
Abstract
Vascularisation of scaffolds is now recognised as a crucial requirement for the success of tissue engineering strategies. This review summarises the state-of-the-art in the techniques available for the in vivo assessment of vascularisation of scaffolds with focus on growth factor delivering scaffolds, microfabrication technologies and in vivo characterisation methods based on the arteriovenous loop model to create three dimensionally vascularised tissue replacements.
Introduction
The creation of living tissue or organ substitutes for the cure of diseases, organ failures and functional or aesthetic tissue losses of any human body part or structural unit has been the dream of mankind for centuries. 1 Only when pioneers of the field started to look for serious alternatives to overcome the shortage of donor organs for transplantation the idea of culturing human cells on suitable carriers was fostered and eventually the term tissue engineering (TE) was coined.2,3 It turned out that the combination of clinical expertise with biomaterial research, basic biological and engineering science offers a new field of research, which can be applied in various ways. On the one hand, the ignition spark of creating living organs or whole extremities in the laboratory leapfrogged these initial aims, and on the other hand, new insights from this truly interdisciplinary emerging field offered platforms for a number of scientific questions to be answered by means of cell culture and TE. 4 One such innovative research direction is the study of angiogenesis mechanisms and tumour cell growth and, with in vitro and in vivo models, the potential spreading mechanism of certain tumour cell cultures under controlled laboratory conditions. 5
In addition to that, techniques of TE have now merged with concepts from regenerative medicine (RM) that rely more on the capacity of cells to develop, stratify, grow and repair defects or lost organ tissue once it has been successfully engrafted into a host. Within the last 10 years, the advent of stem cell research (embryonic and adult stem cells have separately provoked attention) and the detection of induced pluripotent stem cells have opened new horizons to combine TE and RM for the cure of patients. 6
While many experiments have shed light on the principal methods to generate living cell cultures on various two- (2D) and three-dimensional (3D) scaffolds, the clinical translation has been hampered by the lack of vasculature at the time of transplantation when it comes to clinically significant sizes of tissue substitutes. 7 Therefore, to prevascularise large tissues remains a vital challenge for the manufacturing of large or complex organs. 8 As long as no direct perfusion of all relevant cells within a 3D construct is established in order to supply sufficient oxygen, the distance of cells to blood vessels is one limiting factor for cell survival. It has been proposed that distances of more than 200 μm between cells and blood vessels are critical for most cells and that specific sensitive cells do not tolerate distances over 100 μm, while on the other hand, metabolically less demanding cell types such as chondrocytes tolerate more oxygen depletion and can maintain viability in grafts up to 1 mm thickness. 9 This strict relationship between the nourishing vascular supply and cell oxygenation and survival has been shown even in more or less 2D TE substitutes, such as cultured epithelial autografts.10,11 One way to circumvent this diffusion barrier was the use of single cell transplantations in appropriate transfer media, such as fibrin sealant.10–13 Recently, the concept of using single cells as a source of regeneration was also integrated in the creation of encapsulated adipose derived stem cells into poly(d,l-lactic-co-glycolic acid) (PLGA) scaffold with interconnected channels using 3D printing techniques to build the PLGA scaffold. 14 It has been shown that such encapsulated adipose derived stem cells can differentiate into endothelial and smooth muscle cell lineages respectively and that they do correspond to their respective locations within the construct. 14
Since multimodal treatment regimens including surgery, chemotherapy and irradiation gain in importance, the spectrum for clinically relevant applications of TE products becomes more sophisticated. This is also true for the elderly and multimorbid patients with vascular diseases15,16 because tissue oxygenation and microperfusion decrease with age and depend on cardiac function. 17 That means that, in most cases, the host's vascularisation will not be sufficient to nourish the implant, especially during the early period after implantation. 18 Therefore, the integration of vascularisation strategies seems crucial for the clinical transplantation of large TE constructs into human applications, 19 and promoting various vascularisation strategies to support engraftment, integration and consecutive differentiation of cell based tissue substitutes will be one major challenge for the future of TE and RM. 20 The in vivo prevascularisation of biomaterials with arteriovenous loops (AV loops) previous to cell seeding21–23 is one microsurgical approach to be combined with cell cultures on appropriate biomaterials to mimic transplantable tissue surrogates similar to free flap transplantation with vascular anastomosis.24–28 Tissue engineering studies with AV loops have also added to a better understanding of the mechanisms of angiogenesis and vessel network generation in a biological environment. 18 Nevertheless, reliable growth of complex replacement tissues or whole functioning organs, such as heart, muscle, kidney, liver and lung, which are ultimately the goal of TE, seems to be distant milestones at the moment. 29 Besides the constantly improving methods of cell culture in 2D and 3D culture systems and in bioreactors, the main targets of future approaches can be seen in developing better biomaterials, designing TE based drug delivery systems, generating adequate cell sources (including stem cells) and vascularising TE products of clinical relevant size to be transplanted to patients.
Angiogenesis and vasculogenesis in TE and RM
In terms of vascularisation, three distinct phenomena can be distinguished, namely, angiogenesis, vasculogenesis and arteriogenesis,30,31 which are relevant for TE purposes. The initial stimulus to better understand all aspects of angiogenesis came from the paradigm of a therapy aimed at inhibiting the formation of blood vessels in malignant tumours. J. Folkman suggested that depletion of blood vessels would consequentially deprive cells and tissues of oxygen and nutrients. 31 This concept premises that blood vessel formation is central to the progression and maintenance of diseases, which involve cellular metabolism and tissue expansion, and cancer in particular. In contrast to the role of blocking vessel outgrowth in cancer, in the field of TE, the propagation of angiogenesis and detection of angiogenic and vessel sprouting promoting agents are desirable. Nevertheless, the study of the underlying mechanisms in both ways will help to optimise integration of TE constructs into hosts. The induction of angiogenesis has been postulated for therapeutic purposes as an application of biotechnology to stimulate new vessel formation via local administration of proangiogenic growth factors. This could happen in the form of gene therapy or specific proteins. The implantation of endothelial progenitor cells32–34 in various ways has also been attempted to durably deliver cells that will synthesise multiple angiogenic cytokines once they are integrated.
In patients with ischaemic diseases, the stimulation of vessel growth and remodelling utilising TE methods, based on the administration of growth factors or progenitor cells from diverse sources, have been proposed as an alternative. Such approaches are currently tested in patients with peripheral arterial disease or cardiac diseases as a potential therapeutic option. 35
Optimisation and vascularisation of TE constructs can be categorised into various approaches. On the one hand, the addition of numerous growth factors alone or to various scaffolds has been considered but with unsatisfactory results.36–44 This was also reported with different bioactive glasses in combination with different therapeutic drugs, hormones, growth factors and peptides, which can be utilised for bone regeneration. 45 Using bioactive glasses as drug delivery system combines the effectiveness of therapeutic drugs with the intrinsic advantages of inorganic biomaterials and may contribute to help neoangenesis to happen in the recipient organism. 45 Others have studied the angiogenic effects induced by combinations of biodegradable gelatin hydrogel granules incorporating mixed platelet rich plasma growth factor mixture and bioactive basic fibroblast growth factor, which was found to enhance angiogenic effects. 46 However, all of these concepts mainly rely on an initially sufficient blood flow in the recipient host to vascularise the construct from the outside to the inner space via the extrinsic pathway. Thus, thick grafts or grafts with sensitive cells will not be adequately perfused during the early phase of enrgraftment, and only thin grafts may profit from this modality. 29
On the other hand, the creation of spaces, tubes or channels to allow for microvascular ingrowth by means of material science and engineering seems also a promising way with regard to micronourishment of transplanted cells in constructs.47,48 Microfluid networks can be incorporated into the scaffold when computer aided printing techniques help generate different 3D textures to allow for diffusion of fluids in thick organs in robust or soft synthetic biopolymers.49,50 New technologies like automatic layer by layer micromoulding strategies may enable to reproducibly fabricate 3D microfluidic porous scaffolds directly from the aqueous solution of soft natural biopolymers with interconnected microfluidic networks into the extracellular matrix. 49 It has been envisioned that also the developmental biology concept of embryonic tissue fluidity could be combined with engineering approaches to render the creation of a new rapid prototyping 3D organ printing technology possible, which could accelerate and optimise tissue and organ assembly. 51
Other concepts could arise from a better understanding of mesenchymal stem cells (MSC) in TE and RM. Mesenchymal stem cells have been described to be central to the three main vascular repair mechanisms. They are heterogeneous, contain multilineage stem and partly differentiated progenitor cells and are easily expandable ex vivo, and their phenotype is significantly determined by their specific microenvironment. Especially bone marrow MSCs with their perivascular location might contribute to angiogenesis and function and could therefore be harnessed to regenerate a blood supply to TE constructs or injured tissues. 52
A combination of surgical tools derived from the field of microsurgery and supramicrosurgery and TE concepts to prevascularise small and large scale tissue substitutes has been widely examined by various groups to allow for a successful transplantation into hosts. This method relies on a microsurgical operation to generate a microvascular network into a biomaterial scaffold using an autologous AV loop first and implanting the target cells after an initial period of vessel implantation at the heterotopic site. Only after a 3D network has been formed by intrinsic vascularisation cells are implanted, and the graft is ready for transfer.5,20,22,53,54,55,56,57,58,59,60,61,62
Angiogenic growth factors
Angiogenic growth factors have emerged as an important tool for enhancing vascularisation of engineered tissues. Multiple growth factors are known for their angiogenic potential such as basic fibroblast growth factor (bFGF), 63 interleukin-8, 64 platelet derived growth factor-BB (PDGF-BB), 65 transforming growth factor-beta, 66 tumour necrosis factor-alpha 67 or vascular endothelial growth factor (VEGF). 68 These growth factors can be applied as single growth factors or in combination with others to increase their angioinductive potential. To minimise the disadvantage of fast degradation in vivo of growth factor therapies, a delayed release of these bioactive proteins should be provided by the scaffold for efficient neovascularisation. One of the most extensively studied matrices as a growth factor releasing scaffold is the fibrin glue matrix.69,70,71 Fibrin based biomaterials are used in wound healing therapies because of the fact that physiological fibrin matrices are known for their neovascularisation ability in injured areas. 72 Fibrin is a biodegradable matrix through tissue fibrinolysis and can also serve as carrier for transplanted and immobilised cells. The controlled dose and time dependent release of growth factors is mainly accompanied by a slow degradation process, which on the other hand depends on the fibrin glue composition and the addition of fibrinolysis inhibitors, such as aprotinin. 73 The control of the growth factor release kinetic also depends on the used angiogenic growth factor and its tight or weak binding to fibrin. 72 Basic fibroblast growth factor for example is known for its tight binding to fibrin glue and is therefore released in a slow and controlled manner. Vascular endothelial growth factor shows different binding affinities depending on the VEGF isoform. Vascular endothelial growth factor121 for example has a very weak binding to fibrin and is therefore released very fast, whereas VEGF165 was more tightly retained by the clots and thus was released for a longer time period. 72 Also the combination of bFGF and VEGF showed an increased angiogenic potential and more mature vessels compared to the single growth factor application. 28 Basic fibroblast growth factor was also attached to a gelatin hydrogel as a carrier in a rabbit model of hind limb ischaemia and showed 4 weeks after treatment an increased blood flow and vessel density in a dose dependent manner. 74 Also irradiated osseus defects were used to determine the angiogenic effect of VEGF. Two weeks after irradiation of the calvarium, 3·5 mm osseus defects were created and PLGA (copolymer of D,L-lactide and glycolide) scaffolds were inserted with and without incorporated VEGF. 75 Histology showed a significant increase in blood vessel formation and function when using VEGF scaffolds compared to PLGA matrices. Heparinised matrices were utilised to deliver different growth factors with different binding sites and therefore different release kinetics. In subcutaneous implantations, VEGF was detected to be responsible for early angiogenic effects, whereas the incorporation of PDGF-BB resulted in a substantial increase in neovascularisation after 2 months. 76 Microspheres have been described for sustained release of angiogenic growth factors such as bFGF. 77 Leach and co-workers have also implanted VEGF releasing scaffolds coated with bioactive glass in a rat critical sized defect model. 78 They were able to show an enhanced angiogenesis in the coated VEGF releasing scaffolds compared to coated control scaffolds. Elcin and co-workers implanted VEGF activated PLGA sponges in a subcutaneous model in the rat and were able to show new blood vessel formations in the growth factor group infiltrating the sponge pores compared to growth factor free controls or VEGF injections with a much lower or no angiogenic response. 79 An approach to control release kinetics of different growth factors was recently introduced using core–shell microcapsules. Choi et al. encapsuled PDGF and VEGF separately in the core and shell using PLGA and alginate in a layer by layer assembly. 80 It was found that the microcapsule mediated growth factor delivery showed more angiogenic activity compared to the conventional growth factor delivery.
Vascularised bioartificial tissues and organs in vivo: AV loop model
In vivo vascularisation of a matrix or a scaffold offers a number of advantages to generate a prevascularised structure and deliver progenitor or specialised cells to it as the blood vessel tree continues to grow. 81 Tedious in vitro preparations can be avoided, and the desired biomaterial can be generated in the organism directly. Hypoxia, as it artificially occurs in most approaches where cells are combined with a matrix followed by transplantation into an initially avascular recipient bed where the blood supply has yet to grow into the construct, can hence be avoided.
An appealing advantage of the in vivo approach is to make use of the fact that potentially useful cell populations already exist in the body and may be attracted to the site of tissue repair. 82 Endothelial progenitor cells may circulate in the peripheral blood or be localised in the bone marrow and other sites of the body. They have been under intense investigation in the past due to their angiogenic (either directly or via secondary cytokines such as VEGF5,82 and vasculogenic via direct integration and subsequent de novo blood vessel formation) properties. Experimental and clinical research has demonstrated EPC from bone marrow or blood in ischaemic tissues with chemotactic agents such as granulocyte colony stimulating factor or drugs such as statins.
A functional and adequate blood vessel network is mandatory to generate viable engineered tissues and organs. When in vitro engineered constructs containing cells are transferred in vivo, they lack a defined axial blood supply consisting of a main arterial inflow and a venous outflow respectively and therefore rely on blood vessel ingrowth from their surroundings.5,22,33,82,83,84,85,86,87,88 Nutrient supply to cells via diffusion occurs only up to approximately 200 μm into the matrix, resulting in insufficient nutrition and subsequent loss of cells located at the centre of such in vitro engineered constructs.5,19,84
Vascular supply is essential for successful TE applications when cartilage and skin are not involved, and a defined vascular axis allows for transplantation of the bioengineered tissue or organ to a different site. As opposed to other techniques, these tissues are immediately connected to the systemic blood circulation upon implantation.
A current successful development is the establishment of an AV loop model based on the femoral vessels, including a venous graft from the contralateral side in a rat separation chamber, which also constitutes an in vivo bioreactor. This work is based on the initial description by Erol and Spira 89 who successfully generated a prefabricated skin flap by creating an arteriovenous vessel loop using either arterial or venous grafts in a rat model. They recorded the 3D development of a dense vascular system originating from the entire AV loop. Later modifications of this basic principle included isolation of the AV loop into chambers and induction of vascularisation in polymer matrices.
Lokmic et al. implanted the AV loop into a polycarbonate chamber. 90 They were able to show the generation of vascularised tissue surrounding the AV loop. Zdolsek and co-workers used an ‘off the shell’ vascular allograft instead of an autologeous vein in the AV loop model. 91 No significant differences could be detected between autograft and allograft regarding vascular volume, construct weight and morphology at 2 and 6 weeks after implantation.
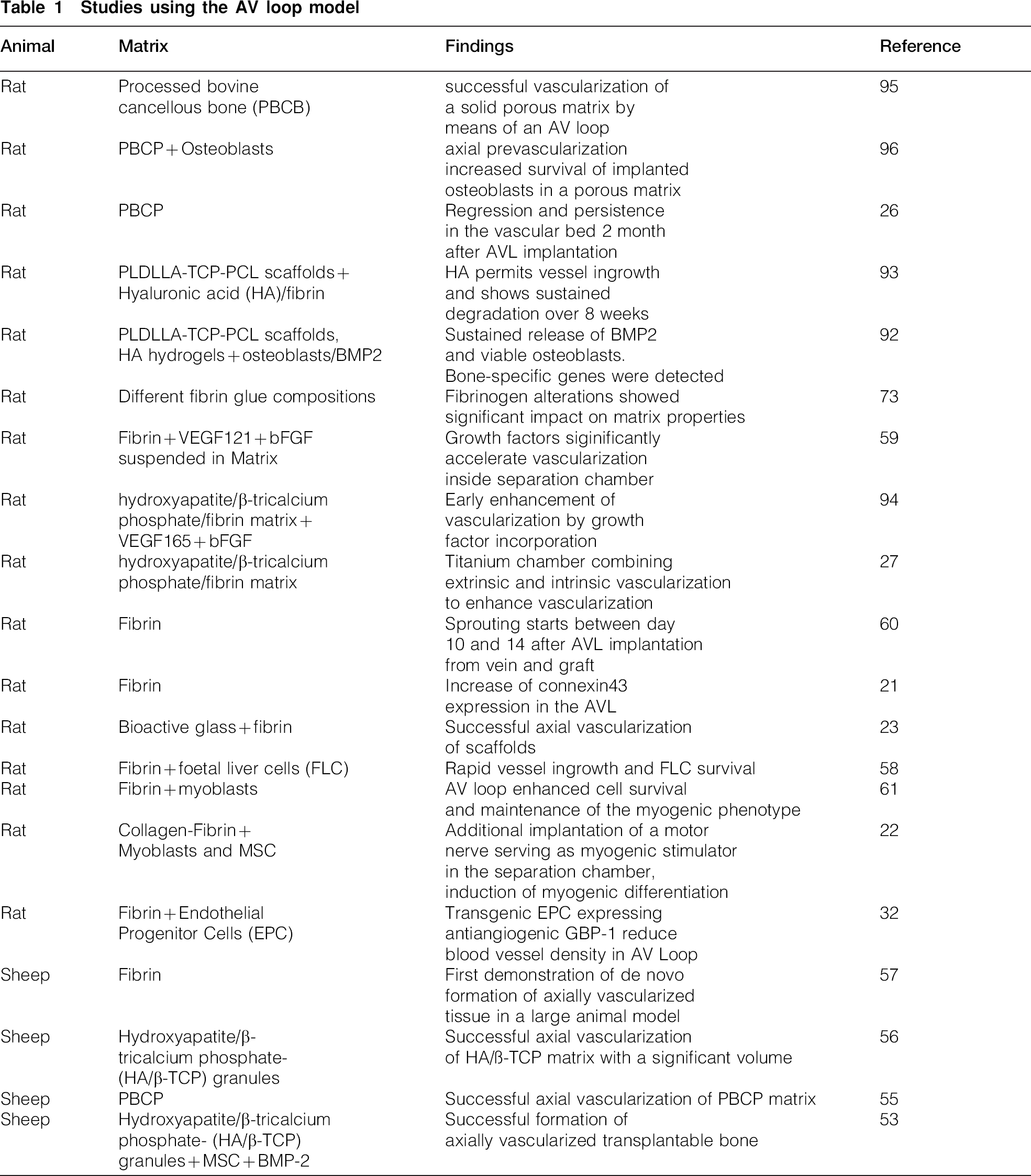
Our own group, inspired by the potential of the system and the appeal of the surgical approach, successfully adopted the model with the initial aim to grow vascularised tissue engineered constructs.21,92,93 A summary of previous work involving vascularisation of constructs and in vivo investigations using the AV loop model is presented in Table 1, and key results are discussed in this section.
Studies using the AV loop model
Initially, we established several different methodologies to enable imaging of the vascularisation (1) including corrosion casting, scanning electron microscopy (SEM), microcomputed tomography (micro-CT) scanning (Fig. 1) and histology. Using SEM it was found that the interpositional venous graft and the femoral vein showed direct luminal sprouting between day 10 and 14 after AVL implantation. 60 More recently, an observer independent automatic quantitative micro-CT evaluation technique was established for the first time allowing the 3D analysis of scaffold vascularisation. 94
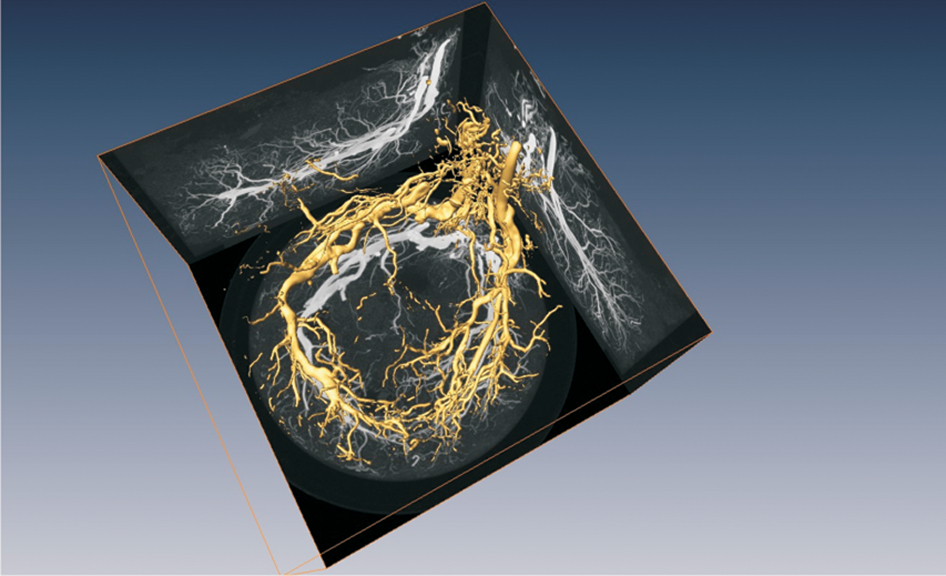
Micro-CT scan of explanted construct including AV loop: system has been perfused with microfil contrast agent to enable visualisation of vascular tree
Using SEM of corrosion casts and histological techniques, vascularisation was further investigated in the AV loop model. 26 The technique enabled to detect processes of regression and the persistence within a time frame of 8 weeks after AVL implantation. Also maturation of vessels and the presence of lymphatics were visible in this setting.
In addition, blood vessel ingrowth into a custom made processed bovine cancellous bone matrix by means of the AV loop was characterised. 95 It was demonstrated that more than 90 of the scaffold vascularised 8 weeks following implantation, using histology based morphometric analysis. Prevascularisation of these matrices significantly improved survival of osteoblasts engrafted into the matrix, emphasising the importance of an intrinsic blood supply for cell vitality within the construct. 96 In the meantime, a large diversity of sophisticated new materials to generate hard tissues has been under investigation, including bioactive glasses, hydroxyapatite and beta-tricalcium phosphate.23,85,94
The use of the AV loop model may also be useful for the replacement of soft tissues. 58 We have demonstrated that a fibrin gel approved for clinical use can be employed to generate a fibrin matrix, which was successfully vascularised and may be used as a platform to create soft tissues or organoids. This in vivo bioreactor was also responsive to proangiogenic stimuli, as demonstrated by the incorporation of recombinant growth factors VEGF and bFGF in the fibrin matrix where vascular outgrowth was significantly accelerated.59,62 Also different compositions of fibrin glue showed a significant impact on the vascularisation properties of fibrin matrices in the AVL model. 73
To overcome two-step procedures when using cell containing scaffolds and to enhance vascularisation of matrices, porous titanium chambers were tested in the AV loop model in order to allow additional extrinsic vessel ingrowth. 27 It was found that the extrinsic and intrinsic vascular pathways showed connections already at 2 weeks after implantation, making a transplantation of the entire construct using the AV loop possible.
The AVL technique has been also investigated in the context of TE of vascularised skeletal muscle. For example, it was demonstrated that transplantation of myoblasts into a previously vascularised fibrin matrix containing the AV loop enhanced cell survival and maintenance of the myogenic phenotype compared to fibrin matrices without AV loops. 61 More recently, a newly developed neurotised AV loop model has been established, referring to the used epigastric vein and saphenous artery and was therefore termed EPI-loop model. 22 Additionally, the obturator nerve was also implanted for neurotisation of the scaffolds. This technique was successful in showing myogenic differentiation of co-implanted myoblasts and MSCs with addition of bFGF and dexamethasone in the neurotised EPI AVL model.
In addition, it has been demonstrated that transgenic EPC expressing the antiangiogenic factor GBP-1 displayed reduced vessel directed migration in vivo in the AV loop, which confirms that this model, initially designed to generate vascularised biomaterials, may also serve as a highly sophisticated, sensitive and quantitative in vivo migration assay, helping to dissect cell functions in the state of inflammation and other disease conditions. 32
The isolation chamber setting with its potential to be monitored and manipulated may also be used as a platform to investigate the phenomena and regulation of angiogenesis and antiangiogenesis in cancer research. 5
Limitations to dimensions in small animal models have always been an argument against successful transfer of TE applications to clinical relevance.
Therefore, efforts have been focused on establishment of relevant large animal models. Beier et al. 57 have established a suitable large animal model (sheep) where de novo formation of axially vascularised tissue was demonstrated for the first time ever by sequential CT angiography and magnetic resonance angiography in vivo, as well as by post-explantational micro-CT and histology. 57 Using this approach, hydroxyapatite and beta-tricalcium phosphate as well as clinically approved processed bovine cancellous bone were axially vascularised using the AV loop large animal model.55,56 Furthermore, bone generation was induced using directly autotransplanted MSCs and rhBMP-2 stimulation in combination with a hydroxyapatite and beta-tricalcium phosphate matrix in clinically significant amounts. 53 The results of this investigation constitute a fundamental progress in approaching the first TE application of vascularised grafts with clinically relevant dimensions.
Conclusions
While initial TE techniques such as keratinocyte transplantation have left their eggshells and have been successfully applied to human diseases, most of the attempts to create functional 3D replacements for organ failure have not entered the clinical stage yet. Oxygen supply to the core of large TE constructs remains a critical issue for proper engraftment and integration to the human body. Hence, strategies of (pre-)vascularisation and optimisation of nutritional support by any means is one task that has to be mastered by future steps in furthering TE from bench to bedside. Extrinsic and intrinsic vascularisation are mechanisms that have to be revisited in this context. Because microcirculatory networks are complex in nature, the help of new technologies, such as organ printing with the help of jet based computer aided 3D TE, may help to improve the assembly of vascularised 3D soft organs and could accelerate organ maturation. There is no doubt that combined efforts from all fields of research, including developmental biology, material science and engineering as well as basic and clinical medical research will have to come together to tackle the prominent task of vascularising TE scaffolds. Many fine researches have been performed already, but still a huge amount of work needs to be carried out. Questions of material geometry and composition, printing devices that manufacture microchannels for fluid transport and which combine signal molecules and cell printing with advanced computer aided mechanisms, coculture of different cell types into customised templates as well as further combinations of microsurgical and TE techniques need to be addressed in the future. While some of these efforts still are in the research phase, without dispute, some therapies arising from TE and RM endeavours are about to enter the clinical stage, indicating that all combined efforts to improve the vascularisation of large or thick cultured grafts hold promise for the future.
Footnotes
Acknowledgements
This work has been supported by the Else Kröner-Fresenius Stiftung, AO Research Fund Grant no. S-10-36A, Baxter Healthcare Corporation as well as the University of Erlangen-Nuernberg (ELAN Program) and the ‘Emerging Fields Initiative’ of the University of Erlangen-Nuernberg (Project TOPbiomat). We would like to thank the Xue Hong and Hanns Georg Geis Foundation for their continuous support of research in Tissue Engineering and Regenerative medicine.