric patients occur with oral liquid formulations. Oral liquid formulations may be compounded with multiple concentrations which may cause confusion related to volume and dose. 4
Medication reconciliation conducted by pharmacists and pharmacy technicians can significantly reduce medication discrepancies up to 66%. 1 Pharmacy directed medication reconciliation in pediatric patients can correct missing medications, missing information, and incorrect doses, and has been found to affect patient care during admission for 22% of patients, requiring change to the patient’s care plan or immediate change to a medication order. 5
In clinical research, medications received by study participants are often provided by a research sponsor.6,7 The medications may not be approved by the Food and Drug Administration (FDA), or they may be FDA-approved drugs that are commercially available. 8 Regardless, the medications provided by research sponsors for execution of clinical trials are considered investigational supply and are designated for use in specific clinical trials.6-8 Accountability records must clearly document the receipt, dispensing, and final disposition for investigational supply of medication.6-8 It is important for prescribers to clearly indicate in medication orders and prescriptions when drugs are prescribed as part of a research protocol and investigational drug supply must be used, especially if the drug is also available commercially. 8
When patients are admitted to or discharged from the hospital, investigational drugs administered due to participation in clinical trials are at risk for medication errors if not accurately documented. 9 Redic et al 9 reviewed medication profiles after completion of study visits with investigational drug dispensing and found only 20.6% of investigational drugs were included on the medication list. Of those investigational drugs documented on the medication list, only 40% had correct dose and 50% had correct frequency documented. 9
Some investigational drugs were missing from the medication list at Rady Children’s Hospital Orange County or were not clearly documented in the electronic health record (EHR) as investigational drug supply for use in a clinical trial, despite a historical standard using the “INV-” prefix as an investigational drug alert on medication profiles. Therefore, in September 2023, a pharmacy-led process was implemented in which a new task was assigned to the investigational drug service (IDS) pharmacists to document the investigational drugs directly in the patient’s EHR medication list.
Previous studies have demonstrated that pharmacy directed medication reconciliation can reduce medication discrepancies for commercially available drugs. 1 Studies have also demonstrated that investigational drugs are frequently omitted from the medication list. 9 The primary objective of this study was to evaluate the impact of implementing IDS pharmacy-led investigational medication reconciliation at the time of outpatient investigational drug dispensing on rate and accuracy of investigational drug documentation in the EHR medication list, comparing the pre-IDS and IDS implementation periods.
Method
This was a single-center, retrospective study conducted at a 386-bed pediatric hospital, Rady Children’s Hospital Orange County. The study was approved by the institutional review board. Patients were eligible for inclusion in the study if they received an investigational drug dispensed by the IDS due to participation in a clinical trial or a single patient investigational new drug (IND) treatment plan during a hospital or clinic visit. Investigational drug dispensing was excluded if the drug was only administered at the hospital and was not intended for the patient to continue administration at home (eg, intravenous infusion which is received during admission to the hospital or outpatient infusion center). Qualifying dispenses included either of the following: (1) a new investigational drug that was not previously dispensed to the patient or (2) a change in formulation, dose, route, or frequency for an investigational drug. The process for IDS pharmacists to document investigational drugs on the EHR medication list was implemented in September 2023. Investigational drug dispensing that occurred during August 1, 2022 through July 31, 2023 was included in the standard documentation period (pre-IDS period), and dispensing that occurred during November 1, 2023 through October 31, 2024 was included in the IDS documentation period (IDS period). The IDS pharmacists were asked to document investigational drugs directly in the patient’s EHR medication list. To clearly identify the drug as investigational drug supply provided for a clinical trial, an “INV-” prefix was added to the drug name to serve as an investigational drug alert. The comment “Investigational Drug, Research Protocol [protocol ID]” was included in the comments, and the formulation, dose, route, and frequency were documented. When applicable, the drug name or dose was entered in a blinded manner (eg, “drug or placebo”). These details were documented on the EHR medication list by the IDS pharmacists at the time of outpatient investigational drug dispensing for clinical trials or compassionate use. The documentation was updated if the dose changed on subsequent dispense. Any provider, including pharmacists, physicians, and nurse practitioners, could remove the investigational drug from the medication list if the patient reported the medication was no longer active during medication reconciliation.
The accuracy of documentation was evaluated by determining if formulation and strength, dose, route, frequency, and investigational drug alert were documented completely and correctly. Documentation was considered incomplete or incorrect if partially documented but missing details (eg, missing oral liquid concentration or tablet strength) or if incorrectly documented (eg, incorrect dose or frequency).
Investigational drug service dispensing records in Vestigo, the IDS system, and medical records in Cerner, the EHR system, were reviewed for the study periods described above. Information collected included patient gender, age, and ethnicity. Prescription details collected included prescription number, drug name, formulation, dose, route, and frequency. Details documented on the medication list in the EHR were collected including protocol, drug name, formulation, dose, route, frequency, alert of investigational drug status, role of user performing documentation, and date of documentation.
The primary outcome was the overall rate of documentation of investigational drugs on the patient’s medication list in the EHR prior to next study visit or prior to discontinuation of treatment and was assessed during the pre-IDS period in comparison with the IDS period. For documented medications, accuracy was evaluated by comparing the rate of correct and complete documentation for drug details (eg, formulation, dose, route, frequency, and investigational drug alert (eg, INV- prefix)) between periods. The secondary outcome was the role of individuals documenting investigational drugs on the medication list. For the IDS period, the frequency that documentation of investigational medications was modified by the IDS pharmacists to correct drug name, formulation, dose, route, frequency, or investigational drug alert was determined.
Statistical Analyses
Commercial availability (yes/no) and formulation type were summarized separately for the pre-IDS and IDS periods. Distributions were compared between periods using the chi-square test, with Fisher exact test applied when expected cell count was less than 5. Prescription-level documentation rates were examined using both crude proportions and models that accounted for within-patient correlation among multiple prescriptions within patients. Differences between the pre-IDS period and IDS period were estimated with binomial generalized estimating equations (identity link), patient number (de-identified) specified as repeated-subject clustering variable to account for prescription sequential order number within subject, and exchangeable working correlation structure with robust (sandwich) standard errors. Results are reported as absolute risk differences with 95% confidence intervals (CIs). The influence of commercial availability (drug and formulation) and formulation type were also examined; for each factor, a separate model included main effects for study period and the factor, plus their interaction, to assess whether associations varied by study period. As a final step, the proportion of prescriptions with documentation on the EHR medication list that was complete and accurate was compared for formulation, dose, route, frequency, and investigational drug alert. All analyses were performed using SPSS v29.0.
This exploratory study was based on a fixed study period expected to yield approximately 200 eligible prescriptions, which was considered sufficient to estimate overall documentation rates, explore documentation patterns by prescription characteristics, and provide adequate power for the expected large effect in the primary comparison. Power calculations for the primary prescription-level comparison used a two-sided α of 0.05 and 80% power, with inflation for within-patient clustering using a design effect of 1 + (m–1)ρ, where m represents the average number of prescriptions per patient and ρ represents the assumed within-patient correlation. Assuming an average of 2 prescriptions per patient, within-patient correlations of 0.05 to 0.20, and an increase in documentation from 30% to 90%, the estimated required sample size was approximately 22 to 24 total prescriptions.
Results
A total of 174 prescriptions issued for 97 unique patients were included. Patient demographics are displayed in Table 1. Overall, 67.2% of prescriptions were for commercially available drugs, and 54.0% used a commercially available formulation (Table 1). Although the percentage of capsule and tablet formulations was similar across periods, the IDS period showed a significantly higher percentage of oral liquid formulations compared with the pre-IDS period (33.3% vs 17.8%), P < .001 (Table 1).
Patient Demographics and Characteristics of Investigational Drug Prescriptions in Pre-IDS and IDS Periods.
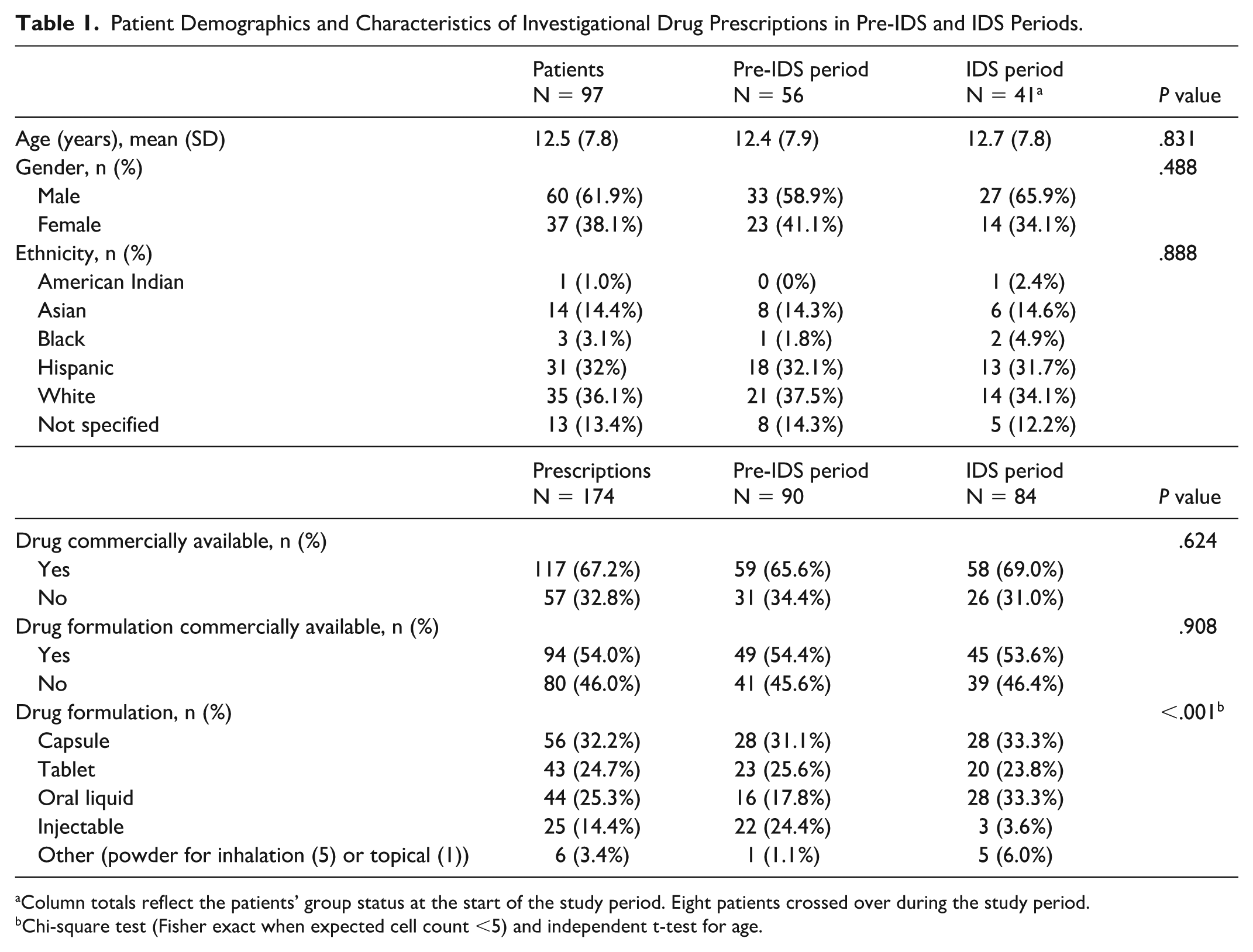
Column totals reflect the patients’ group status at the start of the study period. Eight patients crossed over during the study period.
Chi-square test (Fisher exact when expected cell count <5) and independent t-test for age.
Documentation of investigational drugs on the EHR medication list was 30.0% overall in the pre-IDS period, and remained below 50% regardless of commercial availability or formulation type. Documentation was higher for commercially available than noncommercially available drugs (33.9% vs 22.6%, Table 2), but this difference was not statistically significant after adjustment for clustering by patient (P = 0.152). Likewise, cluster-adjusted comparisons showed no significant differences across formulation types, although lower for oral solids versus oral liquids (29.4% vs 43.8%, P = 0.362) and injectables (29.4% vs 22.7%, P = 0.506). Together, these findings indicate that the low rate of documentation in the pre-IDS period was broad-based rather than limited to specific drug or formulation characteristics. These within-pre-IDS subgroup comparisons were used to assess whether low medication list documentation was concentrated within specific drug or formulation characteristics; the cluster-adjusted percentage point differences and P values are reported in the text but not displayed in Table 2.
Documentation of Investigational Drugs on the Medication List During the Pre-IDS and IDS Periods.
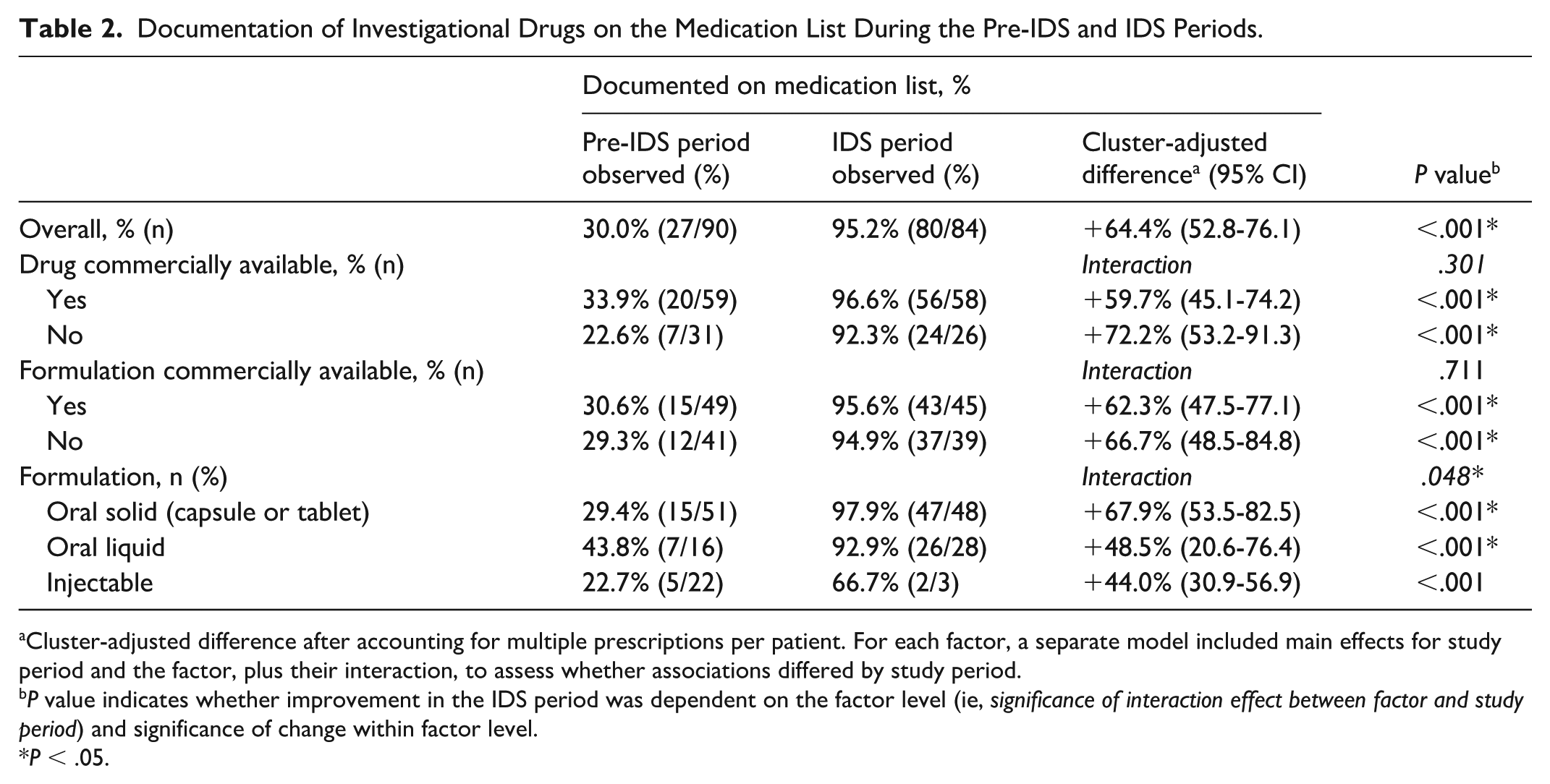
Cluster-adjusted difference after accounting for multiple prescriptions per patient. For each factor, a separate model included main effects for study period and the factor, plus their interaction, to assess whether associations differed by study period.
P value indicates whether improvement in the IDS period was dependent on the factor level (ie, significance of interaction effect between factor and study period) and significance of change within factor level.
P < .05.
The overall documentation rate increased from 30.0% in the pre-IDS period to 95.2% in the IDS period after implementation of IDS pharmacist documentation, corresponding to a cluster-adjusted absolute increase of 64.4 percentage points (95% CI 52.8, 76.1; P < .001) (Table 2). Documentation increased across formulation types, but gains differed by formulation (P = 0.048), with the largest increase observed for oral solids (absolute increase: 67.9 percentage points; 95% CI 53.5, 82.5).
The accuracy of medication documentation improved significantly from the pre-IDS to the IDS period (Figure 1). Before IDS implementation, complete and correct documentation was low across all medication list elements, ranging from 6.7% for formulation to 28.9% for route, indicating poor completeness across all fields. Following IDS implementation, complete and correct documentation rose to 94% or higher for every field, including formulation (95.2%), dose (94.0%), route (95.2%), frequency (94.0%), and investigational drug alerting (95.2%) (all P < .001).
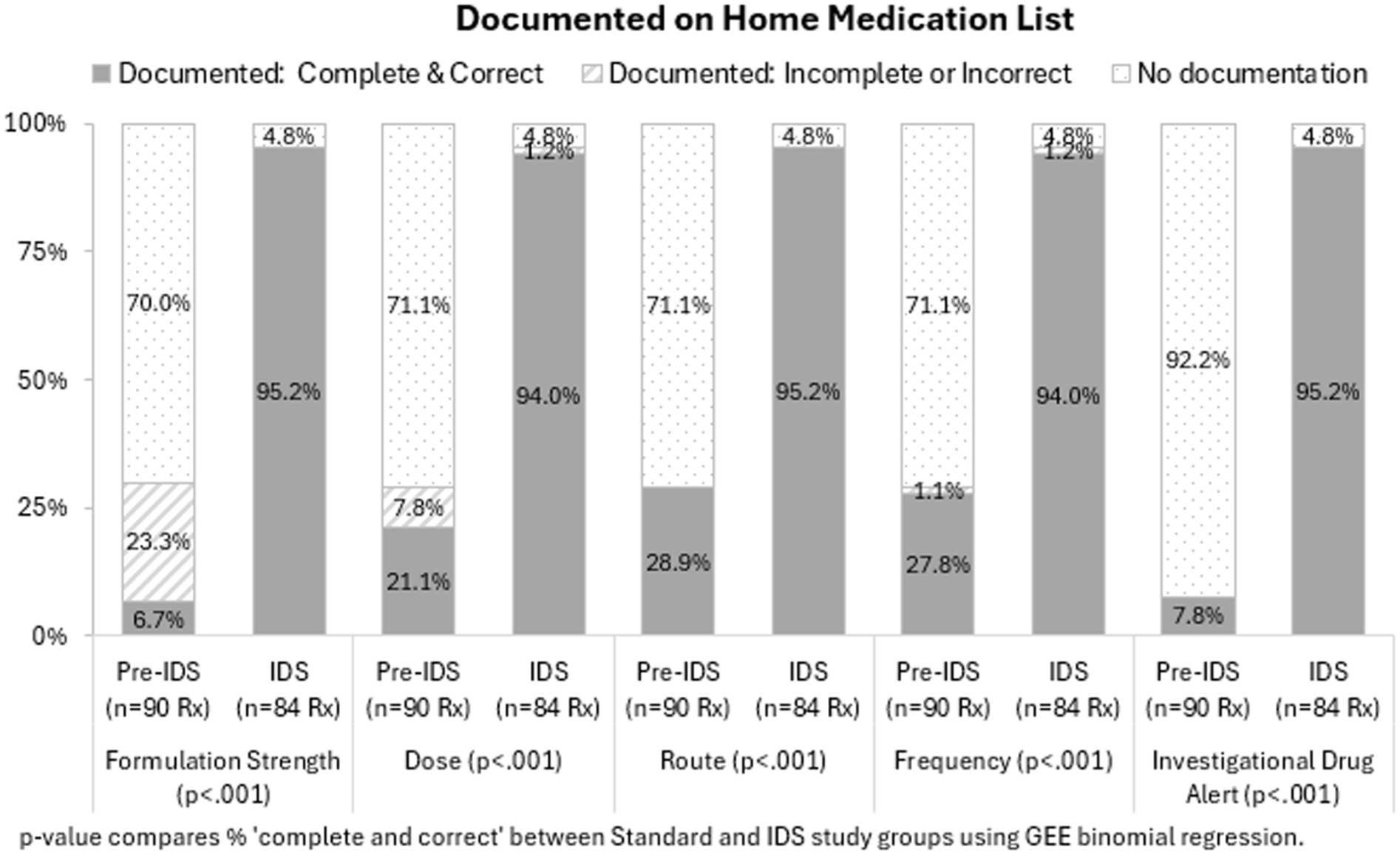
Documentation of investigational drug details on the medication list.
In the pre-IDS period, when IDS pharmacists were not involved in the documentation process, only 30% of investigational drugs were documented on the EHR medication list by physicians, nurse practitioners, or medical assistants, while 70% were not documented (Figure 2). These findings suggest that investigational drug documentation was frequently overlooked in the absence of pharmacist involvement.
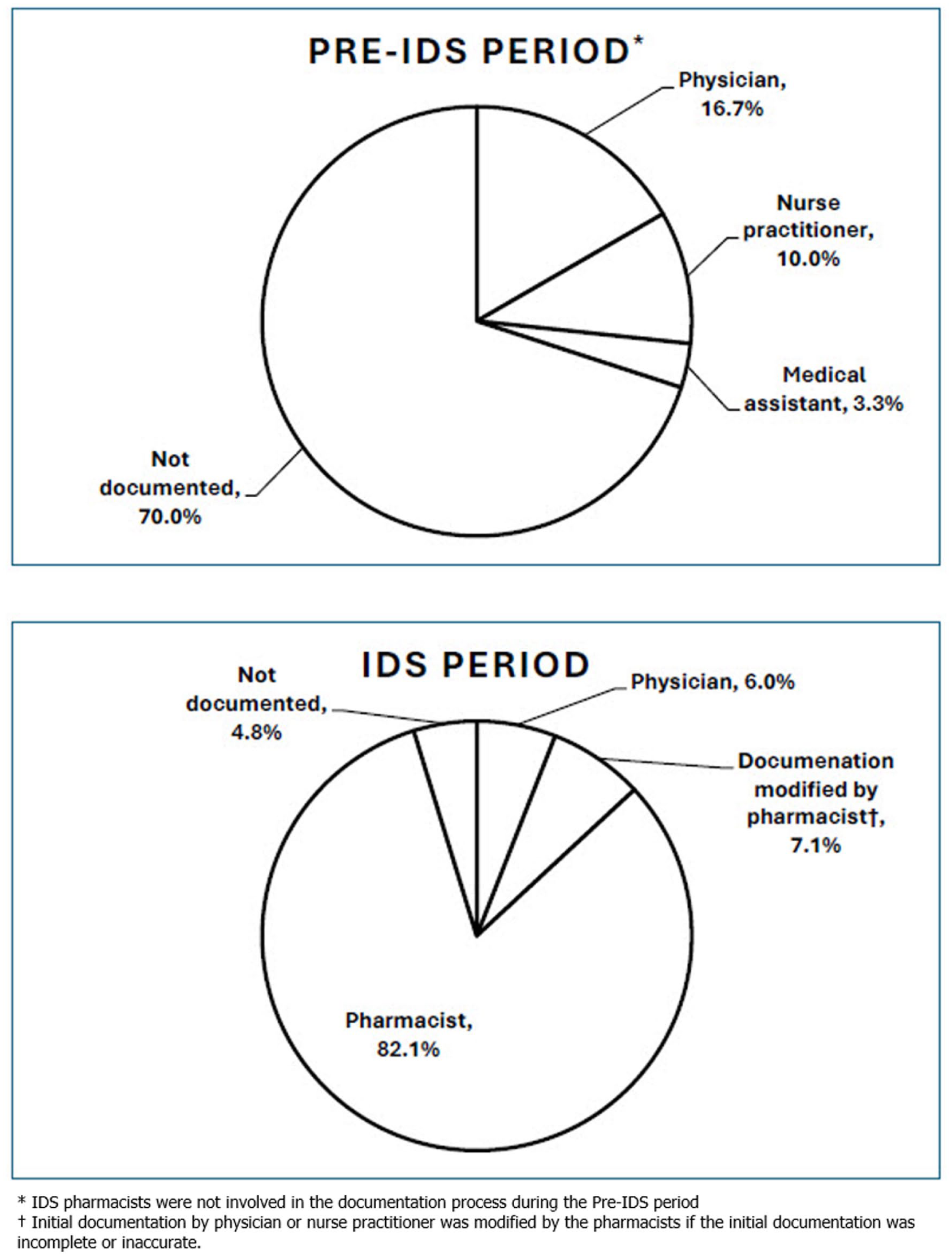
Role of individuals documenting investigational drugs on the medication list.
By contrast, in the IDS period, when IDS pharmacists participated in the documentation process, 95.2% of investigational drugs were documented, and IDS pharmacists completed the initial documentation for 82.1% of the prescriptions (Figure 2). For an additional 7.1% of prescriptions, documentation was initially entered by another health care professional and then modified by pharmacists for accuracy and completeness, whereas 6.0% were documented by a physician and required no pharmacist modification (Figure 2).
Discussion
Previous studies have demonstrated a reduction in medication discrepancies when the task of medication reconciliation is assigned to pharmacists and pharmacy technicians.1,4,5 This reduction in discrepancies may be due to the reassignment of the task from a large group of nurses and physicians with many diverse responsibilities to a smaller pharmacy group focused on medications. Similarly, IDS pharmacy-led documentation of investigational drugs on the EHR medication list was successful in increasing the rate and accuracy of documentation. There was a 64.4% improvement (cluster-adjusted difference) in overall documentation of investigational drugs (Table 2), and an increase from 7.8% to 95.2% for inclusion of an investigational drug alert (Figure 1). It is very important for investigational drugs to be included on the medication list for health care providers to be aware of potential drug interactions, adverse effects, or duplication of therapy. When investigational drugs are also commercially available, it is important to include an investigational drug alert to prevent inadvertent prescribing and dispensing of commercial drug supply when investigational drug supply should be used. The pharmacists working in the IDS are ideal candidates to assume responsibility for documenting investigational drugs on the EHR medication list because they have a specialized focus on investigational drug dispensing and their smaller group size may facilitate training and consistency for documentation procedures compared with other provider groups.
Heath et al 4 found that 60% of medication discrepancies for pediatric patients involve oral liquid formulations. It was anticipated that oral liquids might be vulnerable to incomplete documentation in this study because of the added complexity of specifying administered volume and product concentration. In the pre-IDS period, 56.2% of oral liquid formulations were not documented on the medication list (Table 2), a proportion similar to the 60% discrepancy rate reported by Health et al. Although oral liquid documentation (43.8%) was numerically higher than oral solid documentation (29.4%), the difference was not significantly significant (P > 0.05).
In a study by Redic et al, 9 only 20 of 97 (20.6%) investigational drugs reviewed were included on EHR medication lists for adult patients enrolled in a clinical trial. The 30% documentation rate during the pre-IDS period of this study was also very low. Although most institutions have transitioned to electronic drug and order builds for commercially available medications, many institutions continue to use paper orders and free-text entries for investigational drugs. For example, Redic et al 9 described using free-text entries to document investigational drugs on the medication list. At Rady Children’s Hospital Orange County, most investigational drugs are not built in the EHR drug database (Cerner), and thus not readily available to select when electronically documenting medications. The lack of availability of a prebuilt drug product and need for free-text entry may be one factor contributing to the low documentation rate for investigational medications.
Since investigational drugs are not built in the system, health care providers must use a free-text nonformulary entry to add investigational drugs to the medication list. This manual free-text step creates potential for transcription or omission errors, whereas addition to the medication list would be automatic for medications built in the EHR system and prescribed electronically. Even if the investigational drug is commercially available, the commercial drug product should not be added to the medication list without an investigational drug alert due to the risk providers may inadvertently send a prescription to a local pharmacy to be filled with commercial drug supply. If dispensed, the commercial drug might be administered instead of investigational supply which would be a protocol deviation, or duplication of therapy may occur due to differences in nomenclature (eg, brand name, generic name, or alphanumeric code used during drug development). Thus, an investigational drug build with an investigational alert (eg, INV- prefix) is important for accurate entry on the medication list. When investigational drug products are not available in the EHR, the additional time required to create a free-text entry with an investigational drug alert may contribute to low documentation rates. Future strategies to address this gap may include dedicated investigational drug builds and improved IDS-EHR integration, although these approaches require internal and external validation before implementation.
A barrier to building investigational drugs in the EHR drug database is the time required from IDS pharmacists and information systems pharmacists to build the investigational drug products and orders, perform quality checks to ensure accurate build and functionality, and maintain the build when interim study results are reviewed and protocols amended. Future studies evaluating whether EHR build of investigational drugs and orders, together with ongoing quality assurance processes, improves medication documentation and reduces errors would be valuable and may improve overall medication safety for patients participating in research.
Investigational drug service pharmacy-led documentation improved the rate and accuracy of documentation, but documentation was still missing in 4.8% of prescriptions during the IDS period (Figure 2). The IDS pharmacists dispense investigational drugs using a specialty IDS system, review the medication list in the EHR, and then manually add or modify investigational drugs on the medication list. If the IDS system and EHR system were integrated and investigational drugs available as prebuilt entries in both systems, an automated process might further improve rate and accuracy of documentation.
A limitation of this study was the retrospective single-center design in a pediatric setting. In addition, the study was focused on accurate documentation of medications on the EHR medication list. Other studies have demonstrated the effect of medication discrepancies on patient care at admission and discharge, but this study focused on documentation rates and accuracy. 5 In addition, the number of outpatient investigational drug dispensing events within individual hospital departments was limited, which constrained department-specific comparisons.
Conclusion
Low rates of investigational drug documentation in prior studies and in the pre-IDS period of this study highlight a clear need for improved medication list documentation processes. Investigational drug service pharmacist involvement improved the overall rate and accuracy of documentation. Future studies should assess whether building investigational drugs in the EHR drug database and integrating IDS and EHR systems can further improve documentation and medication safety.
Footnotes
Acknowledgements
N/A.
Abbreviations
EHR, electronic health record; FDA, Food and Drug Administration; IDS, investigational drug service; IND, investigational new drug.
Ethical Consideration
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant international guidelines on human experimentation and have been approved by the appropriate committees at Rady Children’s Hospital Orange County.
Consent to Participate
Given the nature of this study, informed consent was not required by the institutional review board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.