
Abstract
A 9-year-old boy was diagnosed with an isolated single coronary artery (ISCA) complicated by myocardial bridging, where an anomalous left main coronary artery (LMCA) arises from the proximal right coronary artery (RCA), with an intramyocardial course. The patient was referred for an echocardiogram after being diagnosed with hypertension, which revealed the ISCA, significantly increasing his risk of myocardial ischemia and sudden cardiac death. He experienced exercise-related chest pain, leading to a comprehensive cardiac evaluation. Cardiac computed tomography confirmed the anatomical abnormalities, and a treadmill stress test demonstrated intermittent ST segment depression during peak exercise. Surgical intervention included pulmonary artery mobilization, unroofing of the LMCA, and reattachment of the pulmonary artery. Postoperative echocardiograms showed unobstructed flow and normal biventricular function. Following surgery, the patient reported no further chest pain and exhibited significantly improved exercise tolerance. This case report highlights the critical importance of recognizing congenital coronary anomalies, in pediatric patients, and the necessity for thorough assessments during echocardiograms, as symptoms may often be misattributed to non-cardiac conditions. Early detection and intervention are essential to mitigate the risks associated with these rare cardiac anomalies.
Keywords
A case report is provided that describes a 9-year-old boy with an isolated single coronary artery (ISCA). This case, in which an anomalous left main coronary artery (LMCA) arises from the proximal right coronary artery (RCA) with an intramyocardial course, represents a decidedly rare variant with a presumed increased risk of myocardial ischemia and sudden cardiac death (SCD).
Case Report
A 9-year-old boy was referred for an echocardiogram, following a diagnosis of hypertension by nephrology. The patient was noted to have a body mass index (BMI) of 21.53. The echocardiogram revealed an ISCA. The RCA ostium origin was from the right sinus with an early branch off the RCA coursing leftward, anterior to the pulmonary trunk, representing the LMCA. The LMCA was not seen in the usual location (see Figures 1–4; QR code: Video 1). The remaining cardiac anatomy and ventricular function was normal. Due to the echocardiographic findings, the patient was referred to cardiology.
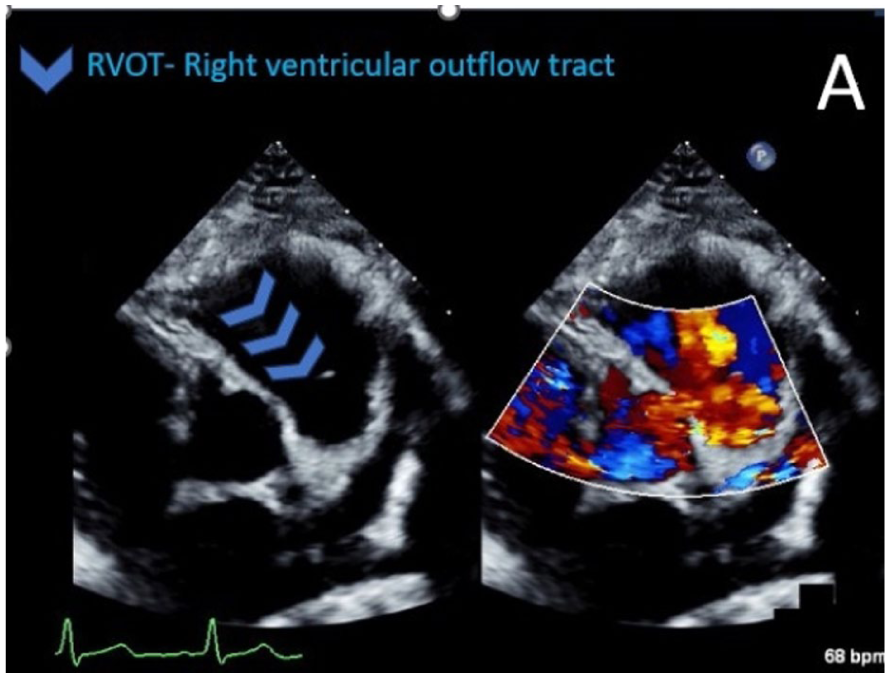
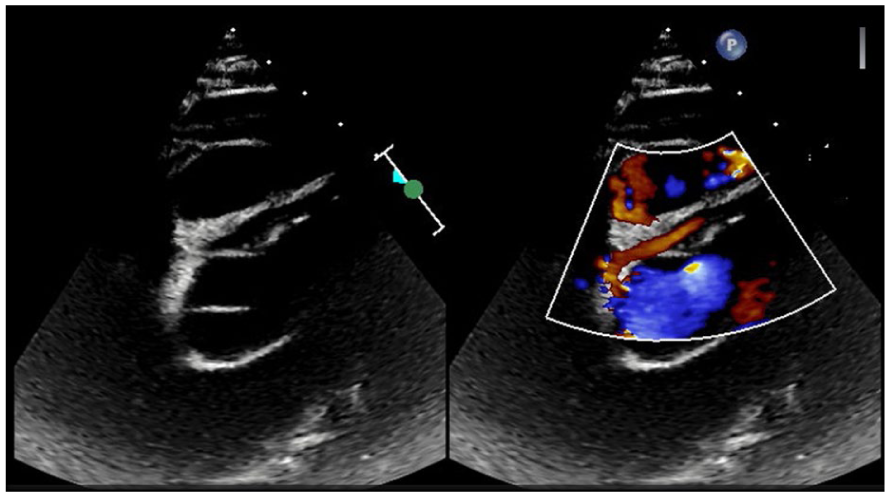
An echocardiographic short-axis view highlighting the right ventricular outflow tract (RVOT), indicated with blue arrows.
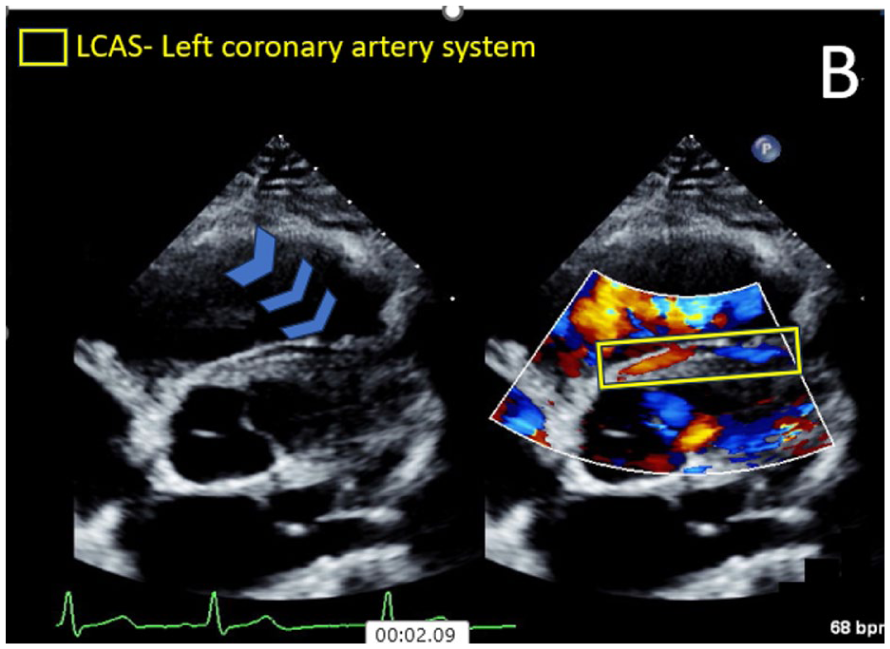
An echocardiographic short-axis view showing the course of the left coronary artery system, across the right ventricular outflow tract (RVOT) and visualized with color Doppler.
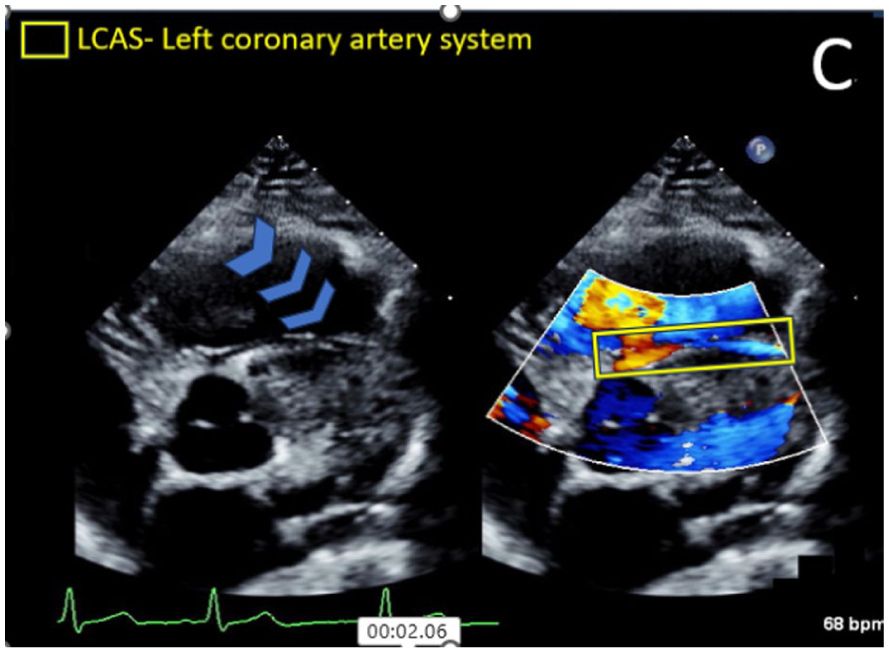
An echocardiographic short-axis view illustrates the course of the left coronary artery system, across the right ventricular outflow tract (RVOT) and slight aliasing observed with color Doppler.
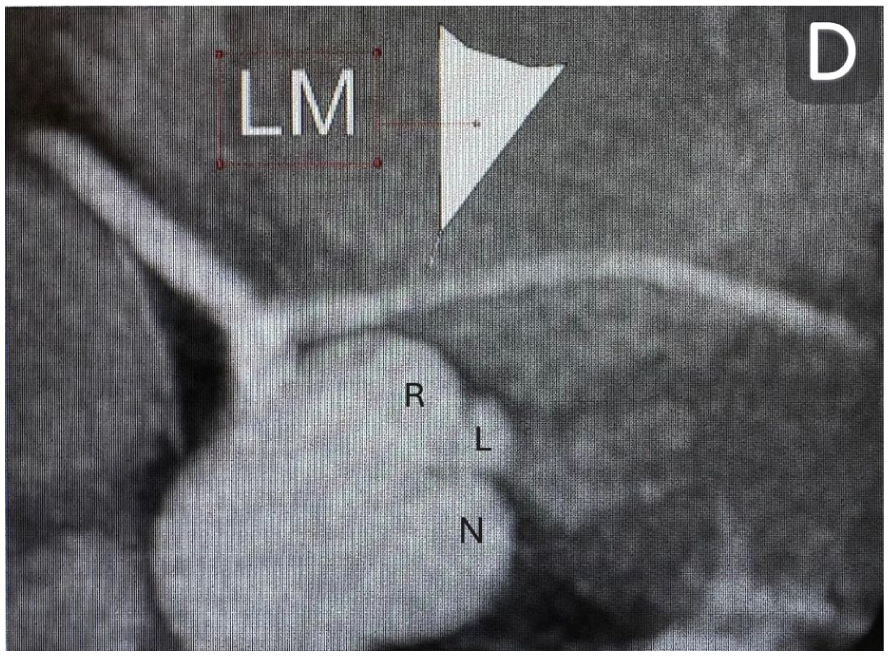
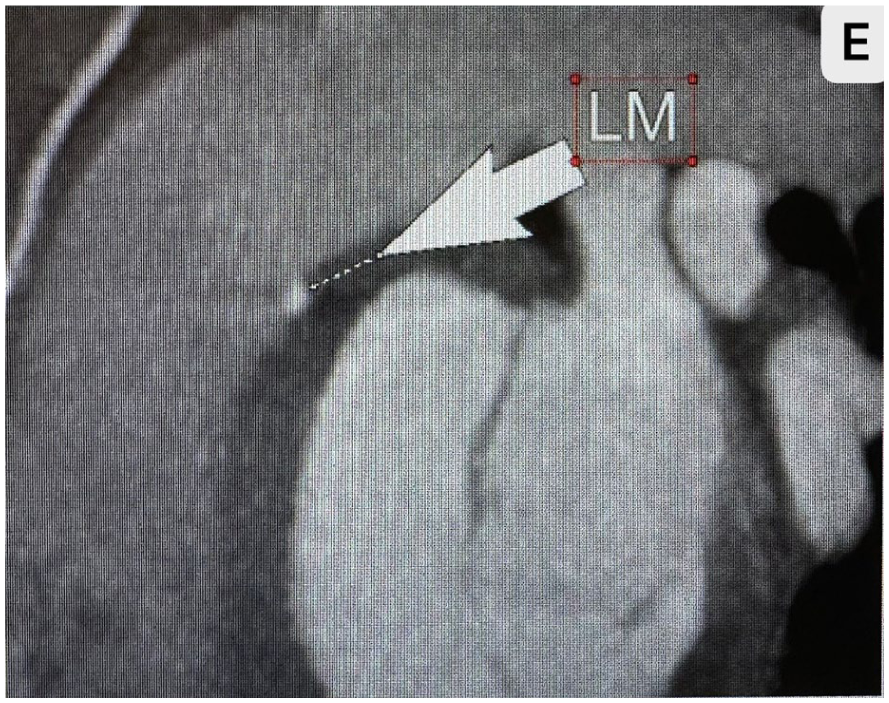
A computed tomography angiogram (CTA) is provided that illustrates the coronary anatomy. An arrow indicates the distribution of the left main coronary artery, arising from a single coronary artery.
During the cardiology evaluation, his history revealed intermittent exercise-related chest pain that resolved with rest. Past medical history was significant for delayed gastric emptying, bone age advancement, and premature puberty. The patient’s renal evaluation was found to be normal. His family history was significant for paternal early-onset hypertension, diabetes, and hypercholesteremia. The patient’s maternal family history is unknown due to patient being a product of in vitro fertilization with an egg donor.
The patient was restricted from vigorous activities and sports. Cardiac computed tomography (CCT) demonstrated a single coronary artery (SCA) from the right sinus with an anomalous origin of the LMCA from the proximal RCA. The LMCA course was anterior to the right ventricular outflow tract (RVOT) before giving rise to the left anterior descending LAD and left circumflex LCX coronary arteries. There was also a long segment of the intramyocardial course of the LMCA as it crossed the RVOT (see Figures 5–7).
An additional computed tomography angiogram (CTA) image is provided that highlights the coronary artery and is marked with an arrow.
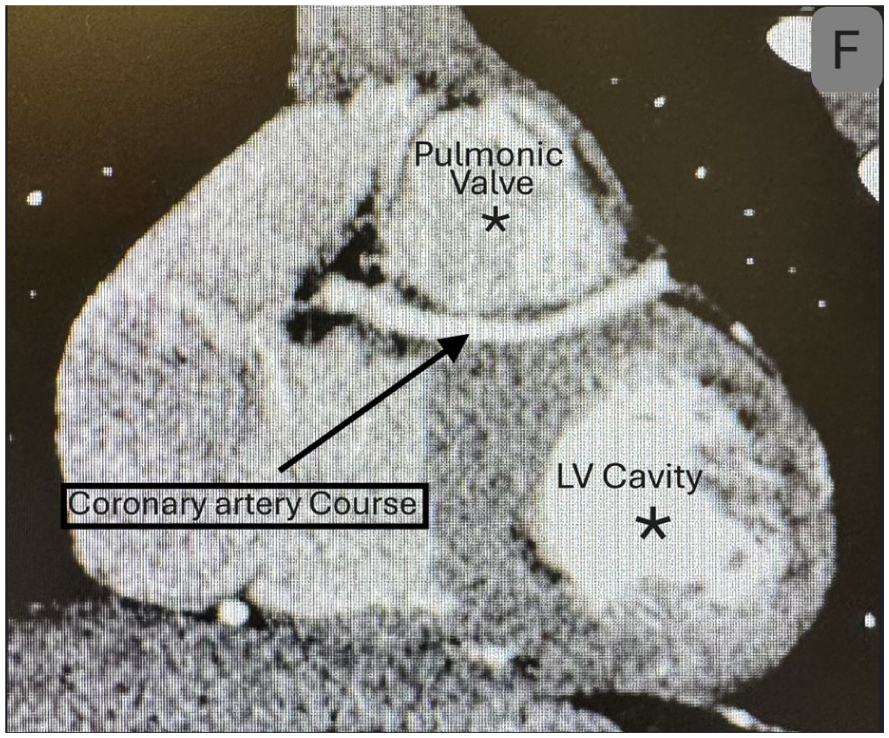
A computed tomography angiogram (CTA) is provided that shows the course of the coronary artery through the myocardium.
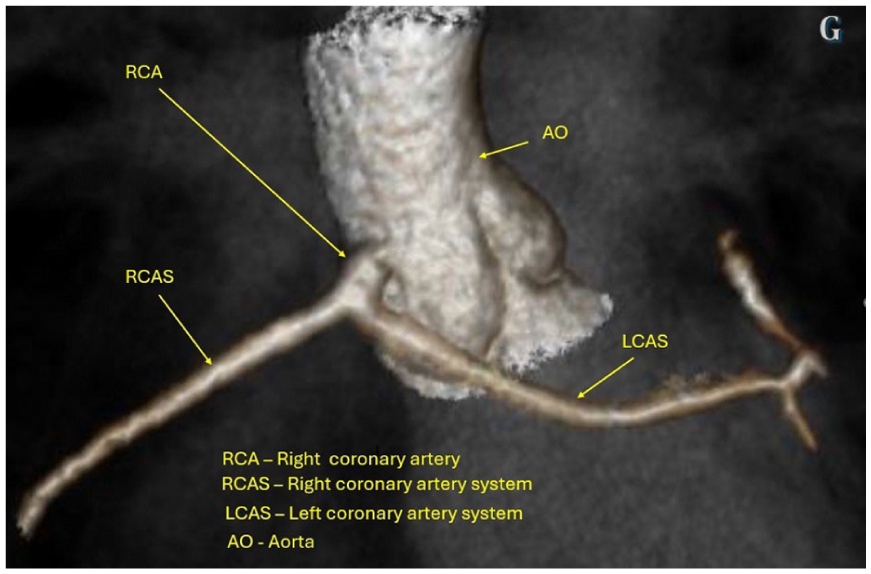
A computed tomography (CT) with volume rendering provided a 3D image with arrows indicating the locations for enhanced understanding anatomy.
In context of the CCT findings and a history of intermittent exercise-related chest pain, a treadmill stress test was ordered. The patient completed 10:39 minutes of standard Bruce protocol treadmill testing and achieved 90% of the maximum predicted heart rate. The patient experienced chest pain during peak exercise, like the previous symptoms experienced during physical exertion. At peak exercise, ECG demonstrated mild intermittent ST depression in V4-V6 with quick resolution post-exercise. Surgical intervention was recommended after review of all the diagnostic findings.
Cardiac surgery included pulmonary artery mobilization and unroofing of the muscle over the septal course of the LMCA, and reattachment of the pulmonary artery with a 28-mm pulmonary homograft extension (see Figures 8–10; QR code: Video 2).
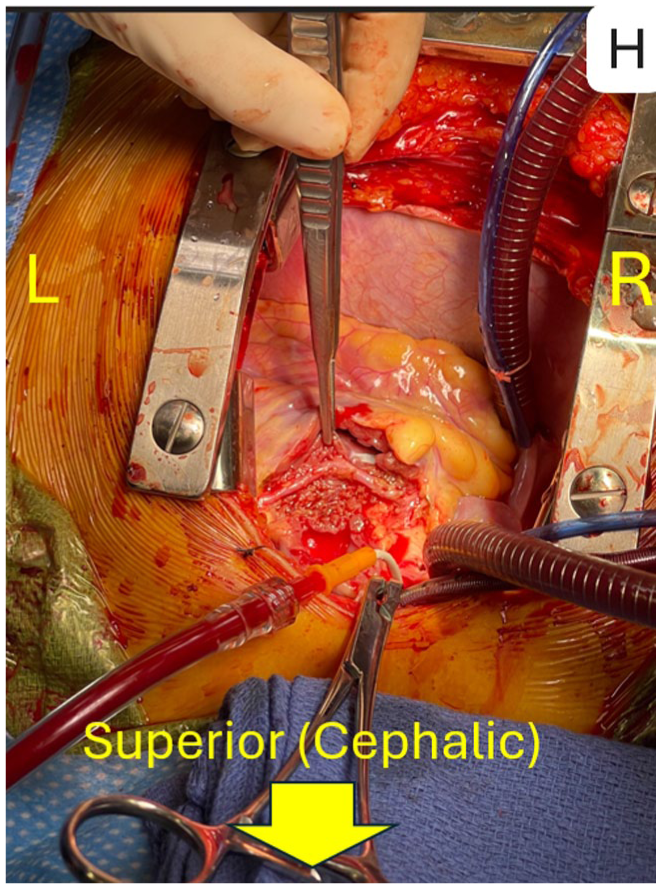
An image is provided from the patient’s intraoperative of heart surgery. An arrow indicates the superior aspect, R-right, L-left. The surgeon is retracting tissue, as seen in this image.
A postsurgical echocardiogram is provided with a transthoracic short-axis view, which illustrates normal laminar flow, without aliasing through the coronary artery.
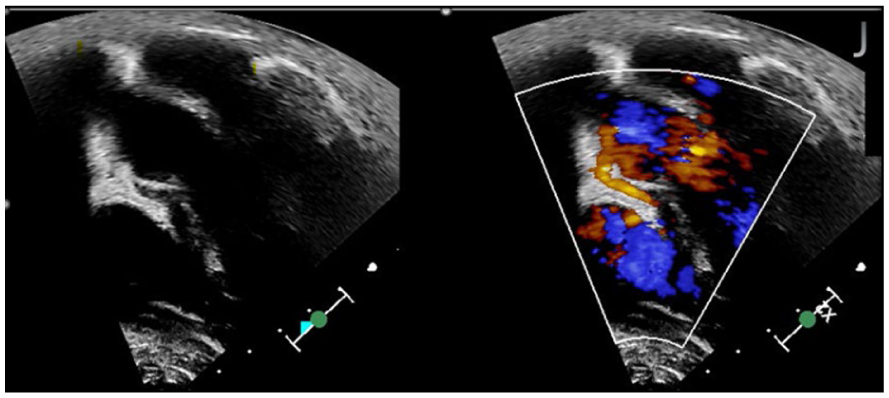
An echocardiogram is provided that included an apical approach, utilizing 2D imaging, and color Doppler. This image provided an additional view of laminar flow, through the coronary artery.
Postoperative echocardiograms demonstrated unobstructed flow in the visualized portions of the SCA with normal biventricular function and no wall motion abnormality. The patient’s postoperative course was uncomplicated, and he was discharged home, on the sixth postoperative day. The patient became asymptomatic with no further chest pain with exertion. On an exercise stress test done 4 months postsurgery, the patient completed 10:44 minutes of standard Bruce protocol treadmill testing and achieved 90% of maximum predicted heart rate, without any chest pain or other symptoms, and without any ST abnormalities.
Discussion
Clinicians are consistently faced with unique complexities and challenges in patients with an anomalous origin of coronary arteries. 1 A congenital abnormality, of coronary arteries, is the second leading cause of SCD in young athletes. 2 However, diagnosis of patients with coronary artery anomalies is especially challenging since many patients are asymptomatic with sudden cardiac arrest, often being the first or only symptom. Implementing a comprehensive precompetitive screening may be appropriate especially when there is a history of chest pain and/or syncope during physical activities or a family history of congenital heart disease and sudden death.
Echocardiography plays an important role in diagnosis of congenital heart disease, particularly in identifying coronary artery anatomy and potential abnormalities. It is crucial to implement standardized protocols for assessment of coronary arteries origin and course during the initial echocardiogram. Pediatric sonographers should be trained in the assessment of coronary arteries as part of all pediatric echocardiograms.
Single origins of coronary arteries are a rare subset of coronary artery abnormalities. SCA is defined as an isolated coronary artery that arises from a single coronary ostium and provides blood supply to the entire myocardium. 3 The reported prevalence of SCA is ranging from 0.024% to 1.0%. 3 This defect can be present in isolation or in association with other congenital cardiac defects. Most of the patients with SCA are asymptomatic but patients with some variants of SCA are at increased risk of myocardial infarction, ventricular arrhythmias, and SCD. 4 In most of these patients, there is an intramural course which may be a major contributing factor.
The Lipton-Yamanaka classification categorizes SCA based on the origin, course, branching pattern and relationship of the transverse artery with the aorta and the main pulmonary trunk. 5 SCA with an interarterial course, anomalous artery passing between the ascending aorta and the main pulmonary artery, has been associated with myocardial ischemia and sudden death and especially among young competitive athletes.5,6 Myocardial bridging (MB) occurs in 0.5% to 16% of the patient population, based on coronary angiography. 7 MB is characterized by a segment of the coronary artery being sandwiched between the myocardium. This anomaly creates a milking effect that is often recognize in angiography procedures.
Based on Lipton-Yamanaka, this patient’s coronary artery course would be classified as RIIA (LCA after arising from RCA courses anterior to the pulmonary artery). Since LMCA crosses anterior to the pulmonary artery without an interarterial course, it is thought to be at a lower risk of coronary obstruction. However, computed tomography angiogram (CTA) revealed an intramyocardial course, consistent with MB of the LMCA, as it crosses anterior to the pulmonary artery trunk. This is thought to be secondary to extrinsic compression of the intramyocardial segment during systole and incomplete decompression in early diastole leading to decreased coronary perfusion. 8 Risk of myocardial ischemia is increased with physical exertion by increasing the myocardial oxygen demand combined with decreased perfusion through the intramyocardial segment, as well as reduced diastolic perfusion time. 8 This patient’s symptoms of chest pain with exertion that resolved following surgery were consistent with this finding.
Conclusion
This case study is extremely rare and highlights the significance of recognizing and managing rare congenital coronary anomalies, in pediatric patients. It highlights the importance of evaluating coronary arteries in all pediatric echocardiogram, regardless of indication for the study. As is underscored by the current case where the echocardiogram was ordered to evaluate for left ventricular hypertrophy, in a patient with hypertension. A SCA with MB is challenging, hard to diagnose, and could be easily overlooked. Reported symptoms such as chest pain, in a pediatric patient, could be easily attributed to other noncardiac issues, such as musculoskeletal, gastrointestinal, pulmonary, or anxiety related. Following a comprehensive pediatric cardiac protocol assessment can provide early detection of coronary anomalies and early intervention when necessary.
Supplemental Material
sj-pdf-1-jdm-10.1177_87564793251371587 – Supplemental material for Rare Congenital Coronary Anomaly of Myocardial Bridging in a Pediatric Patient With Isolated Single Coronary Artery
Supplemental material, sj-pdf-1-jdm-10.1177_87564793251371587 for Rare Congenital Coronary Anomaly of Myocardial Bridging in a Pediatric Patient With Isolated Single Coronary Artery by Jose L. Bastida, Mohammad B. Rahimi and Saar Danon in Journal of Diagnostic Medical Sonography
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought for the present study because all patient information was de-identified.
Informed Consent
Informed consent was not sought because all case data were de-identified and/or aggregated and followed the ethics committee or IRB guidelines (also referred to as the Honest Broker System.)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.