
Abstract
Objective:
The aim of this study was to determine if the fetal cerebellum can be used as a predictor of gestational age (GA), in comparison with other biometric parameters, such as fetal head circumference (HC), biparietal diameter (BPD), abdominal circumference (AC), and femur length (FL).
Materials and Methods:
A grayscale sonographic examination was completed on a cohort of 200 pregnant participants, during their second and third trimester. A descriptive analysis was used to determine the fetal GA, utilizing the transcerebellar diameter (TCD), while comparing it with other biometry metrics. The mean and standard deviation were provided for quantitative variables, while frequencies were determined for categorical variables. A multivariate regression was used to construct models for determining the fetal GA by using the fetal TCD.
Results:
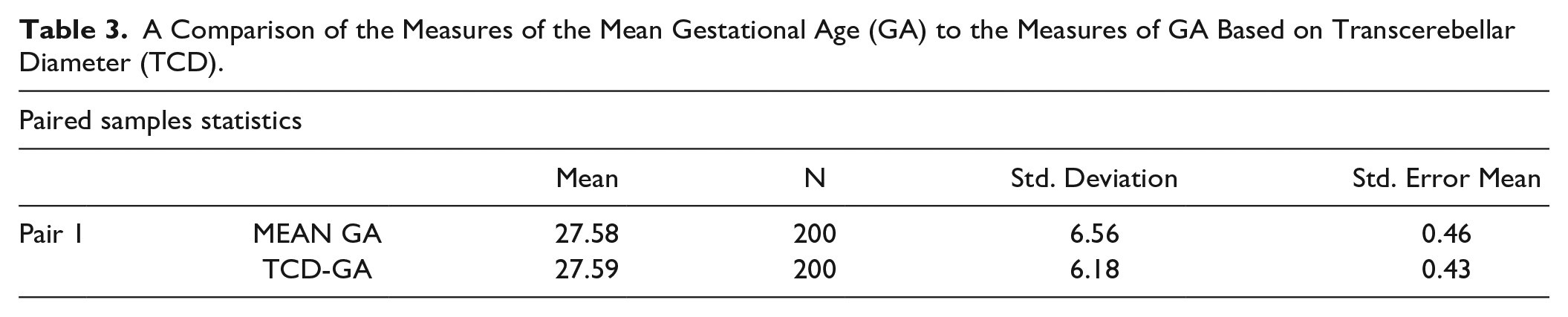
Paired sample statistics of this fetal data showed that the mean GA (i.e., fetal GA based on BPD, FL, HC, and AC) and TCD-GA have approximately the same mean values of 27.59. Moreover, the strength of correlation was 0.941 and a significance of P < .001, respectively. Based on the paired sampling, the analysis indicated that there was a very strong significant positive linear relationship between mean fetal GA and TCD-GA and strong reliability.
Conclusion:
This cohort study demonstrated a very strong significant positive linear relationship between mean fetal GA and TCD-GA, with strong reliability. This may suggest that it is possible to determine fetal GA by measuring TCD.
Keywords
The estimation of fetal gestational age (GA) serves as the cornerstone for determining the precise timing of deliveries. Erroneous GA assessments yield elevated rates of both fetal and maternal morbidity and mortality.1,2 It forms the bedrock for judiciously timed deliveries and the effective handling of potential complications, with empirical evidence substantiating the dire consequences of relying on imprecise GA assessments in terms of heightened risks to both fetal in addition, maternal health. 3 The systematic measurement of cephalic, abdominal, and femoral biometric parameters facilitated the meticulous documentation of crucial anatomical landmarks. Moreover, deviations from standard measurements could signify early indications of serious pathologies, preventing an undue influx of false-positive findings and the subsequent need for subsequent diagnostic examinations. 4
In first trimester, the crown-rump length (CRL) measurement is considered the diagnostic gold standard for GA assessment.5,6 Particular attention should be given to the precise placement of the electronic calipers, at the distinct endpoints of both the fetal crown and rump, to ensure clear and unambiguous visibility.7,8 During pregnancy, biometric measurements like the femur length (FL), biparietal diameter (BPD), and abdominal circumference (AC) are essential metrics for determining the accurate GA, after the first trimester. 9
The fetal transcerebellar diameter (TCD) is considered a highly reliable sonographic measurement, and it plays a significant role in predicting GA, during the entire pregnancy. The TCD is recognized as a distinct and independent parameter for assessing GA. 10 It closely aligns with GA in weeks and becomes particularly useful when measuring a BPD is challenging. While the cerebellum’s growth curve levels off in the third trimester, TCD remains a reliable diagnostic tool for assessing fetal development and maturity. 11 It serves as a consistent reference point for GA determination when other methods may be less reliable 12
The fetal BPD continues to serve as the reference standard by which other parameters for assessing GA are gauged. The BPD measurement is crucial for assessing fetal growth and development. 13 Measuring fetal AC involves obtaining a cross-sectional view of the abdomen where the stomach is visible, at the skin’s outer layer. 4
The growth of the femur follows a linear pattern throughout fetal development and is most reliably measured after the 14th week of gestation. Measurements are taken along the bone’s elongated axis, without considering the bone curvature. FL measurements prove to be a valuable diagnostic tool for accurately estimating GA, particularly within the gestational period of 14 weeks to full term. This measurement also aids in evaluating lower limb development and spotting potential severe skeletal issues early, which improves overall fetal assessment. 14
The TCD emerges as an exceptionally dependable indicator of GA, particularly in the third trimester of pregnancy. Its reliability can be attributed to the distinctive anatomical characteristics of the fetal cerebellar hemispheres, which are situated within the posterior cranial fossa, a region known for its resistance to external pressure and growth variations. Consequently, the relative stability and resilience of the fetal cerebellum make it an exceptional indicator for determining GA, especially in later stages of pregnancy. The reason it is so crucial, is that it is not affected by fetal conditions such as intrauterine growth restriction (IUGR). IUGR is a condition characterized by fetal growth below the expected norm, considering each infant’s unique growth potential. It has significant implications for fetal and neonatal health. 15 Even in severe conditions and growth deviations TCD seems to be maintained. That is why this fetal biometry measurement is very promising for estimating fetal GA, compared to other sonographic fetal growth measures.
Materials and Methods
The research design was a cross-sectional analytical study that lasted carried for six months. This cohort study was conducted after the approval from university’s research ethical committee (Ref #: REC-UOL-/174/M/23). A university tertiary health-care facility, in Lahore, was the site for recruiting patients within the second and third trimester of pregnancy, without fetal congenital abnormality.
The inclusion criteria for patients were to be experiencing an uncomplicated pregnancy and having no known history of congenital anomaly or fetal demise. Participants with a history of hypertension, diabetes, congenital anomaly, and fetal demise were excluded from the study. A written informed consent was obtained from 200 participants. The sonogram was performed between 14th to 38th weeks of gestation, by a sonographer with total of eight years clinical experience.
Sonographic Examination
The sonographic evaluation of the fetus was completed using the Xario Prime X (Toshiba International, Tokyo, Japan) ultrasound equipment system equipped with a 3 to 5 MHz frequency convex transducer. Regular quality control of the ultrasound equipment system and transducers, including calibration, phantom testing, performance checks, and diagnostic tests, was necessary to ensure that the system was operating at optimal performance. Quality control is crucial for ensuring the reliability and accuracy of research and clinical results, obtained with the imaging system. To examine the fetus, the participants were requested to lie down in a supine position on an examination couch, in a reclined position, with the head of the couch elevated at a 30-degree angle. A small pillow was placed under the right leg of each participant. A layer of acoustic gel was applied over the abdomen so that the ultrasound transducer could be applied for scanning the fetus. The equipment system’s depth and gain settings were adjusted to achieve acceptable sonographic images.
The obstetrical sonographic examination was done by placing transducer on the lower abdomen, superior to symphysis pubis. The transducer was slid superiorly using sweeping movements to locate the fetus. In addition, the transducer was slid superiorly, sweeping side to side up to uterine fundus. Then fetal position (e.g., cephalic or breech) and presentation were checked. After checking each fetus to assure they had normal fetal cardiac activity (FCA) and fetal movement (FM), classic biometry was completed using measures of HC, BPD, TCD, AC, and FL (See Figures 1 and 2). The HC and BPD were measured in second and third trimester while also visualizing the cavum septum pellucidum, falx cerebri, and thalami. The BPD was measured from outer to inner border, while HC was measured outer to outer border. As for the TCD measurement, the maximum transverse diameter of the fetal cerebellum was recorded. The cerebellum was measured transversely from one edge to other. The FCA was rechecked and then the AC was measured, while visualizing stomach bubble, spine, and portal sinus. The AC was measured from outer-to-outer edge. At last, FL was measured from one edge to other and all the data was recorded in a final diagnostic report.
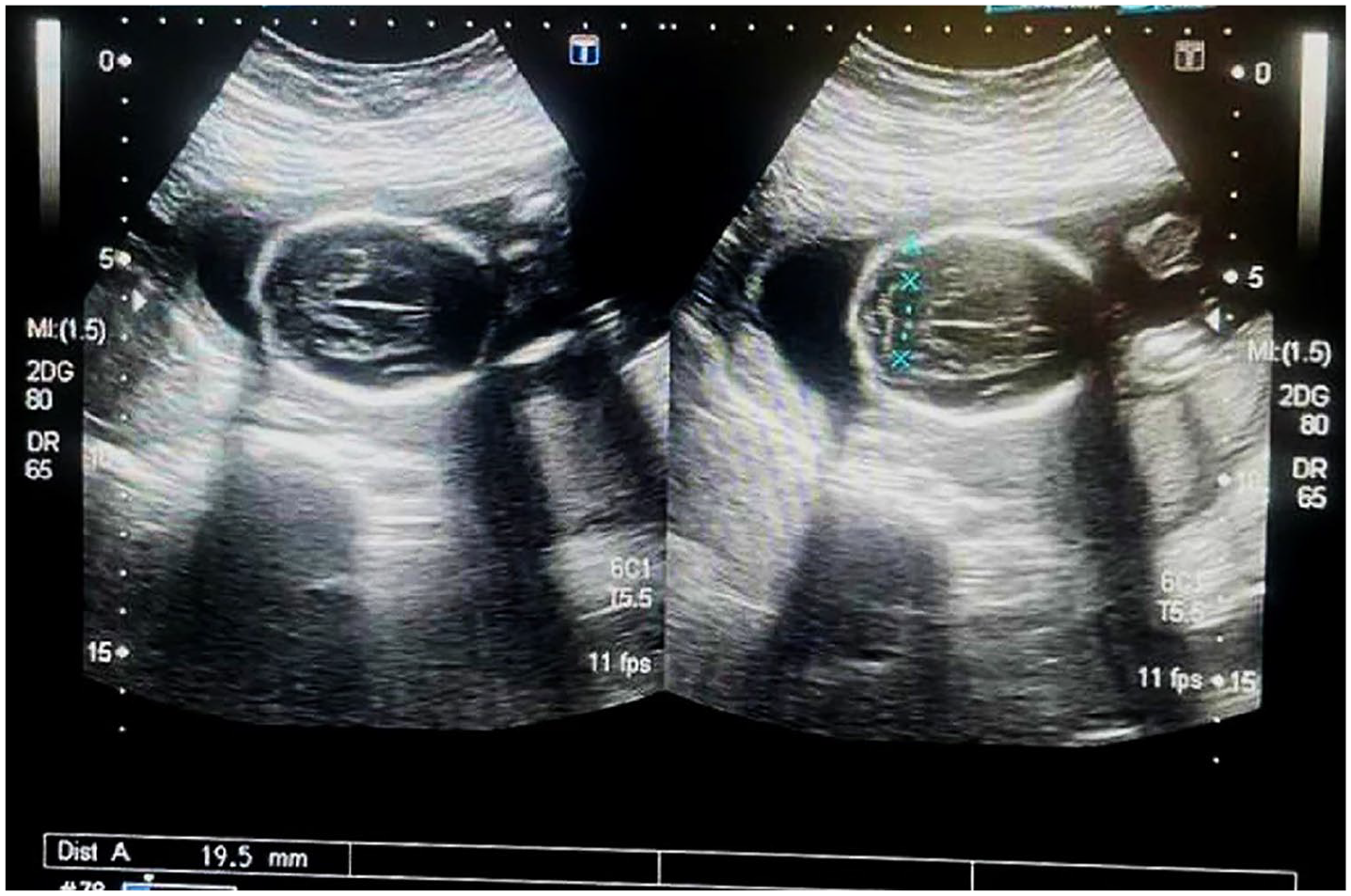
A female participant that was 33 years old reported for a sonogram and these images demonstrate the transthalamic view on the right image, to measure the BPD and the left image provides a transcerebellar view where the cerebellar diameter is 19.5 mm.
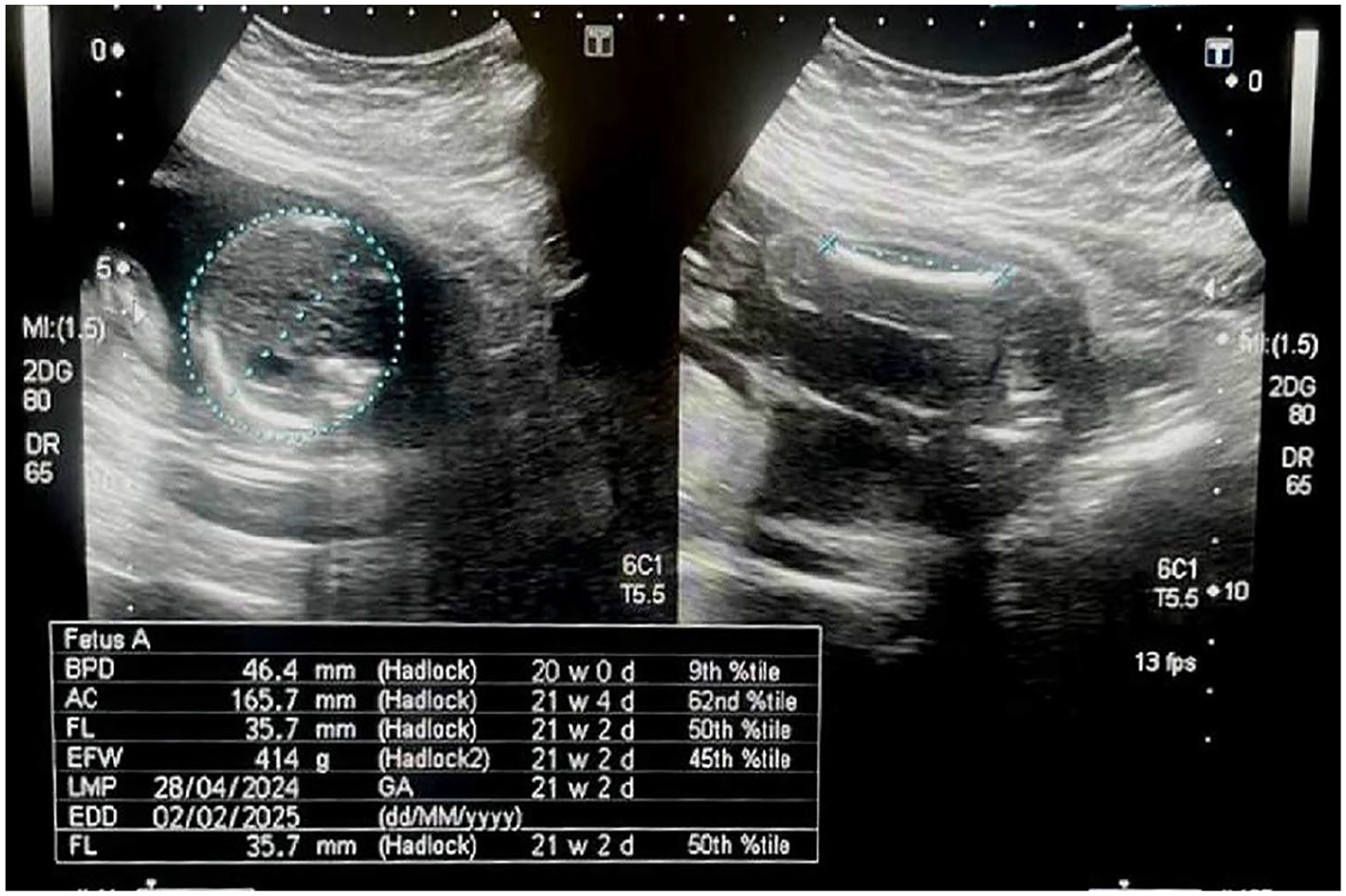
These example sonographic images are from the same participant and the right image is of the fetal abdominal circumference and left image shows the femur length that indicates an average gestational age of 21 weeks 2 days.
Statistical Analysis
Data was analyzed using the IBM SPSS Statistical software (v 25. IBM Corp., Armonk, New York) and Microsoft Excel (Microsoft Corporation, 2016). Descriptive analysis was performed and generated the mean and standard deviation to summarize quantitative continuous variables. A descriptive analysis was completed to examine the data distribution. The mean and standard deviation were provided for quantitative variables, while frequencies were determined for categorical variables. The collected data was recorded in Microsoft Excel. A regression analysis and correlations were applied. The statistical significance was set at p < .05, a priori.
Results
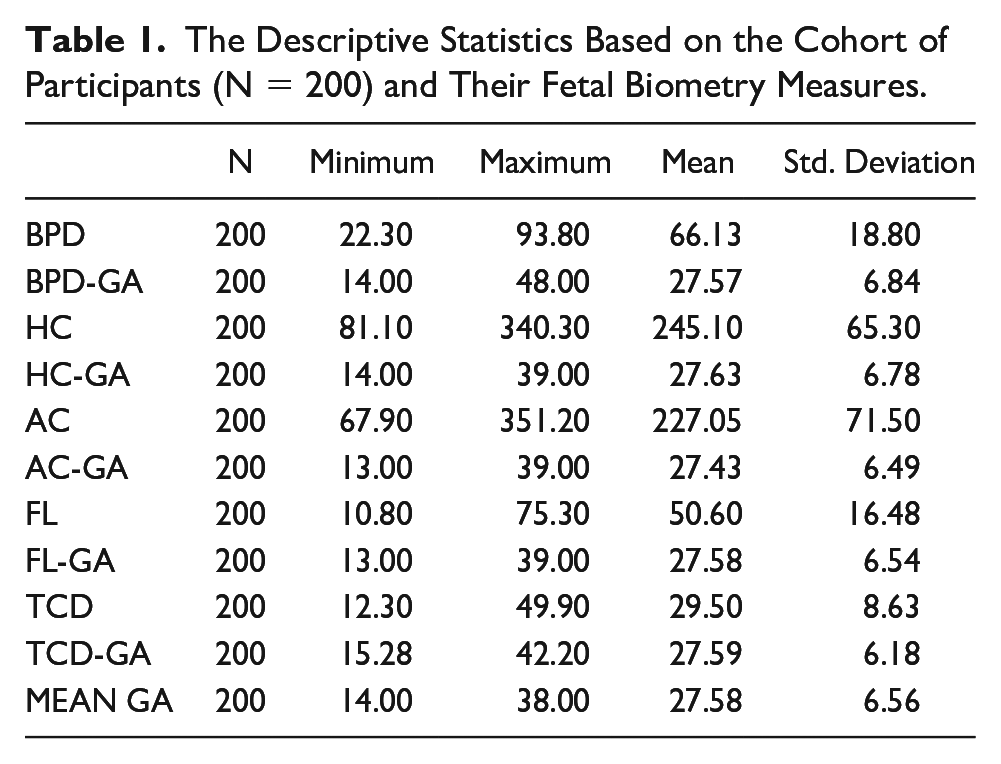
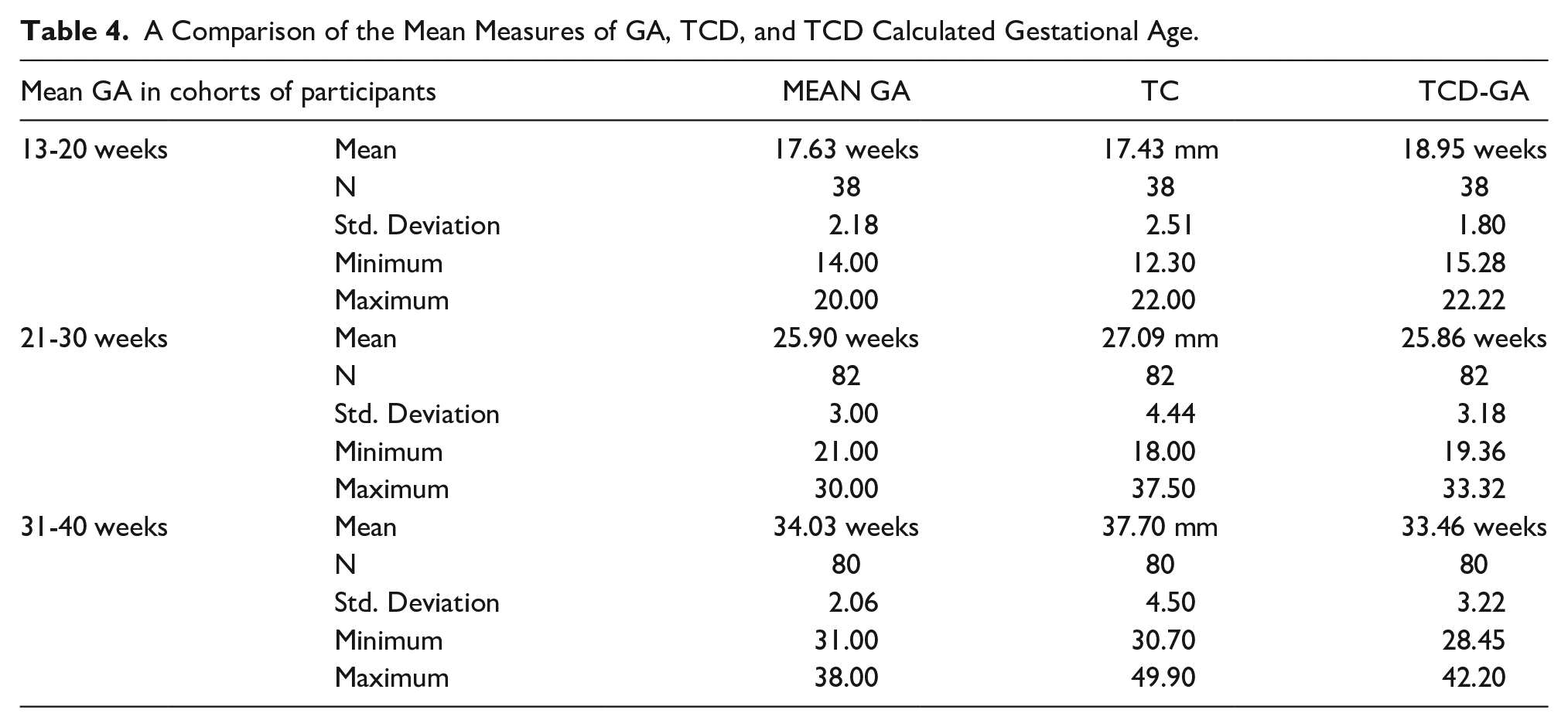
There were 200 pregnant female participants recruited and consented to this study. The mean of BPD was 66.13 mm (SD ± 18.80). The mean of BPD-GA was 27.57 weeks (SD = ±6.84). The mean of HC was 245.10 mm (SD = ±65.30). The mean of HC-GA was 27.63 weeks (SD = ±6.78). The mean AC was 227.05 mm (SD = ±71.50), with a minimum and maximum value 67.90 mm (SD = ±351.20). The mean of AC-GA was 27.43 weeks (SD = ±6.49). The mean FL was 50.60 mm (SD = ±16.48). The calculated FL-GA was 27.58 weeks (SD = ±6.54). The TCD mean was 29.50 mm (SD = ±8.63). The mean of TCD-GA was 27.59 weeks (SD = ±6.18) and a mean GA was 27.58 weeks (SD = ±6.56), with a minimum of 14 weeks to a maximum of 38 weeks (See Table 1). The TCD measure demonstrated a strong positive correlation with other biometric measurements such as BPD (See Figure 3), HC (See Figure 4), AC (See Figure 5), and FL (See Figure 6), and a mean GA (p < .01). BPD-GA showed a significant positive correlation with all the growth parameters (p < .01). HC-GA exhibited a strong positive correlation with TCD-GA, BPD-GA, AC-GA, FL-GA, and the mean GA (p < .01). AC-GA showed positive correlations with TCD-GA, BPD-GA, HC-GA, FL-GA, and mean GA (p < .01). FL-GA demonstrated substantial positive correlations with TCD-GA, BPD-GA, HC-GA, AC-GA, and mean GA (p < .01). The mean GA indicated a significant positive correlation with TCD-GA, BPD-GA, HC-GA, AC-GA, and FL-GA (p < .01) (See Table 2). Paired samples statistics showed that the mean GA and TCD-GA had approximately the same mean values of 27.59 weeks (See Table 3). In the 13- to 20-week participant cohort, the mean GA was 17.63 weeks (SD± 2.18), with a minimum GA of 14 weeks and a maximum of 20 weeks. In the 21- to 30-week participant cohort, the mean GA increased to 25.9 weeks (SD = ±3.00), with a minimum GA of 21 weeks and a maximum of 30 weeks. Finally, in the 31- to 40-week participant cohort, the mean GA further increased to 34.03 weeks (SD = ±2.06), with a minimum GA of 31 weeks and a maximum of 38 weeks (See Table 4).
The Descriptive Statistics Based on the Cohort of Participants (N = 200) and Their Fetal Biometry Measures.
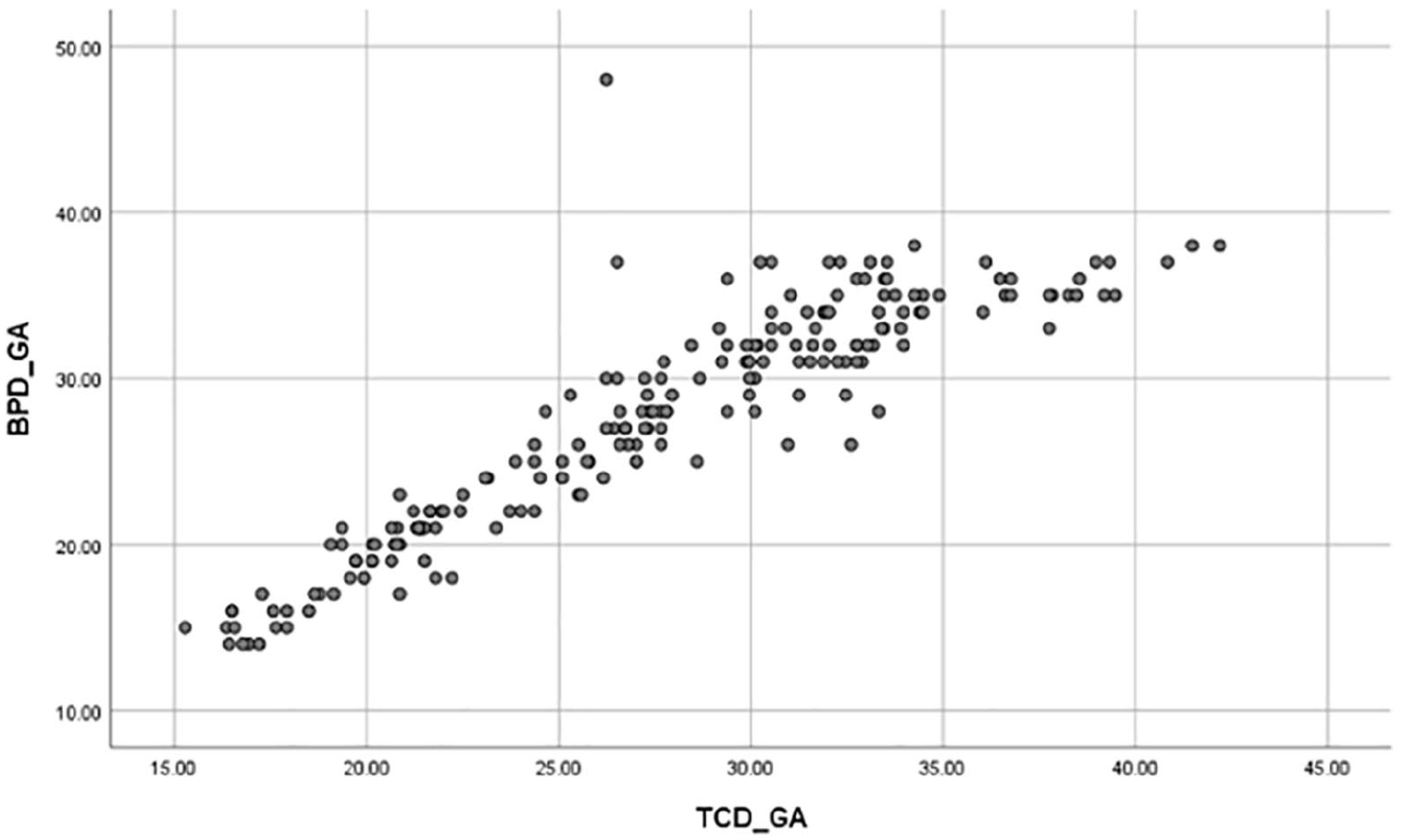
A scatter plot between TCD-GA and BPD-GA. The graph shows a significant correlation between transcerebellar diameter, gestational age, and biparietal diameter’s calculated gestational age.
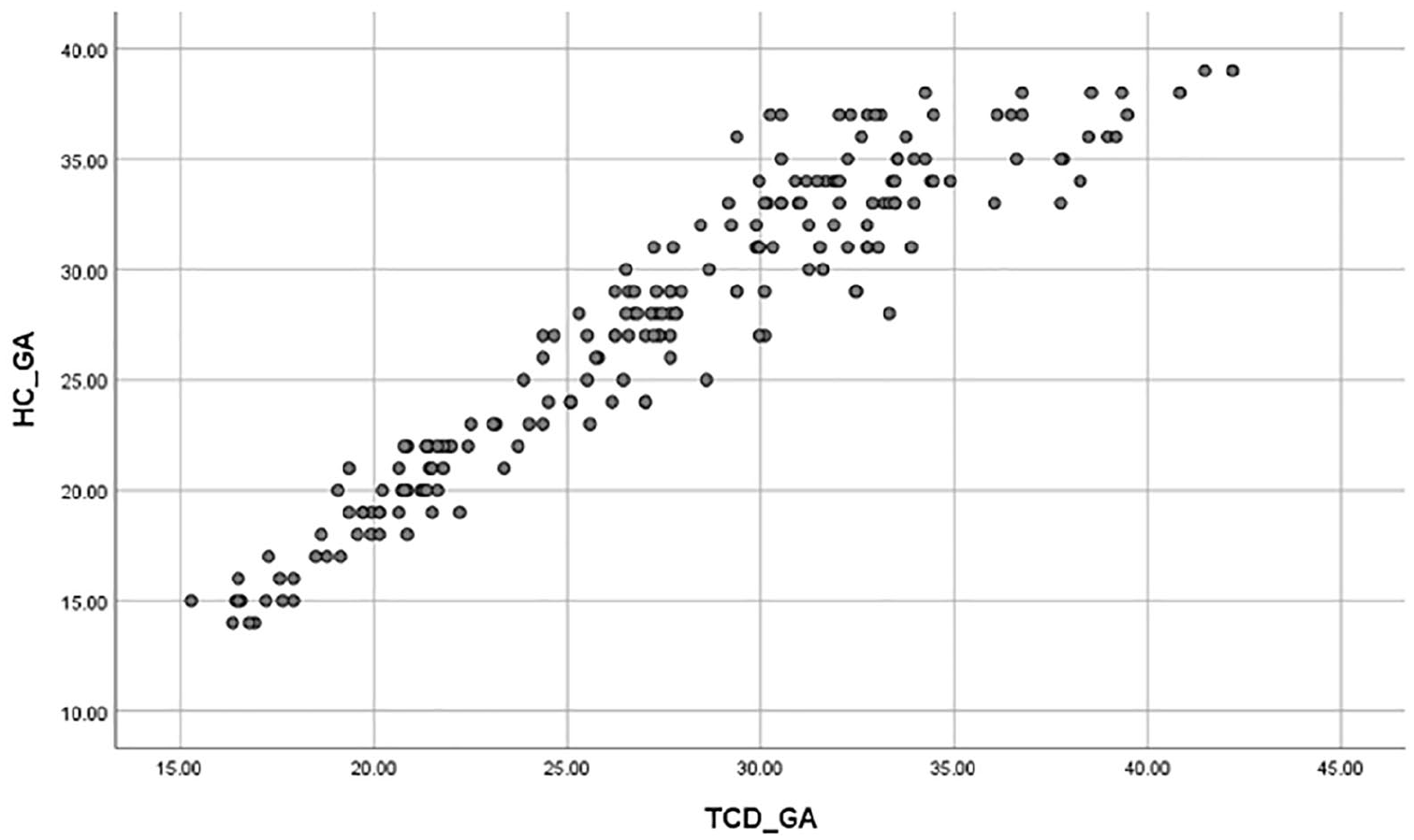
A scatter plot between TCD- GA and HC-GA. The graph shows a significant correlation between transcerebellar diameter, gestational age, and head circumference’s calculated gestational age.
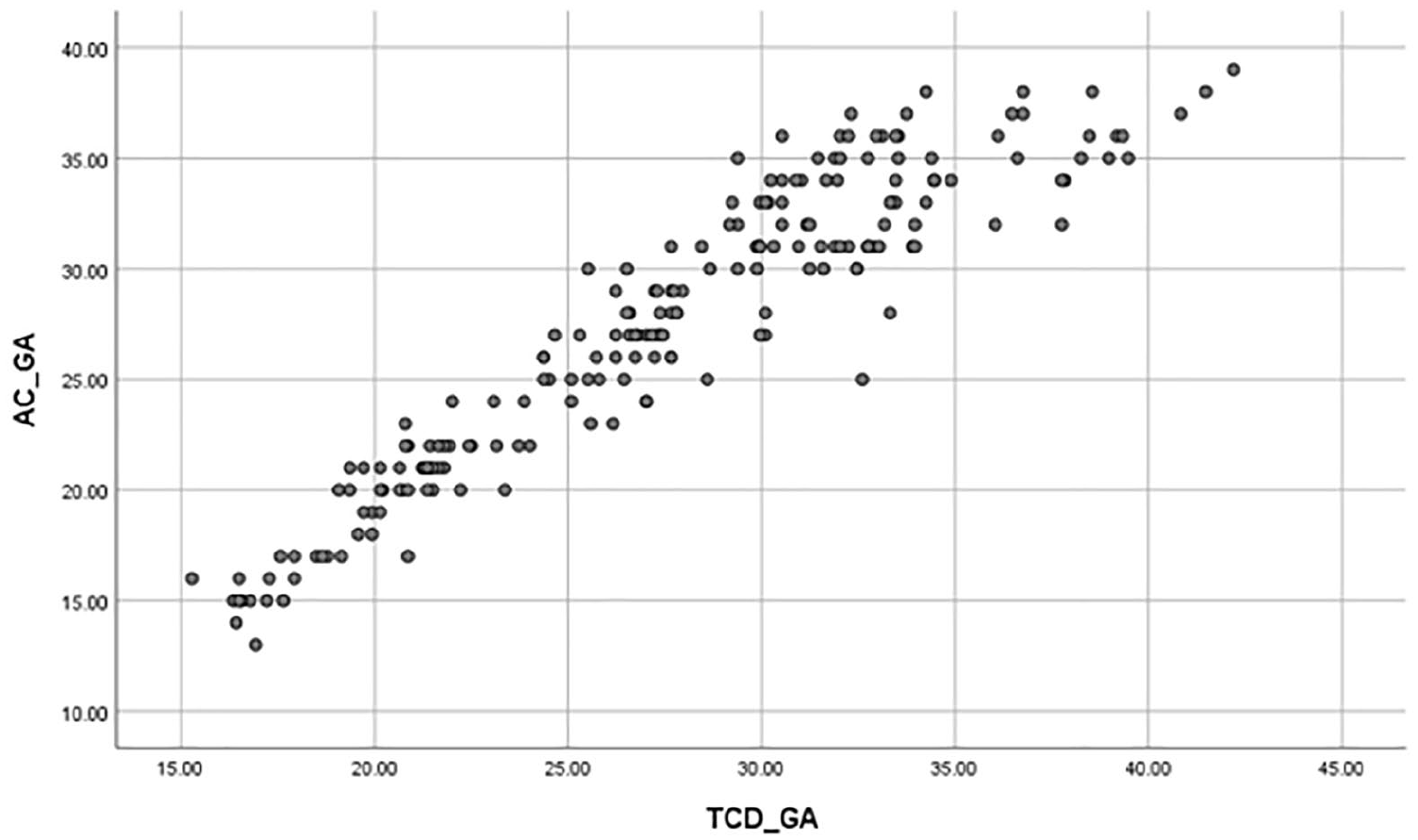
A scatter plot between TCD-GA and AC-GA. The graph shows a significant correlation between transcerebellar diameter, gestational age, and abdominal circumference’s calculated gestational age.
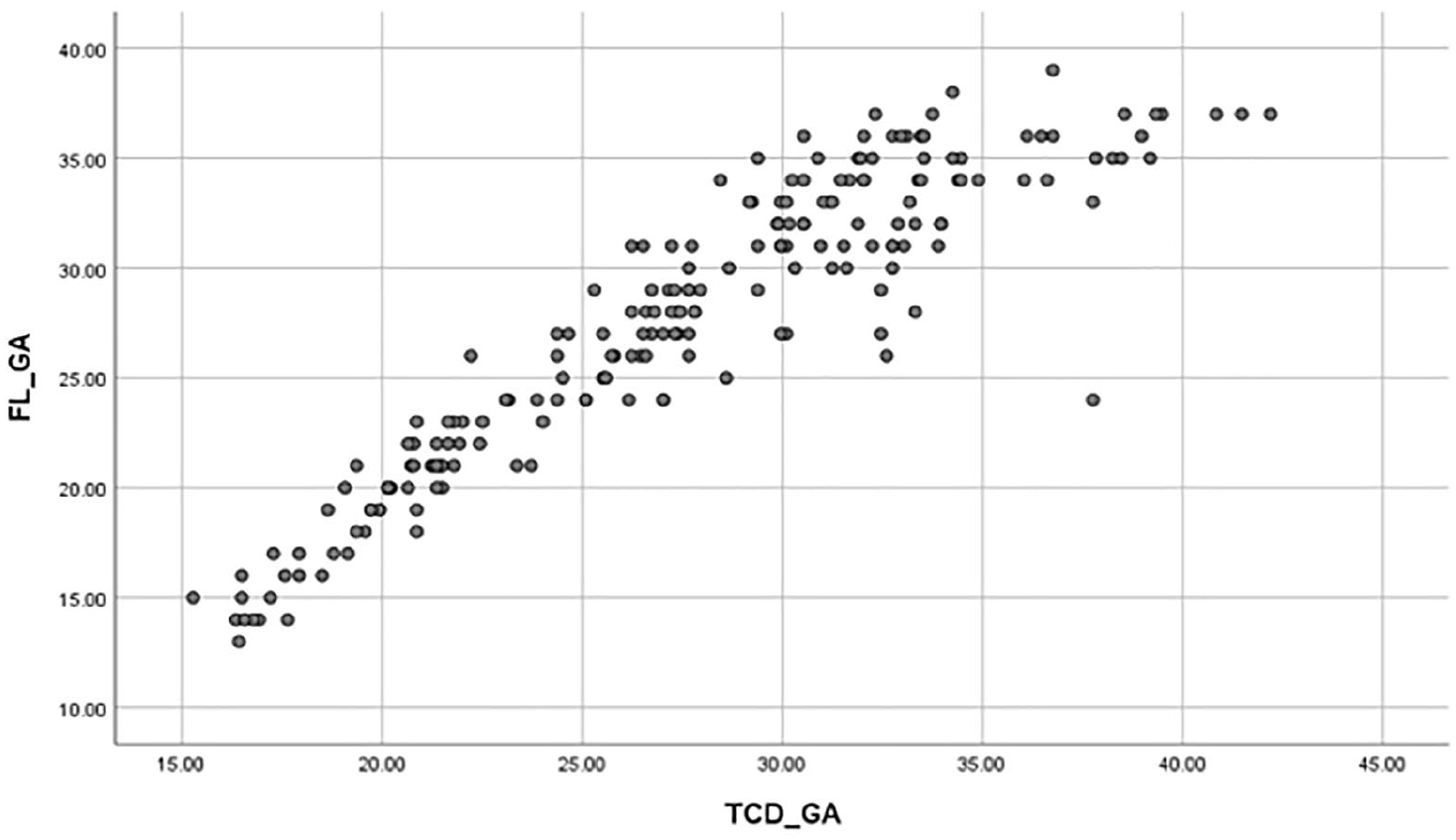
A scatter plot between TCD-GA and FL-GA. The graph shows a significant correlation between transcerebellar diameter, gestational age, and femur length’s calculated gestational age.
The Strength of Correlation and Statistical Significance for the Cohort’s Transcerebellar Estimated Gestational Ages Compared to Other Fetal Biometry Measures.
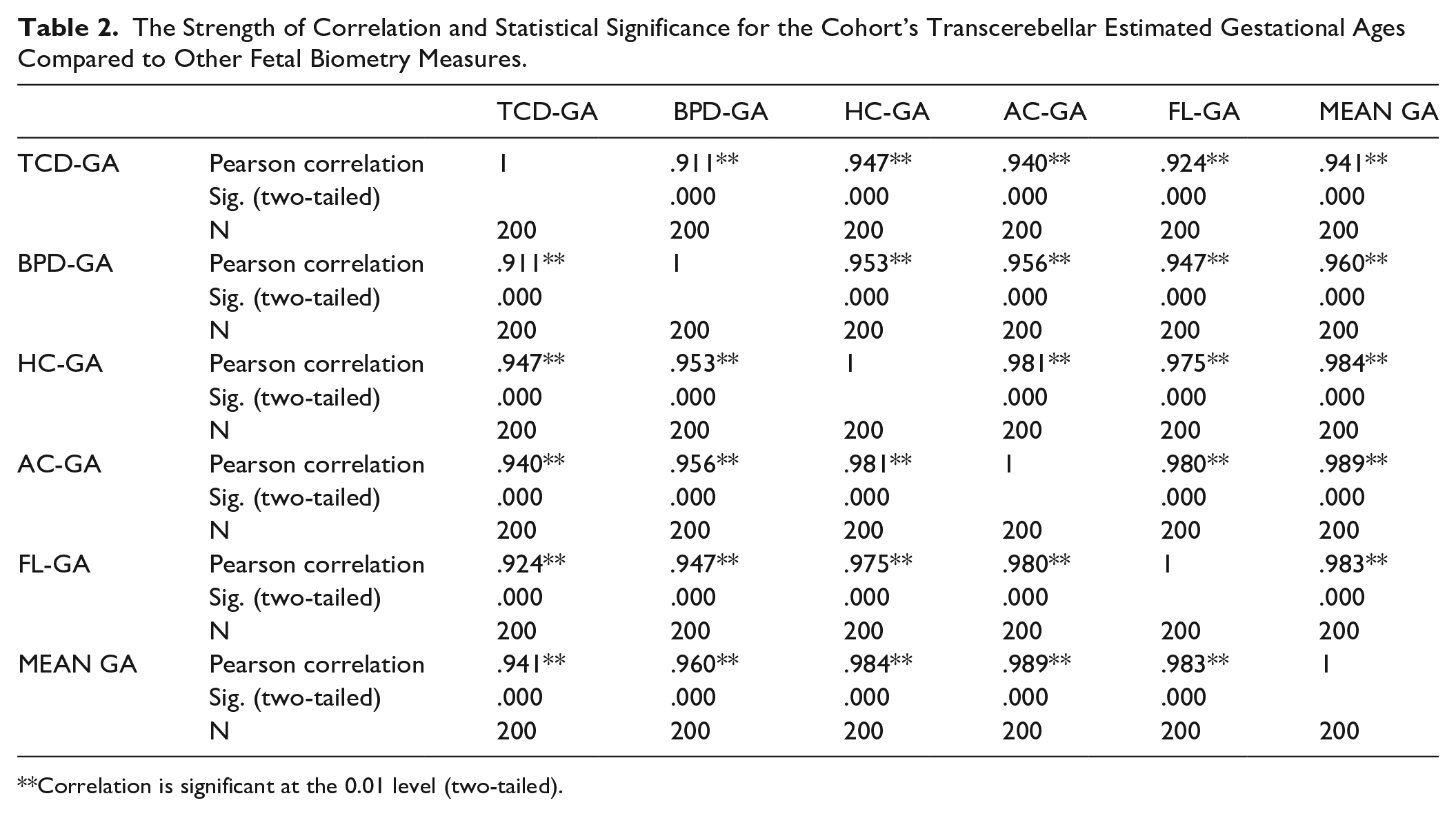
Correlation is significant at the 0.01 level (two-tailed).
A Comparison of the Measures of the Mean Gestational Age (GA) to the Measures of GA Based on Transcerebellar Diameter (TCD).
A Comparison of the Mean Measures of GA, TCD, and TCD Calculated Gestational Age.
Discussion
Many women have no access to routine prenatal care in developing countries. As a result, numerous pregnant women report to hospitals, during their second and third trimester of pregnancy, without a complete medical record allowing for their GA to be confirmed. To allow for proper pregnancy treatment, physicians must work from the best estimate of the correct GA, in these women. When women are unsure about their menstrual history, a sonographic assessment may be the only diagnostic method that can be used to evaluate GA. However, it has been noted that differences of up to three weeks might be noted when calculating GA, in the second and third trimester, when using sonographic measures, such as HC, AC, or BPD. 16
The ratio of TCD to AC is a useful diagnostic tool, in prenatal sonography, for assessing fetal growth. When this ratio is increased, it can be a helpful indicator for predicting IUGR. 17 The TCD measurement has emerged as a valuable diagnostic parameter for estimating GA, during pregnancy. Bekele et al. related TCD significance in dating the pregnancy and suggested that Bland Altman analysis is superior to correlation or regression statistical tests, when comparing the value of one variable, measured by two different methods. 11 Studies conducted in recent years have consistently demonstrated the accuracy and reliability of TCD in predicting GA, particularly in the third trimester.3,9,18,19 The current study also demonstrated a strong positive correlation of TCD with other biometric measurements such as BPD, HC, AD, FL, and mean GA (P < .01). Based on local study involving 135 pregnant women, with uncomplicated pregnancies, they established that TCD could accurately estimate GA, either independently or in conjunction with other factors. 20 In addition, there was a suggestion that incorporating the TCD/AC ratio could further enhance the precision of GA assessment using sonography. 20 In research conducted by Mishra et al., they observed a maximum measurement of TCD at 47.4 mm. This measurement closely approximates the highest reported TCD value of 48.4 mm documented in study by Prabhat et al. 21 In addition, investigations involving diverse groups of pregnant participants have consistently shown that TCD serves as a dependable marker for estimating GA, reaffirming its diagnostic value in clinical practice. In the current study, paired samples statistics showed that the mean GA and TCD-GA had almost the same mean values of approximately 27.59 weeks. This correlation is especially significant in the later stages of pregnancy, where accurate GA estimation is crucial for monitoring fetal growth and ensuring optimal prenatal care. TCD has been shown to be more accurate than other biometric measurements, such as BPD, in estimating GA, during the second and third trimester. 22 Consistent with this sample of previous studies, the current study found that TCD was a more accurate method for estimating GA, compared to other the other classic sonographic biometry measurements.
Limitations
This cohort study has specific limitations related to the study design, which was pre-experimental and the sample of participants that were by clinical convenience. These pose significant threats to internal and external validity and make these results only applicable to those participants of this study. In addition, these sonographic GA measurements were completed on a cohort of participants from this specific part of the globe and may have unique cultural, ethnic, and environmental factors that make their fetal development unique. Although this work is limited, it does suggest the diagnostic value of TCD and how it might be further explored in a variety of populations for refining GA accuracy.
Conclusion
The current study concluded that TCD, in this cohort of participants, seemed to be a reliable single biometric sonographic measurement for estimating GA, in second and third trimester. This may be especially helpful in those patients who are unable to report their last mensural period and subsequently have an unknown gestational age. This cohort’s results are very comparable to previous studies that investigated the diagnostic value of TCD.
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the university’s research ethical committee (Ref #: REC-UOL-/174/M/23).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.