
Abstract
Objective:
The aim of this study was to explore and understand sonographers’ occupational burnout experience and develop a curriculum for an intervention program, to mitigate this type of distress.
Materials and Methods:
A convergent parallel mixed-method design was employed to better understand sonographers’ experience of occupational burnout and develop a curriculum for an intervention program that targets specific needs of sonographers. The quantitative data were collected via an online survey, which included demographic questions, ranking factors that contribute to burnout on a 5-point Likert scale, and prevalence and feelings around conflict at work. Simultaneously, qualitative data were gathered through semistructured interviews conducted remotely with eight sonographers.
Results:
A total of 104 sonographers responded to the survey and eight sonographers participated in the online interview. Most of the participants were females (83.5%), working full-time (88.5%). Among this cohort, 60.6% self-reported experiencing burnout. In both qualitative and quantitative data, the experience of conflict at work was reported as stress or anxiety provoking. Stress management and conflict resolution were the most rated topics that participants wanted to be included in the intervention program. A total of 46.1% respondents from the survey reported being interested in participating in such a program.
Conclusion:
This study explored sonographers’ occupational burnout experience to develop a curriculum for an intervention program, tailored to their needs. The study findings indicated that this cohort of sonographers were aware of burnout and open to participating in an intervention program. Based on the results of this study, a group therapy curriculum was developed to help sonographers deal with conflict at work, managing stress, and mitigating occupational burnout.
Occupational burnout is defined as a long-term response to prolonged stress on the job. 1 It consists of emotional exhaustion, detachment, and/or depersonalization from the job combined with a lack of accomplishment, due to the continued conditions of work-related stress. 1 Previous research has shown that sonographers are experiencing moderate to high work-related burnout.2 –6 Some risk factors and potential causes of sonographer’s occupational burnout have been linked to increased workload, working overtime, patient encounters, work-related musculoskeletal disorders, and lack of administrative support.3 –9 During the COVID-19 pandemic, there was an increase in sonography requests for patients with possible severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral infection, which further increased the workload and stress for sonographers.10 –12 Evans et al 7 explored the downstream effects of the COVID-19 pandemic on sonographers and vascular technologists. A total of 1389 sonography users participated in this study, 48% of which reported higher workload, and 39% indicated considering retirement or changing jobs. A key finding reported in this study was the lack of support from supervisors and hospital administration, which has been supported by a similar study 8 where lower supervisor support and job satisfaction were associated with higher work-related burnout. In a Nigerian study, high levels of occupational burnout were reported among 50 sonographers. 2 The main identified factors that contributed to their burnout were high workload and inability to cope with hostile interactions between patients, colleagues, and supervisors. Among this cohort of sonographers, 5% reported conflict with their supervisors. 2
Despite this prevalence of occupational burnout alongside the lack of supervisors’ support and the impact it has on the individual and organizational level, there is a lack of published data on intervention programs to specifically address sonographers’ occupational burnout. However, in more recent research, Callpani et al 13 and Walsh 14 have pointed toward program interventions, as the next necessary step. Regarding such programs, some studies have shown that mindfulness training can help with stress and burnout.15,16 Mann A et al 17 studied the effects of a coaching program on occupational burnout among 1017 female physician trainees. This web-based group coaching program “Better Together” provided by a coach-certified physician for 4 months, showed a significant decrease in all subscales of burnout measured with the Maslach Burnout Inventory tool. Another finding was improved self-compassion compared with the control group of physicians. Considering these reported effective intervention program outcomes, this study was designed to explore sonographers’ experience of occupational burnout and develop a curriculum, for an intervention program, tailored to their needs. An additional aim was to assess whether sonographers were interested in participating in an intervention program, given the resistance that may exist for mental health and psychological well-being. Such resistance was shown in the study conducted by Callpani et al. 13 In that study, they used the Oldenburg Burnout Inventory, a validated tool to assess postpandemic work-related burnout in sonographers in New York City. They found that among 70 sonographers, 81.4% were experiencing moderate to high occupational burnout. Yet only 5% of participants reported seeking professional psychological help.
To develop a curriculum, as a basis for an intervention program, the study was focused on several goals: (1) identifying factors that contribute to occupational burnout, (2) assessing the prevalence of conflict at work and its impact on sonographers, (c) assessing if sonographers are open to participating in an intervention program, and (d) getting sonographers’ input regarding topics they would like to be included in such a program.
Materials and Methods
This was a descriptive and exploratory cross-sectional study, designed to assess key themes that may contribute to occupational burnout among a cohort of sonographers, working in New York City. A convergent parallel mixed-method component design was used to understand in more depth their occupational burnout experience, factors that contribute to their burnout, occupational burnout symptoms, and potential interventions. An Institutional Review Board approval was obtained through the State University of New York (SUNY) Downstate Health Sciences University (IRB# 2118185-1). The e-mail addresses of sonographers, working at various clinical sites and sonography specialties, in the New York City metropolitan area, were obtained. The survey was distributed electronically based on an e-mail list of 400 sonographers. A brief introduction to the study and its purpose was included in the first e-mail, alongside the link to the survey and instructions to reply, if they were also interested in participating in a remote interview. A separate follow-up e-mail that contained a Zoom link and details about the interview process, was sent to those who responded to the initial e-mail. When sonographers accessed the Zoom link, it constituted a consent to participate. It was stressed that participation in the study was voluntary.
The quantitative data were collected using an online survey developed with Qualtrics software (Qualtrics, Provo, UT). The survey consisted of 13 questions which included demographic characteristics such as age, gender, type of employment (full-time, part-time, per diem, travel sonographer), number of years in sonography, work shifts (daytime, nighttime, evenings); ranking factors that contribute to occupational burnout on a 5-point Likert scale, and prevalence and feelings around conflict at work. Multiple choice questions were asked to gather participant’s opinions on topics they would like included in an intervention program. It was also a means to gauge whether they would be open to participating in such a program. A free-text open-ended question regarding the manifestation and their experience of occupational burnout was provided. The intent was to gather insights into participants’ awareness of burnout and its manifestation in the body, mind, and effects on their day-to- day life. The term burnout was not defined to avoid bias in the participants’ response regarding manifestations of occupational burnout.
The qualitative portion of the research included a 35- to 40-minute remote interview with participants. A semistructured interview script (See Appendix A—QR code) was designed to explore the sonographers’ experience of occupational burnout and capture nuances and depth that could better inform and help those developing training and/or program interventions that target specific symptoms and factors that contribute to occupational burnout.
Participant Interviews
The interview questions were created by the researcher, a registered sonographer with years of experience in private and hospital settings, who was also a trained mental health counselor from New York University. Following Morrow’s 18 conceptual foundation of qualitative research in counseling psychology, the semistructured interview was designed to explore the lived experience of sonographers’ occupational burnout and used language as a tool to capture the depths, nuances, and the insights of sonographers regarding potential solutions. It also identified some protective factors that could be used when designing program interventions or preventions. The researcher conducted the interviews with an attitude of warmth and empathy. Summarizing was used as a technique to reflect the main points and let the participant correct and clarify, if the summary felt inaccurate.
The qualitative data, gathered from semistructured interview, was inductively analyzed using a well-established six-stage approach. 19 The six-stage process included: becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, define themes, and write-up. 19 An analytic memo was written after each interview. Participants were involved in reviewing the qualitative data to get feedback about the accuracy of the researchers’ interpretation and findings. Both data sets were analyzed separately using descriptive statistics for quantitative data and thematic analysis for qualitative data. Findings were then integrated by comparing themes from qualitative data with patterns identified in the quantitative data, allowing for a richer understanding of sonographers’ occupational burnout and development of a curriculum, tailored to their needs.
Results
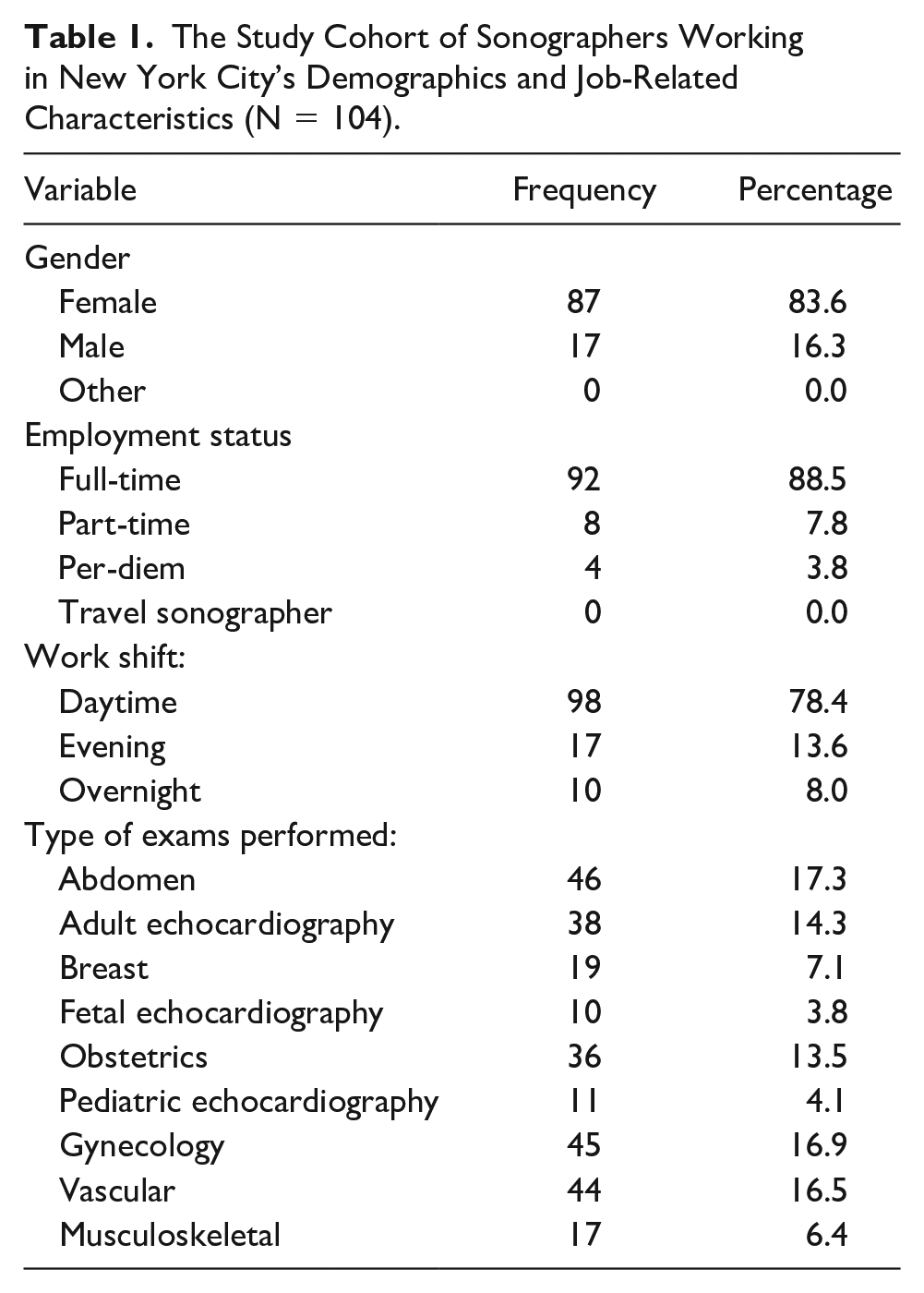
One hundred and twenty-four sonographers participated in the survey; however, 20 participants were excluded as they did not fully complete the survey. The total sample of analysis was 104 survey responses corresponding to a 26% response rate. Demographic characteristics from the survey are reported in Table 1. There were 92 participants who reported a mean age of 44.7. One hundred and two participants reported their years of experience with a mean score of 15.7. Most of the participants were females (83.6%), working full-time (88.5%) with a day-time shift (78.4%) and performing multiple different types of sonographic exams, during their shifts. In the survey, participants were allowed to select all the answers that apply regarding work shift and the type of exam.
The Study Cohort of Sonographers Working in New York City’s Demographics and Job-Related Characteristics (N = 104).
In this cohort of sonographers, when asked if they ever experienced burnout, most of the respondents agreed (60.6%) (See Figure 1). Fifty-nine participants provided free-text comments, regarding their personal experience and manifestation of occupational burnout. These comments were organized in three categories (See Table 2). Although the term burnout was not defined for participants, these comments speak to participants’ awareness of work-related burnout and their ability to recognize the signs and symptoms, as their description of how burnout manifest for them, is like what has been reported in the literature. 1
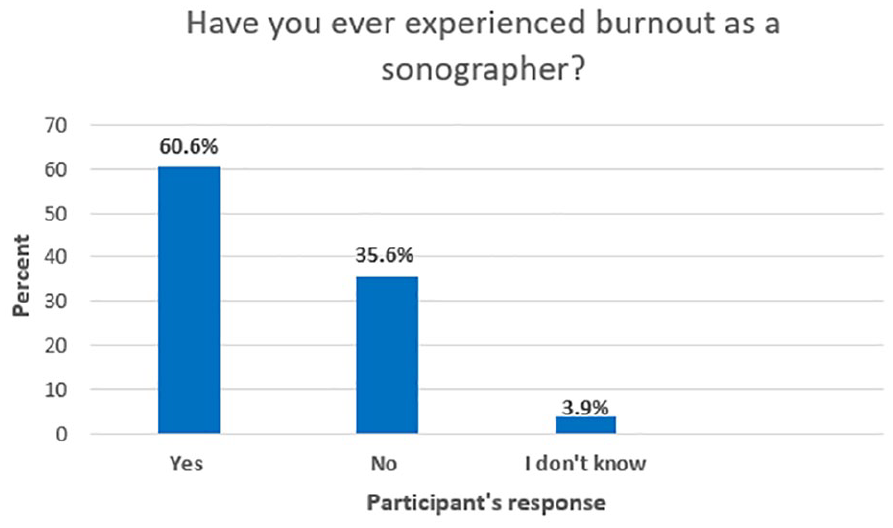
A bar chart of participants’ self-reported occupational burnout, as recorded in the survey (N = 104).
A Sample of a Participant’s Comments From the Survey to the Free-Text, Open-Ended Question Describing How They Experience Occupational Burnout.

Abbreviations: P, physical; E, emotional; PE, physical and emotional.
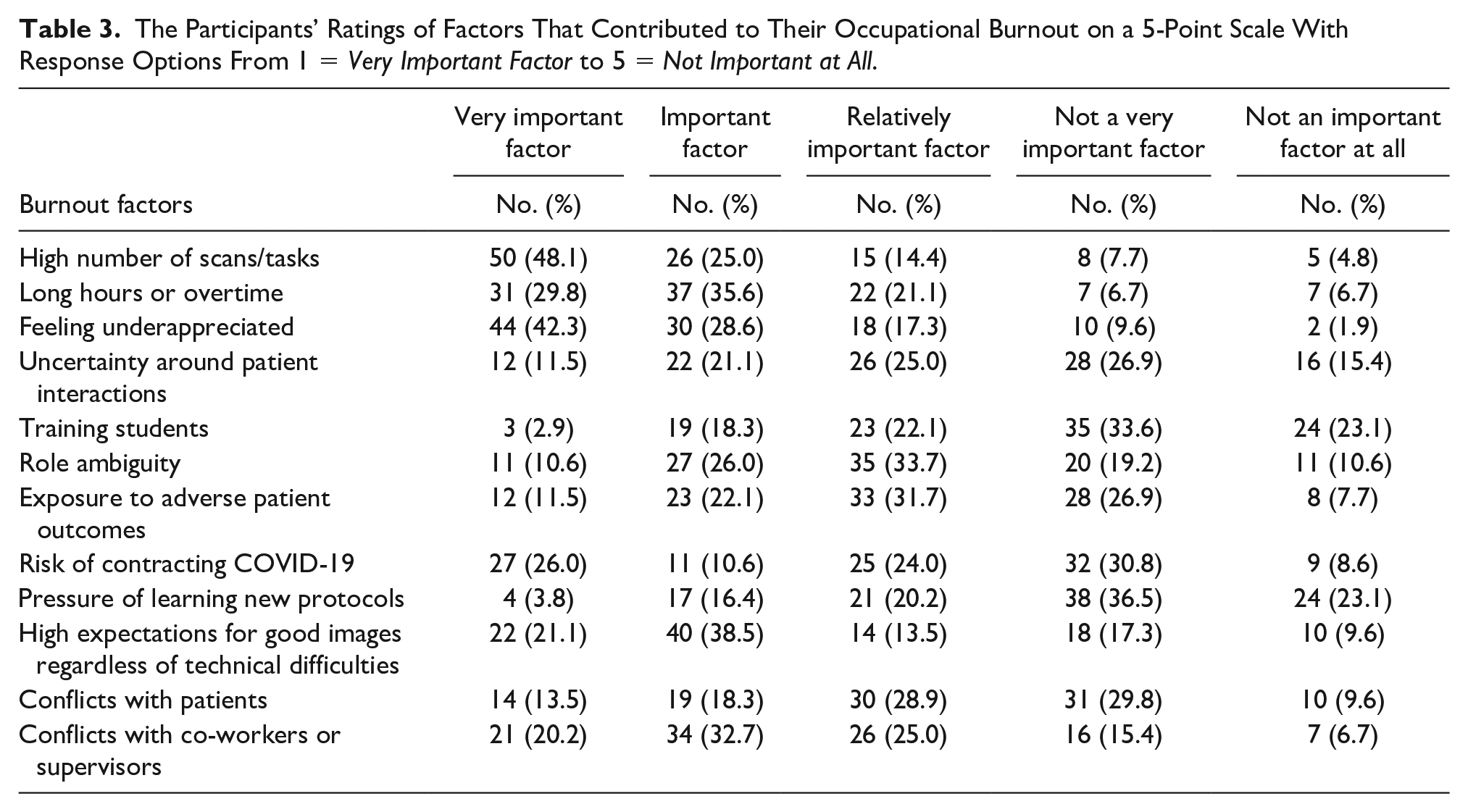
Participant ratings of the most important factors that contribute to occupational burnout are reported in Table 3. The high number of sonograms and feeling underappreciated were reported, as the most important factors contributing to their occupational burnout. In this cohort, 73.1% (N = 76) rated the increased number of sonograms as a very important or important factor. Likewise, in this cohort, 71.1% (N = 74) rated feeling underappreciated, as a very important or important contributing factor. The introduction of conflict, as a possible factor contributing to occupational burnout, was rated by 52.9% (N = 55) of participants that the conflict between co-workers or supervisors was a very important factor or important factor. This was also supported by the qualitative data from the interview. The prevalence of conflicts at work is provided in Table 4. Conflicts with management and patients are reported as more prevalent compared to conflicts with other sonographers or physicians, with 35.6% reporting experiencing conflict with management sometimes, or often. Regarding conflicts with patients, 30.8% reported experiencing conflict sometimes, and 5.8% reported experiencing conflict often. When asked to rate their anxiety when in conflict at work on a 5-point scale with response options from 1 = very likely to 5 = very unlikely, a total of 72.1% were either very likely or likely to experience feelings of anxiety during conflict at work (See Figure 2). The participant’s multiple-choice answers regarding the topics they would like to be included in the intervention program are shown in Figure 3. These topics were not defined for participants in this cohort. Stress management (36.2%) and conflict resolution (26.2%) were the most rated topics. When asked if they would be interested in participating in an intervention program that helps mitigate occupational burnout, 46.1% answered yes and 30.8% answered unsure.
The Participants’ Ratings of Factors That Contributed to Their Occupational Burnout on a 5-Point Scale With Response Options From 1 = Very Important Factor to 5 = Not Important at All.
The Participants Provided Their Survey Responses to How Often They Have Conflict at Work With Management, Other Sonographers, Physicians, or Patients.
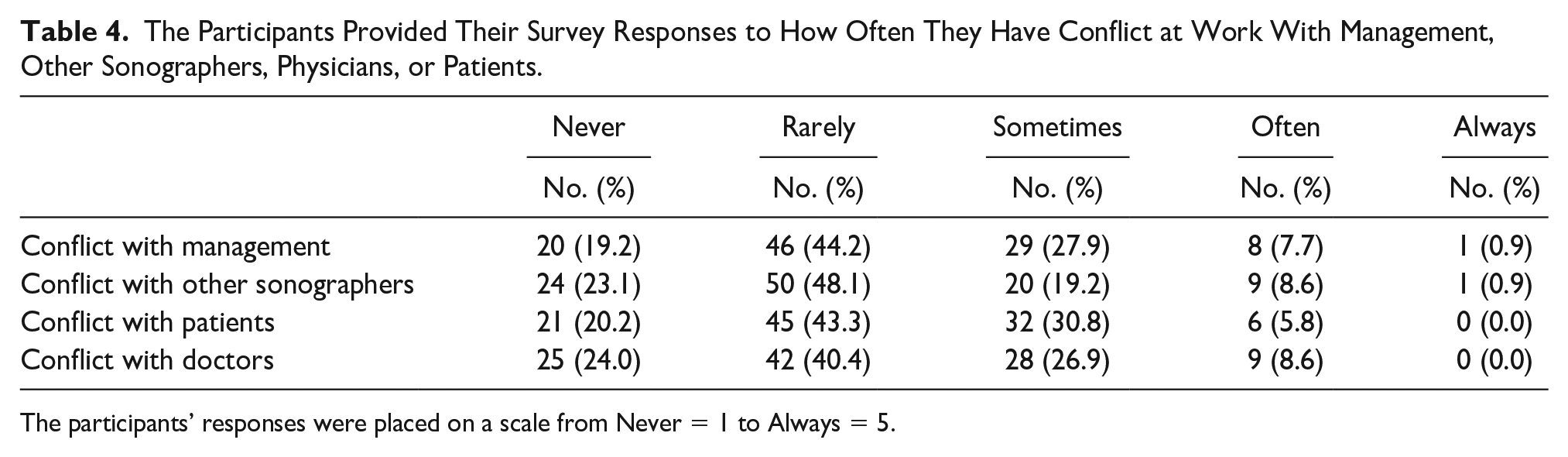
The participants’ responses were placed on a scale from Never = 1 to Always = 5.
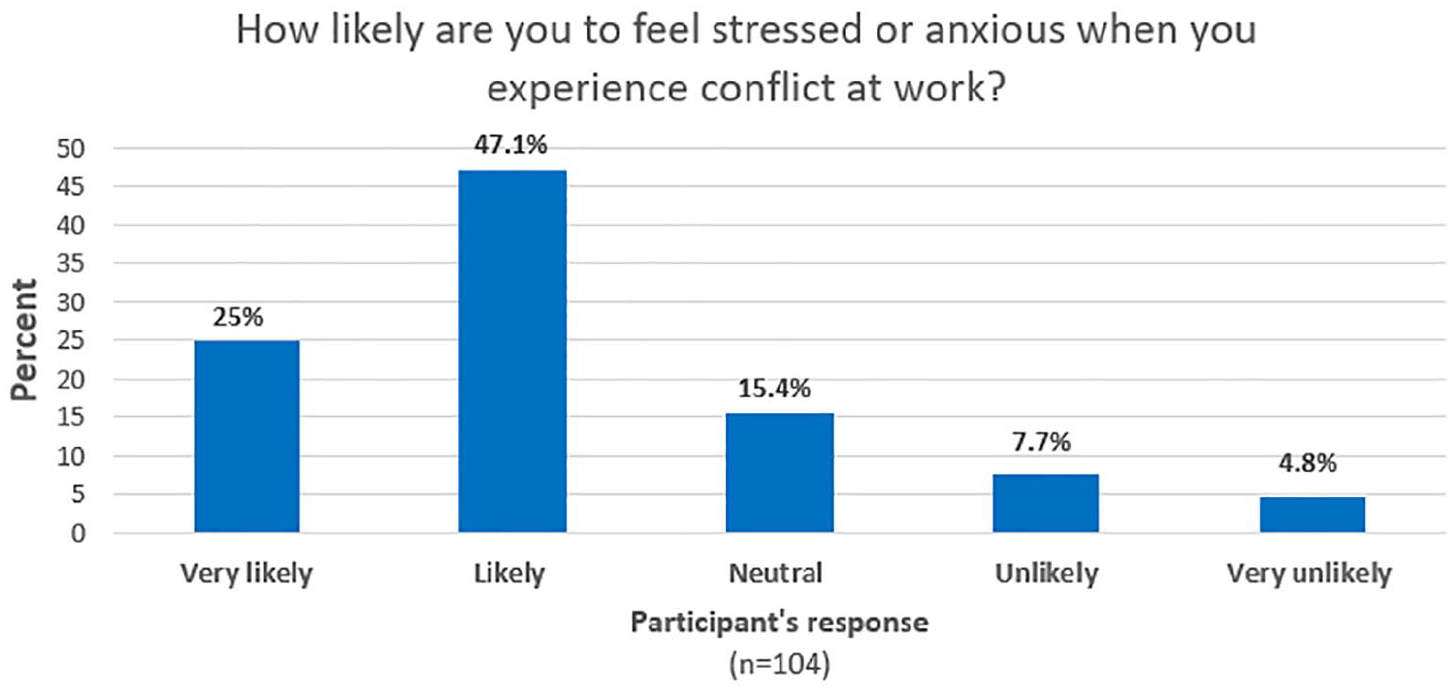
This bar chart represents participants’ survey response to how likely they are to feel stressed or anxious, when dealing with conflict at work.
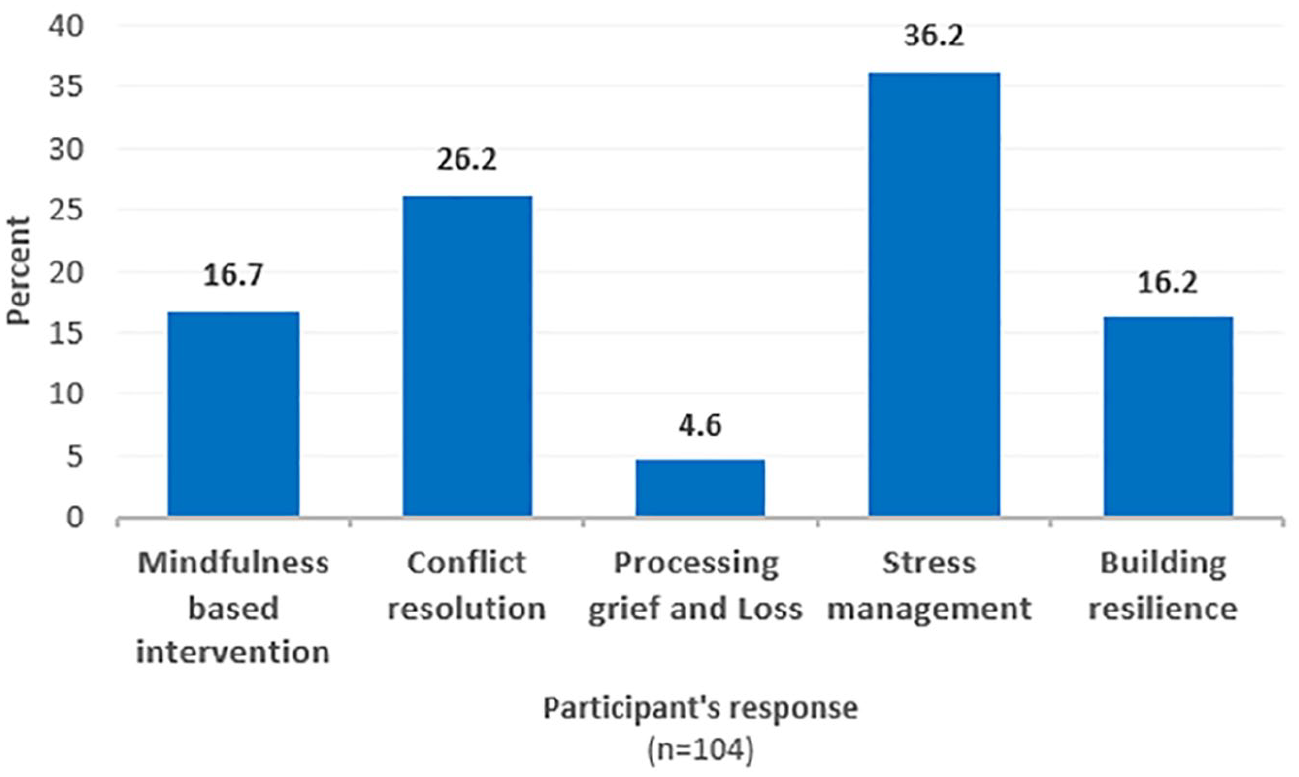
This bar charts represent participants’ selection of up to three topics they would like to be included in an intervention program.
Participant Interviews
Eight sonographers responded to the initial recruiting e-mail expressing their interest in participating in the interview portion of the study. From these participants, three were male sonographers and five were female sonographers. Based on their responses, the data were coded. A sample of thematic analysis coding is provided in Table 5. A summary of the qualitative themes that emerged through the thematic analysis and subcategories are provided.
A Sample of the Coding Applied to a Participant’s Interviews, Using Thematic Analysis.

Theme #1: Source of occupational burnout
Some of the sources of occupational burnout identified from the interviews were the following: a lack of administrative support, a lack of autonomy, workload, pressure to quickly complete sonograms, the high expectation for sonographic quality, regardless of exam limitations. The cohort also listed poor leadership, working alone during overnight shifts, conflicts with the team (e.g. nurses, physicians, etc.), conflicts with patients, dealing with patient’s encounter, unable to say “no” to the supervisors. They also talked about the inability to practice good ergonomics, due to the pressure to complete as many sonograms quickly, doing a lot of bedside portable sonograms and complex exams, such as transplanted organs and duplex Doppler studies.
While links between conflict and occupational burnout have been explored and published in the literature,20,21 there is a lack of evidence that such a link exists, specific to sonographers. Thus, questions around conflict such as prevalence and feelings were included in the survey and the interview script. Some female participants told of crying and feeling “terrible” after having a conflict with a patient, versus one male sonographer stopped the exam and told the patient they were being abusive.
Theme #2: Manifestation of occupational burnout
The interview participants were aware of their level of occupational burnout. Only one out of eight participants reported not having experienced burnout, and another participant was not sure or aware of experiencing it. Some common ways that occupational burnout affected participants’ well-being were physical exhaustion, pain in arms, neck, and shoulders, mental exhaustion, fear of losing connections with patients, feelings of resentment, and eye strain. They also reported feeling like a “zombie,” overwhelmed, and feeling invisible. These findings were important insights into the somatic and emotional experience of occupational burnout, thus guiding the curriculum design into targeting these specific manifestations.
Theme #3: Protective factors
Examples of the protective factors that the participants’ offered were having experience in the field, having work options, standing up for oneself, and having knowledge and expertise, as evidence to support claims during conflicts. They also talked about being able to stand up to bullies, feelings of making a difference, connection, and interactions with patients, and being part of a team. They also wanted strong and supportive leadership, gratitude from patients, and knowing one’s personal limits. They also wanted supportive radiologists, who can say “no” to pressure, as well as each sonographer expressing their favorite sonography specialty. They advocated for a positive and supportive work environment, getting praise from supervisors and/or radiologists, networking and keeping contacts with mentors from school. They also valued having patience and having supervisory support in time of conflicts.
Participant Generated Solutions
Some solutions suggested by participants were clear guidelines on what an urgent (i.e. stat) sonogram is and how to manage this during overnight shifts, especially when there is only one sonographer working. They also mentioned educating the whole team on the limitations of sonography, as well as having a support group with other sonographers. They also wanted free massage therapy at work and also being able to voice struggles without retaliation. Other suggestions were an increased pay rate, educate administration about sonography, and no mandatory exam time slots for exams, as patient situations can be very unpredictable. They also wanted to educate students and help them develop more nonclinical (“soft”) skills, being more patient with new sonographers by giving them more time and support and setting a limitation on how many exams a sonographer does per shift.
Qualitative Analysis
An interesting finding of the qualitative data was a difference in perception and reaction to conflict and supervisors’ support between males and females. Among the eight interview participants, only three were male. While female sonographers were more likely to empathize with their supervisors and try to understand their challenges, male sonographers were more critical and placing blame on their supervisors. They also described their behavior as “bullies,” pointing out “they give preferential treatment” and blaming their supervisors for the new sonographers quitting. The language was also more direct when it came to patient interactions, especially when one male participant was able to recognize and label it, when patients were being abusive. Conversely, the female sonographers tended to justify patient’s reactions even if they were abusive or combative toward them. Male sonographers were more likely to stand up for themselves and say “no” to supervisors, whereas female sonographers tended to avoid such confrontations with authority figures. There was no difference whether the authority figure was a male or female. No female participants reported confronting their supervisor, despite problems, and challenges. One sonographer reported feelings of being “stuck” in a toxic environment and staying there for many years, which came with big consequences on her physical and mental health. Among female sonographers, there was a tendency to avoid conflicts, which probably is the root of the feelings of resentment, a repeated code that was subcategorized with the phrase: Manifestation of Burnout. Regarding awareness of work-related burnout, male sonographers reported not being burned out or at least not being aware of it. It is difficult to study how gender might influence differences in occupational burnout among male- and female-identified sonographers, as many sonographers tend to be females. However, when developing program interventions and/or preventions, such differences may need to be taken into consideration.
The source of occupational burnout themes, identified in the interviews, was supported by multiple studies,3 –9 which identified lack of supervisor/management as having a consistent impact on the sonographer’s sense of burnout. These findings also overlap with the quantitative data from the survey where high number of sonographic examination and feeling underappreciated were reported as the most important factors contributing their occupational burnout. While the interview participants were aware that practicing good ergonomics was important, some reported that maintaining good ergonomics was very difficult, due to the pressure of doing a lot of exams and having a limited rest between patients. In terms of solutions, having a support group was an important finding. This was also supported by the quantitative data where 46.1% said they would be interested in participating in a program intervention. During the interview, when asked what was helpful when going through difficult times at work, they mentioned the need to talk to other sonographers. One participant shared that it is hard to talk about work challenges with someone who does not understand or know anything about sonography and the taxing duties. This insight is important because it further suggested that a program intervention, implemented in a group setting, could be effective in supporting sonographers and helping them mitigate occupational burnout.
Discussion
When a problem such as occupational burnout is measured and identified, it is important to investigate the level of sonographer awareness. This becomes essential when developing program interventions or preventions that address work-related burnout. Awareness of a problem is the first step toward personal change. If sonographers are not open or willing to participate in such programs, this could be a major challenge in implementing such an intervention. However, the findings of this study suggested that this cohort of sonographers were aware and open to getting help. In the study by Callpani et al, 13 only 5% of participants reported receiving individual psychological help, but in this study 46.1% reported being interested in participating in an intervention program. It could be interpreted that this study revealed an unmet need that these sonographers had for support, which few had received, perhaps due to reasons such as lack of availability, stigma, cost, and so on. During the interview portion, participants suggested that group support could help mitigate burnout. It seems that being around other sonographers who are going through similar challenges may be viewed as helpful.
Prevalence and feelings around conflict is an important finding, as some studies have reported a link between conflict and occupational burnout, in other occupations.20 –23 However, to date, there are no published studies reporting a link between conflict and sonographer burnout. Nevertheless, conflict at work is almost inevitable and sonographers are not exempt, as was demonstrated in this study. Conflicts can be stressful, especially if individuals lack the skills to deal with them. The increased self-reported stress and anxiety when dealing with conflict at work, by this cohort, prompted the need to address it, as part of the intervention program. Also considering the overlap of occupational burnout, conflict, and anxiety,20 –24 a combination of therapeutic and somatic intervention (relaxation, grounding techniques) may help in decreasing the emotional component of burnout. The findings of this study were used to develop a curriculum for an intervention program, based at an individual level.
A prevention framework was the promotion of personal strengths, positive characteristics, and behaviors that serve as protectors against potential problems. 25 This was important to emphasize protective factors, identified in the qualitative data, to promote sonographers’ strengths and positive characteristics.
Leveraging the Research to Develop a Sonographer Support Group Curriculum
Group therapy is a form of psychotherapy where one or two trained therapists work with a group of people, which has been shown to be effective in improving each members’ symptoms and self-awareness. 26 This proposed curriculum was based on a cognitive behavioral group therapy (CBGT) approach, as a way to help sonographers learn new coping skills, in a supportive setting.26 –28 This evidence-based approach was highly structured, and it included cognitive restructuring, exposure therapy, problem-solving skills, role playing, and relaxation techniques. This combination has been shown to be effective in treating many mental health problems such as anxiety, phobias, posttraumatic stress disorder, and so on.26 –29 These techniques were adapted into the support group curriculum to specifically address sonographers’ needs and help them mitigate work-related burnout. Problem-solving skills, cognitive restructuring, and role playing are tools used in conflict resolution. Cognitive restructuring and relaxation techniques are used to address both the physiological and cognitive aspect of anxiety, when dealing with conflict at work. Self-compassion techniques were also incorporated into the support group curriculum, as such practice has been shown to help reduce anxiety, lower stress, and burnout.15,17,30,31 Considering the participants’ feelings of being “stuck” in their career and given the studies that pointed to sonographers who were thinking of changing careers or retiring,4,7 this factor was added in two group sessions to specifically address these challenges. The intended goal of those session is to help sonographers explore the feeling of being “stuck” in their career and getting more clarity regarding their decision to leave the profession.
The main objectives of the support group curriculum are to: Increase awareness of burnout and how it affects the body, brain, and the overall well-being. Increase self-compassion and incorporate such practices into daily work/personal activities. Provide conflict resolution skills. Foster skills to reduce stress and anxiety and regulate emotions. Please use the QR code to access an outline of the curriculum that was developed (See Appendix B—Insert QR).
Limitations
The main limitation to this study was the research design and the threats to internal and external validity. The cohort of sonographers who responded were formed by convenience and therefore the responses are specific to them. In addition, the survey instrument was developed for this study and was not validated. The cohort’s expressions of anxiety and stress, as they related to conflict, were self-reported data and a validated tools was not available to measure anxiety or conflict. The survey tool that was used to assess occupational burnout was also not validated. Another limitation was the small sample size, which only included sonographers who worked in New York City.
Future research should be done using the developed support group curriculum, as part of an intervention program, to evaluate its effectiveness in mitigating burnout. It may also be helpful in reducing feelings of stress and anxiety during conflict at work and increased overall well-being. Also, further exploration of conflict at work in the sonography can help to better understand the challenges that sonographers face and the possible links of conflict to occupational burnout. With these new insights, it may be possible to implement conflict resolution skills training, as part of sonography education. The goal would be to provide preventative measures, so that future sonographers are better equipped with tools to deal with conflicts at work. Using validated tools to measure conflict, anxiety, and objective measures of stress such as cortisol levels or physiological monitoring can be an added dimension to future research.
Conclusion
This study explored a cohort of sonographers who worked in New York City and reported feelings of occupational burnout. These data were pivotal in developing a curriculum for an intervention, specific to those expressed needs. The analysis of this study cohort demonstrated that they were aware of their occupational burnout and were open to participating in an intervention program. Based on the needs of this sonographer cohort, a CBGT curriculum was developed. The goal was to help sonographers navigate work conflicts, manage personal stress, and mitigate factors that could lead to occupational burnout.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793251316326 – Supplemental material for Developing an Intervention Program Based on a Cohort of Sonographers’ Occupational Burnout Experience and Mitigating Associated Factors to Improve Worker Well-Being
Supplemental material, sj-docx-1-jdm-10.1177_87564793251316326 for Developing an Intervention Program Based on a Cohort of Sonographers’ Occupational Burnout Experience and Mitigating Associated Factors to Improve Worker Well-Being by Veneta Callpani in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-2-jdm-10.1177_87564793251316326 – Supplemental material for Developing an Intervention Program Based on a Cohort of Sonographers’ Occupational Burnout Experience and Mitigating Associated Factors to Improve Worker Well-Being
Supplemental material, sj-docx-2-jdm-10.1177_87564793251316326 for Developing an Intervention Program Based on a Cohort of Sonographers’ Occupational Burnout Experience and Mitigating Associated Factors to Improve Worker Well-Being by Veneta Callpani in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The author acknowledges Nadia Alkaysey BS, Sheana Gordon BS, and Kayla Worrell BS, for their help in distributing the survey and interview scheduling.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics approval for this study was obtained from State University of New York (SUNY) Downstate Health Sciences University (IRB# 2118185-1).
Informed Consent
An online survey form allowed participants to check the “I agree” box and agree to participate in the study. By checking the box, they also confirmed that they were 18 years or older. If the participant did not wish to participate in the study, they simply closed out of the browser window.
Animal Welfare
Guidelines for humane animal treatment did not apply to this study because no animals were used during the study.
Trial Registration
Not Applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.