
Abstract
Background:
Valacyclovir requires dose adjustment according to renal function to prevent serious adverse events. However, real-world data on renal function-based dosing practices are limited.
Objective:
To evaluate the frequency of valacyclovir overdosing according to renal function and to identify the characteristics associated with overdosing in Japan.
Methods:
We conducted a retrospective cohort study using a nationwide database of administrative claims and laboratory results from acute care hospitals in Japan. We included adults aged ≥18 years who received at least 1 valacyclovir prescription between October 1, 2022, and September 30, 2024, and who had a serum creatinine measurement within the preceding year. The primary outcome was overdosing, defined as a prescribed dose that exceeded the maximum recommended dose for the patient’s renal function level per the Japanese package insert. Renal function was estimated using creatinine clearance calculated with the Cockcroft-Gault equation.
Results:
A total of 6764 patients with 7901 valacyclovir prescriptions were included; 1649 prescriptions (20.9%) were for patients with impaired renal function. Overdosing was rare among patients with normal renal function. Among patients with impaired renal function, overdosing occurred in 25.1% of prescriptions for varicella or herpes zoster and in 6.4% for other indications. Overdosing was more frequent among women and most common for prescriptions dispensed at community pharmacies.
Conclusions:
In this nationwide study, valacyclovir overdosing was common among patients with impaired renal function, particularly for high-dose indications, and occurred more frequently among women and for prescriptions dispensed at community pharmacies. Strengthening renal function-based prescription review may help reduce preventable overdosing.
Introduction
Valacyclovir, an antiviral prodrug of acyclovir, is widely prescribed for the treatment of herpes zoster and herpes simplex worldwide, including in Japan. 1 As valacyclovir is primarily eliminated by the kidneys, dose adjustment based on renal function is required to prevent drug accumulation and subsequent adverse events. 2 Given its widespread use in routine clinical practice, inappropriate dosing may affect a substantial number of patients.
Inadequate valacyclovir dose adjustment among patients with impaired renal function has been associated with serious adverse events, including acute kidney injury and toxic encephalopathy, in case reports and small observational studies.2,3 Furthermore, an analysis of a Japanese spontaneous adverse event reporting database suggested that valacyclovir was among the drugs most frequently reported as suspected causes of acute kidney injury.4,5 As these adverse effects are largely preventable through appropriate dose adjustment, understanding real-world dosing according to renal function is a clinically important issue. However, population-level data describing how valacyclovir is dosed according to renal function remain limited worldwide. Prior evidence has been limited to case reports and small observational studies conducted in restricted patient populations,2,3,6 and no nationwide analysis has examined renal function-based valacyclovir dosing.
We used a large hospital-based administrative claims database covering acute care hospitals with linked laboratory data to evaluate valacyclovir dosing according to renal function in real-world clinical practice in Japan. This database allows longitudinal linkage of prescriptions and laboratory test results at the individual patient level. Specifically, we assessed the frequency of overdosing in relation to renal function and evaluated the patient characteristics associated with overdosing.
Methods
Study Design and Data Source
This retrospective cohort study was conducted using data from a nationwide medical information database (Medical Data Vision [MDV] Co. Ltd., Tokyo, Japan). 7 This database contains anonymous medical fee claims, Diagnosis Procedure Combination (DPC) data, and laboratory test results from acute care DPC hospitals in Japan. 8 The database enables longitudinal linkage of medical fee claims, prescriptions, and laboratory test results at the individual patient level. Data from October 1, 2021, to September 30, 2024, were analyzed. Patients were eligible for inclusion if they had at least 1 serum creatinine (SCr) measurement during this period.
Study Population and Exposure
Patients were included if they received at least 1 valacyclovir prescription between October 1, 2022, and September 30, 2024. For each valacyclovir prescription, renal function was estimated using the most recent laboratory test result obtained within 1 year prior to the prescription date. Accordingly, laboratory test results from October 1, 2021, onward were used for renal function assessment. Patients were excluded if (1) their hospital started or stopped contributing data to MDV during the study period or (2) they were aged <18 years as of October 1, 2021, because renal function was estimated using the Cockcroft-Gault equation, 9 which was developed for adults. The exposure was defined as any valacyclovir prescription written at one of the study hospitals, whether dispensed in-hospital or at a community pharmacy. Valacyclovir recorded as a medication brought in by the patient at the time of hospital admission was not included.
Outcome
The primary outcome was overdosing at the prescription level. Because recommended valacyclovir doses differ by indication, overdosing was defined conservatively using the maximum recommended daily dose for herpes zoster or varicella, the highest approved daily dose at each renal function level. Thus, regardless of the clinical indication, overdosing was defined as a valacyclovir dose higher than this renal function–specific maximum daily dose, as specified in the Japanese package insert for VALTREX tablets 500 mg. 10 The renal dose-adjustment criteria from the package insert are provided in English translation in Supplementary Table S1. Eligible valacyclovir prescriptions served as the denominator. In a subgroup analysis, the frequency of valacyclovir overdosing for varicella or herpes zoster prescriptions was determined according to patients’ renal function.
Variables and Definitions
Data on age, sex, renal function, dispensing setting, and indication for varicella or herpes zoster were collected from the database and were complete for all included prescriptions.
Renal Function
Renal function was assessed using creatinine clearance (CCr), estimated using the Cockcroft-Gault equation based on the most recent renal function measurement obtained within 1 year prior to the valacyclovir prescription. SCr concentrations ≤ 0.3 mg/dL or ≥ 30 mg/dL were excluded as extreme values. In particular, SCr concentration ≤ 0.3 mg/dL was considered unreliable for renal function estimation using the Cockcroft-Gault equation, 9 as such unusually low SCr is more likely to reflect markedly reduced muscle mass associated with conditions such as sarcopenia or frailty, rather than true renal function. When multiple SCr measurements were available on the same day, the lowest concentration was selected to minimize potential underestimation of renal function and the resulting risk of false classification of prescriptions as overdoses. If SCr was unavailable but estimated glomerular filtration rate (eGFR) was recorded, CCr was recalculated from the eGFR. Prescriptions for which neither SCr nor eGFR was available within 1 year prior to the prescription date were excluded because renal function could not be estimated. Body weight was parameterized using sex- and age-specific mean values derived from national population statistics (Statistics of Japan, e-Stat 11 ) for all patients, regardless of whether individual body weight was recorded, because body weight was available for some inpatients but was not routinely captured for outpatients (meaning it was unavailable for the majority of outpatient cases in the database). This enabled standardized estimation of CCr at the population level. Accordingly, body weight was not treated as missing data in the analyses.
Dialysis Status
The patients were defined as receiving dialysis if their records included specific procedure codes for hemodialysis or maintenance dialysis (Supplementary Table S2). Their dialysis status started on the first documented dialysis date. Prescriptions for patients on dialysis were analyzed separately from the CCr-based groups.
Varicella/Herpes Zoster Indication
Prescriptions were defined as being for varicella or herpes zoster if a confirmed diagnosis code from the International Classification of Diseases, 10th Revision (ICD-10; Japan, 2013 version), 12 was recorded 1 day before, on, or 1 day after the prescription date (B01 for varicella; B02 for herpes zoster). Prescriptions that also had a confirmed herpes simplex diagnosis (A60 or B00) within the same time frame were excluded. “Confirmed” indicates that the diagnosis status was recorded as confirmed in the database (Supplementary Table S3).
Dispensing Setting
Prescriptions were classified as inpatient, in-hospital, or community pharmacy based on the encounter status and dispensing fee codes in the database. Community pharmacy dispensing was identified by claims for the fee associated with issuing outpatient prescriptions for external dispensing.
Statistical Analysis
Continuous variables are summarized as the median (interquartile range), and categorical variables are summarized as count (percentage). Patient characteristics between the normal renal function (CCr ≥ 50 mL/min) and impaired renal function (CCr < 50 mL/min or receipt of dialysis) groups were compared using the Wilcoxon rank-sum test for continuous variables and either Pearson’s chi-square test or the Cochran-Armitage trend test for categorical variables. Among patients with impaired renal function and varicella or herpes zoster as the indication, the overdosing group was compared with the appropriate dosing group in terms of sex, age, and dispensing setting using the same tests. All tests were 2-sided, P-value < .05 was considered statistically significant. All analyses were performed using JMP Pro 18.2.0 (SAS Institute Inc., Cary, North Carolina).
Ethical Considerations
This study used anonymized administrative data. According to applicable local regulations and institutional policies, ethics committee review and informed consent were either waived or not required for this secondary use of anonymized data. This report follows the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) recommendations for observational studies. 13
Results
Study Population
Between October 1, 2022, and September 30, 2024, 6764 patients were included, with 7901 valacyclovir prescriptions analyzed in total, reflecting multiple prescriptions per patient during the study period. Of all prescriptions, 1649 (20.9%) were for patients with impaired renal function (CCr < 50 mL/min or receipt of dialysis). The median age of the overall population was 68 (53-78) years. The median age was 63 (49-74) years in the normal renal function group (CCr ≥ 50 mL/min) and 82 (77-87) years in the impaired renal function group. Prescriptions for varicella or herpes zoster accounted for 42.1% of all prescriptions and were similar across both renal function groups (normal renal function: 42.4%; impaired renal function: 41.4%) (Table 1).
Characteristics of Prescriptions.
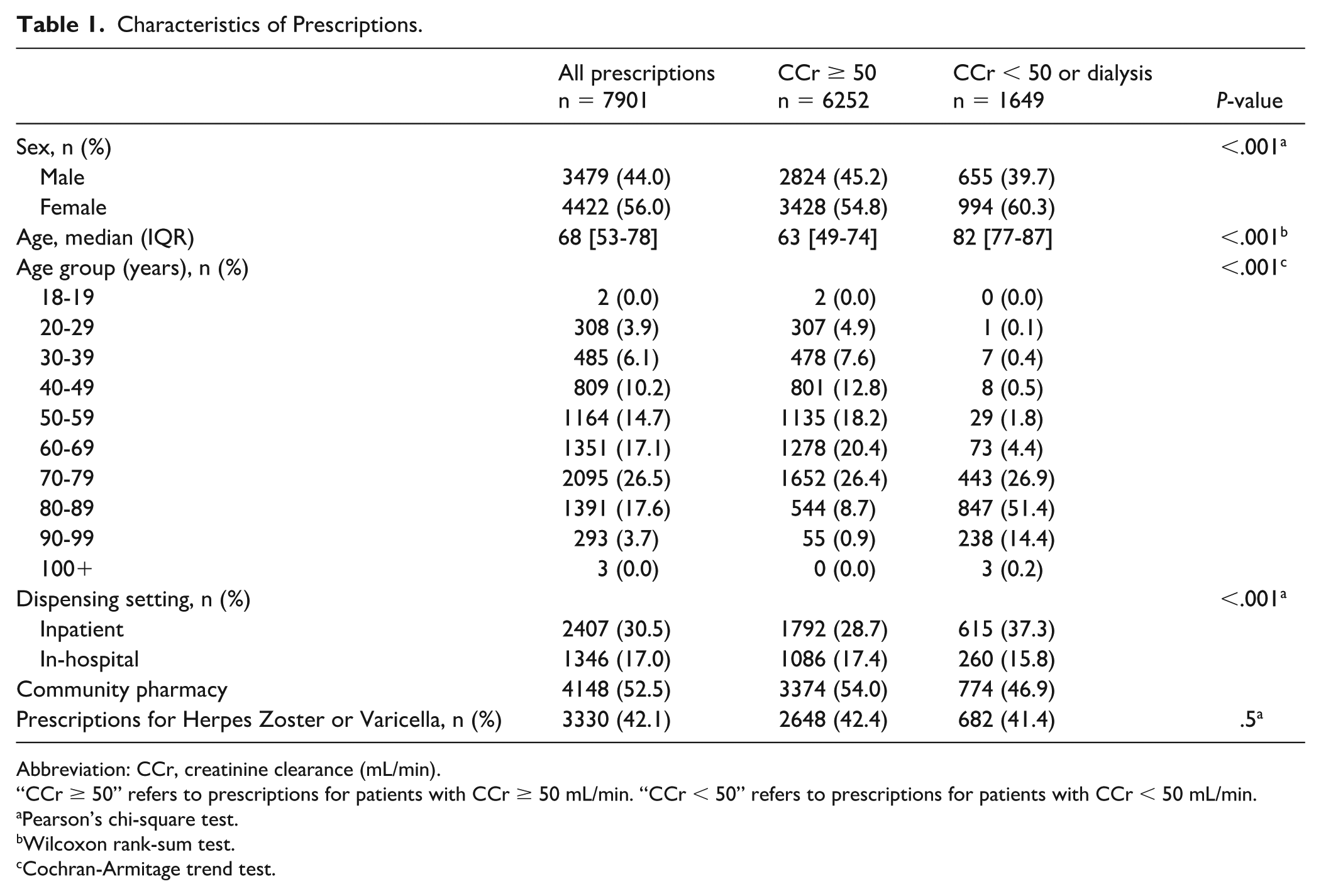
Abbreviation: CCr, creatinine clearance (mL/min).
“CCr ≥ 50” refers to prescriptions for patients with CCr ≥ 50 mL/min. “CCr < 50” refers to prescriptions for patients with CCr < 50 mL/min.
Pearson’s chi-square test.
Wilcoxon rank-sum test.
Cochran-Armitage trend test.
Primary Outcome
Among patients with impaired renal function (CCr < 50 mL/min or receipt of dialysis), overdosing occurred in 25.1% of prescriptions for varicella or herpes zoster and in 6.4% of prescriptions for other indications (Table 2). Overdosing was rare among patients with normal renal function. The overdosing rates were 0.0% for varicella or herpes zoster and 0.1% for other indications. The comparisons of age, sex, and dispensing setting between the overdosing group and the appropriate dosing group are shown in Supplementary Table S4.
Prevalence of Overdosing Based on Renal Function.
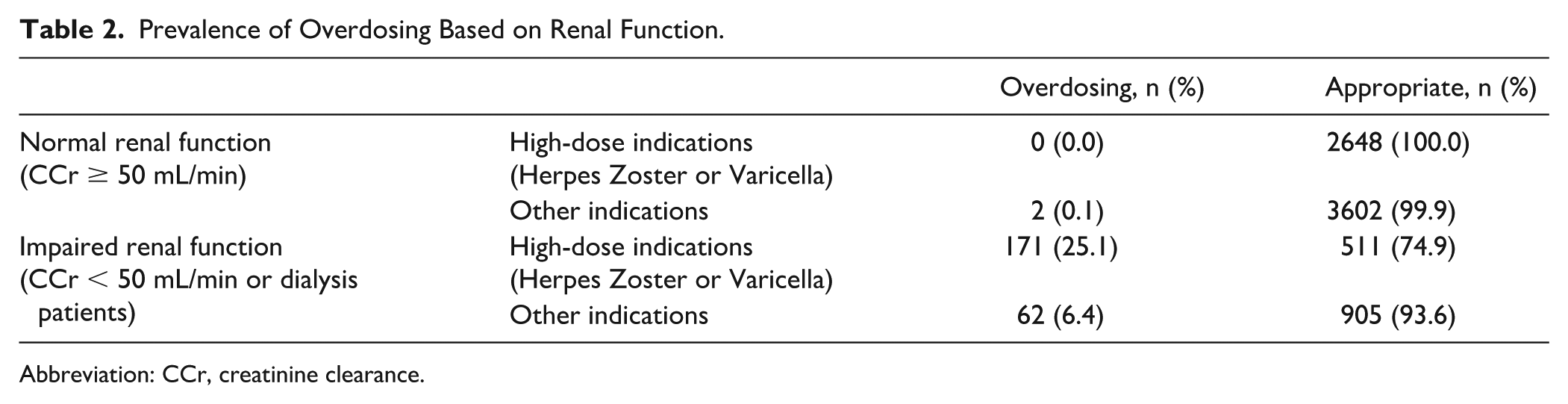
Abbreviation: CCr, creatinine clearance.
Prescriptions for Varicella and Herpes Zoster Among Patients With Impaired Renal Function
Given the high prevalence of overdosing among patients with impaired renal function, particularly for high-dose indications, such as varicella or herpes zoster, a more detailed subgroup analysis was performed. First, to provide a more detailed description of overdosing by renal function, we summarized prescriptions for herpes zoster or varicella according to renal function category and the corresponding recommended daily dose stated in the Japanese package insert (Table 3). Among categories requiring dose reduction, overdosing was observed in 142 of 519 prescriptions (27.4%) in the CCr 30 to 49 mL/min category, 27 of 132 prescriptions (20.5%) in the CCr 10 to 29 mL/min category, and 2 of 4 prescriptions (50.0%) in the CCr <10 mL/min category. No overdosing was observed among patients receiving dialysis. Next, among prescriptions for herpes zoster or varicella in patients with impaired renal function, we compared characteristics between the overdosing and appropriate dosing groups (Table 4). The proportion of women was higher in the overdosing group than in the appropriate dosing group (65.5% vs 56.4%; P = .04). Age did not differ between the overdosing and appropriate dosing groups (84 [79-87] vs 82 [77-88]; P = .3). By dispensing setting, overdosing prescriptions were most frequently dispensed at community pharmacies (64.9%), followed by hospital outpatient pharmacies (23.3%) and inpatient settings (11.7%).
Overdosing According to Recommended Daily Dose Based on Renal Function Among Prescriptions for Herpes Zoster or Varicella.
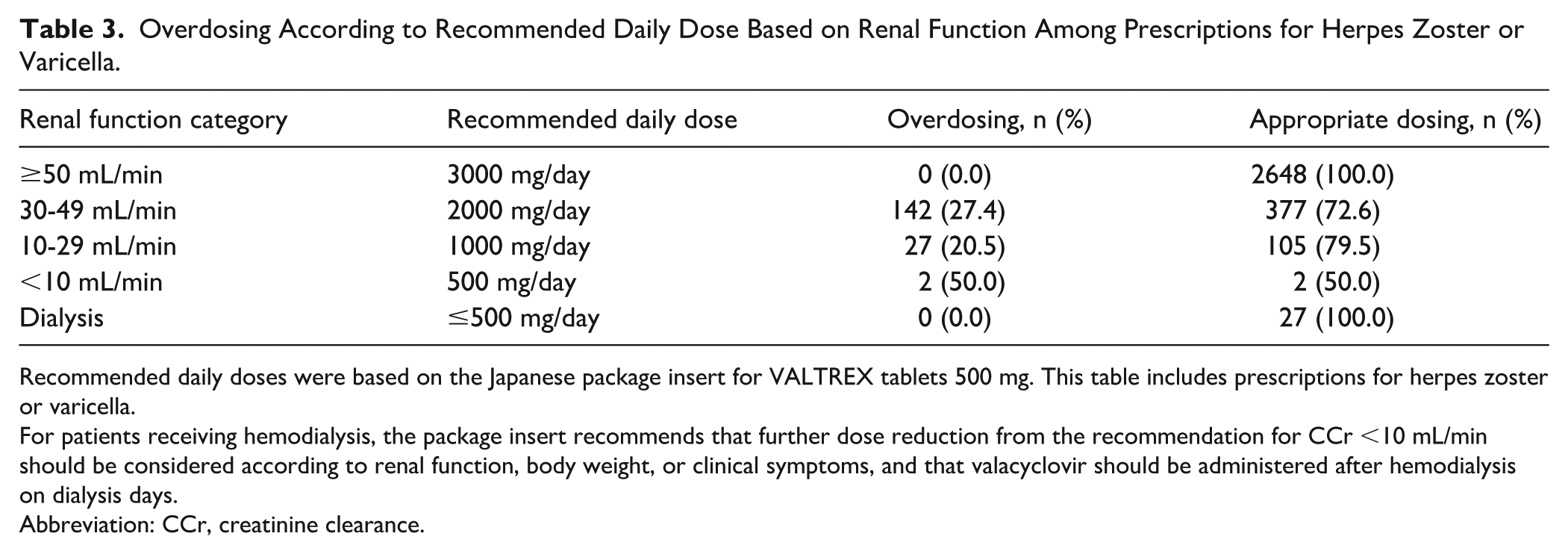
Recommended daily doses were based on the Japanese package insert for VALTREX tablets 500 mg. This table includes prescriptions for herpes zoster or varicella.
For patients receiving hemodialysis, the package insert recommends that further dose reduction from the recommendation for CCr <10 mL/min should be considered according to renal function, body weight, or clinical symptoms, and that valacyclovir should be administered after hemodialysis on dialysis days.
Abbreviation: CCr, creatinine clearance.
Overdosing Versus Appropriate Dosing in Valacyclovir Prescriptions for Herpes Zoster or Varicella Among Patients, by Patient Characteristics.
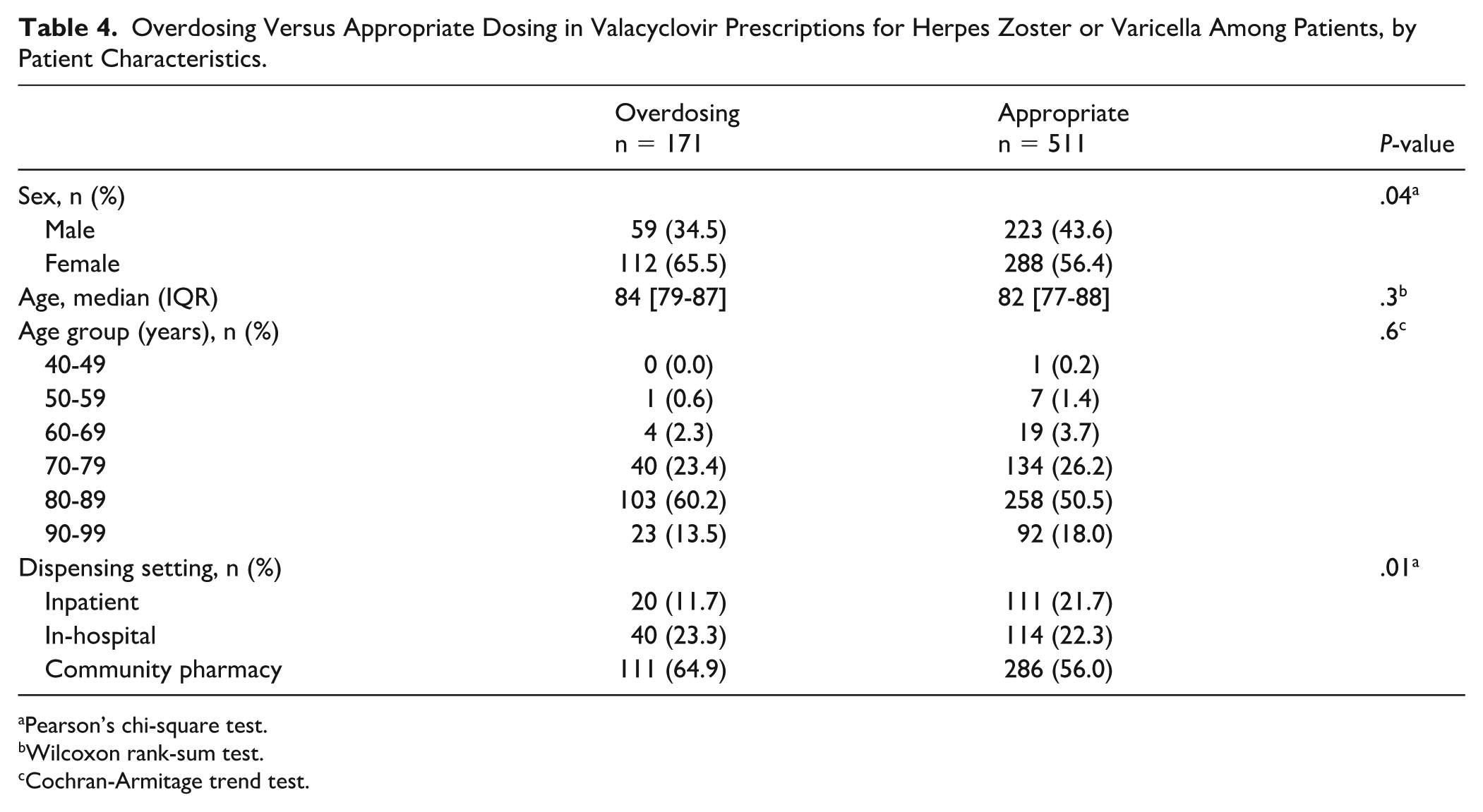
Pearson’s chi-square test.
Wilcoxon rank-sum test.
Cochran-Armitage trend test.
Discussion
This study revealed that among patients with impaired renal function, valacyclovir was frequently prescribed at doses exceeding the maximum renal function–adjusted dose specified in the Japanese package insert. 10 Overdosing occurred more frequently for prescriptions indicated for varicella or herpes zoster, in women, and dispensed at community pharmacies. These findings highlight gaps between recommended renal function–based dosing and actual prescribing practices in routine clinical care in Japan.
To our knowledge, no previous large-scale claims-based studies have comprehensively evaluated valacyclovir dosing appropriateness in relation to renal function, and this study represents the first such analysis using nationwide laboratory-linked data. Previous evidence has consisted mainly of case reports and systematic reviews of such reports, with no large-scale claims-based investigations assessing the real-world prevalence of valacyclovir overdosing.2,3,14 Although overdosing among patients on dialysis has been reported, 3 prior studies have not evaluated dosing practices across the broader patient population. By leveraging a nationwide claims database with linked laboratory data, our study provides an assessment of valacyclovir overdosing across the entire population of patients treated with this drug in routine clinical practice.
Among patients with impaired renal function (CCr < 50 mL/min or receiving dialysis), overdosing occurred for 25.1% of prescriptions for varicella or herpes zoster. In Japan, the approved dose of valacyclovir differs by indication (3000 mg/day for herpes zoster or varicella and 1000 mg/day for herpes simplex in patients with normal renal function), and herpes zoster and varicella require higher daily doses than other indications. 10 As the risk of adverse drug reactions is driven primarily by drug exposure rather than by the indication itself, appropriate dose reduction becomes essential when renal function is impaired. Accordingly, prescriptions combining high-dose indications and impaired renal function represent a particularly high-risk context for valacyclovir overdosing. In this study, approximately 1 in 4 such prescriptions demonstrated overdosing, highlighting the need for more careful renal function–based dosing in clinical practice.
The detailed analysis by renal function category and renal function–based recommended daily dose showed that overdosing was concentrated in categories requiring dose reduction, particularly in the CCr 30 to 49 mL/min category. Although the proportion of overdosing was highest in the CCr <10 mL/min category, the number of prescriptions in this category was small. In contrast, the CCr 30 to 49 mL/min category accounted for most overdosing events. This suggests that moderate renal impairment may be particularly prone to missed dose reduction in routine practice. Because moderate renal impairment may be overlooked more easily than severe impairment, the standard high-dose regimen may be continued unintentionally. These findings emphasize the importance of actively calculating renal function when prescribing or dispensing valacyclovir.
The higher proportion of women among the overdosed patients may reflect sex-related differences in renal function. Women generally have a smaller body size and lower glomerular filtration rates than men, 15 and they may require dose reduction even when SCr falls within the normal range. As a result, reliance on SCr alone may obscure clinically relevant renal impairment, particularly in women, 16 potentially increasing the risk of inappropriate dosing.
Overdosing was most frequent at community pharmacies, accounting for more than half of all cases of prescription overdosing. However, unlike hospital settings, community pharmacies often lack access to laboratory information at the time of dispensing. Previous surveys have suggested that renal function ascertainment in community pharmacy settings may be limited,17,18 which represents a structural barrier to adequate renal function–based prescription review. Improving access to renal function information and strengthening renal function–based prescription review in community pharmacy settings may help reduce valacyclovir overdosing.
Excessive exposure to valacyclovir and its active metabolite, acyclovir, may lead to clinically important toxicity, particularly neurotoxicity, as well as acute kidney injury. Neurotoxicity may present with confusion, hallucinations, agitation, altered consciousness, dysarthria, tremor, or myoclonus, whereas acute kidney injury may present with increased SCr or reduced urine output.2,14 In the present study, many overdosing prescriptions were dispensed at community pharmacies. Therefore, these potential toxicities are clinically relevant not only in inpatient settings but also in outpatient and community-based medication management.
This study had several limitations. First, this study did not assess clinical outcomes associated with valacyclovir dosing, including both adverse events related to overdosing and treatment effectiveness. Although the database used in this study may contain diagnostic codes or other records suggestive of adverse events, it does not provide sufficient information to determine whether these events were caused by inappropriate dosing. Furthermore, patients with herpes zoster often do not revisit medical institutions after completing treatment, making it difficult to capture subsequent clinical outcomes. Moreover, patients are no longer tracked after changing medical institutions, and subsequent outcomes cannot be captured. Therefore, the associations between valacyclovir dosing and subsequent clinical outcomes remain unclear. Second, only patients who had at least 1 renal function measurement within 1 year before the prescription date were included. Patients without renal function testing in the prior year were excluded, even though some of them may have also received valacyclovir. Therefore, overdosing among patients whose renal function was not measured could not be assessed in this analysis, which could lead to potential underestimation of the true frequency of overdosing. Third, the database used in this study included data from large acute care hospitals that participate in the DPC system.19,20 These hospitals typically have well-established laboratory testing systems and can obtain renal function results promptly. Smaller hospitals and clinics may not have the same testing capacity. Consequently, overdosing in other healthcare settings in Japan may have been underrepresented. Fourth, renal function was estimated using the most recent laboratory value prior to the prescription date. Although laboratory measurements could have been obtained up to 1 year before prescribing, 61.4% of the prescriptions were based on renal function measurements obtained on the same day or within 1 day prior to the prescription, and more than 81.6% were based on measurements obtained within 4 weeks. These findings suggest that temporal misalignment between laboratory assessment and prescribing was limited in most cases. Moreover, even when earlier laboratory values were used, renal function generally declines over time21,22; therefore, any misclassification arising from the use of earlier measurements would be expected to bias the results toward underestimation of overdosing rather than overestimation. Fifth, renal function was derived from a single laboratory measurement. Short-term changes occurring between measurements—such as acute kidney injury or transient declines—may not have been captured. These unmeasured fluctuations might have influenced the determination of overdosing. Sixth, detailed clinical information, such as disease severity, treatment strategy, and prescribing intentions, was unavailable. Some doses that exceeded recommendations adjusted for renal function may have been intentionally prescribed for clinical reasons. Therefore, not all identified overdoses should be considered inappropriate prescribing. Seventh, CCr was estimated using average body weight values derived from national statistics because individual body weight was often unavailable, particularly for outpatients. This approach enabled standardized estimation of CCr at the population level; however, when a patient’s actual body weight differs from the population average, estimation error may occur, which could affect the classification of overdosing. In addition, CCr estimation using the Cockcroft-Gault equation is challenging in older adults. The Cockcroft-Gault equation depends on SCr and body weight; therefore, reduced muscle mass or sarcopenia, which is common in older adults, may lower SCr and lead to overestimation or misclassification of renal function. 23 Such overestimation may have led to under-recognition of the need for renal dose reduction and, consequently, underestimation of overdosing. Because most overdosing events occurred in patients older than 70 years, such estimation error may have affected overdose classification. However, although these limitations may have affected overdose classification, the observed frequency of overdosing suggests that renal function–based dose adjustment remains important in routine practice.
Conclusions
In this nationwide claims-based study using linked laboratory data, valacyclovir overdosing was common among patients with impaired renal function, particularly for high-dose indications, such as varicella or herpes zoster. Overdosing occurred more frequently among women and for prescriptions dispensed at community pharmacies. These findings underscore the importance of incorporating renal function information into dosing decisions and strengthening renal function–based prescription review, especially in settings where access to laboratory data may be limited.
Supplemental Material
sj-docx-1-pmt-10.1177_87551225261462036 – Supplemental material for Inappropriate Valacyclovir Dosing by Renal Function in Japan
Supplemental material, sj-docx-1-pmt-10.1177_87551225261462036 for Inappropriate Valacyclovir Dosing by Renal Function in Japan by Sumire Suzuki, Yuki Kondo, Kaho Sato, Yuka Sakazaki, Yoshiko Tominaga, Koji Sato and Yoichi Ishitsuka in Journal of Pharmacy Technology
Footnotes
Acknowledgements
Authors’ Note
Part of the data from this study was previously presented as an oral presentation at the 19th Annual Meeting of the Pharmacy Society of Japan, a domestic academic conference held at the Sapporo Convention Center, Sapporo, Japan, November 1 and 2, 2025.
Ethical Considerations
This study used anonymized administrative data. Under applicable local regulations and institutional policy, ethics committee review was not required for this secondary use of anonymized data.
Consent to Participate
Under applicable local regulations and institutional policy, informed consent was not required for this secondary use of anonymized administrative data.
Author Contributions
SS and YK conceived and designed the study. KaS, YS, YT, KoS, and YI contributed to the conception of the study. SS contributed to data acquisition and interpretation. YK and KaS contributed to data acquisition, analysis, and interpretation. YS contributed to data analysis and interpretation. YT, KoS, and YI contributed to data interpretation. SS and YK drafted the manuscript. All authors critically revised the manuscript for important intellectual content, approved the final version of the manuscript, and agreed to be accountable for all aspects of the work in ensuring its integrity and accuracy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (grant number JP22K10387) and by a scholarship donation from Japan Pharmaceutical Association and Minami-Nihon Pharmaceutical Center.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YI reports having patents or royalties with the Safety Medical System Laboratory Corporation. YK reports receiving research funding from Safety Medical System Laboratory Corporation; having patents or royalties with the Safety Medical System Laboratory Corporation; and serving in an advisory or leadership role for Safety Medical System Laboratory Corporation (unpaid). All remaining authors have nothing to disclose.
Data Availability Statement
The datasets generated and/or analyzed during this study were obtained from Medical Data Vision Co. Ltd. They are not publicly available. Data may be available from the corresponding author on reasonable request and with permission from Medical Data Vision Co. Ltd.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.