
Abstract
Keywords
Strengths and Limitations of this Study
The present article extends previous work published by the same first author and includes all relevant studies evaluating the various mechanisms of action of levonorgestrel-emergency contraception (LNG-EC). To our knowledge, this is the first paper which seeks to quantify the degree of pre-fertilization effect that may be realistically attributed to pre-ovulatory LNG-EC administration. This analysis was conducted in conjunction with a statistician.
The number of studies available for the analysis regarding the drug's ability to suppress ovulation is limited, and an ad hoc technique is used, e.g., using the median of 19 to denote the follicle size of 18 to 20. If the exact numbers are available, a linear regression model will actually be more informative. Because of the ad hoc method that we used and the limited sample size, we could not include other explanatory variables into the logistic regression model. For example, the follicle size and the conception probability could not be incorporated into the same model. Overall, this review is limited by the small number of studies available for analysis and the heterogeneity of the data. Although no studies are currently available which mimic in vivo conditions so as to settle the question of the drug's possible post-fertilization effect unequivocally, determination of early pregnancy factor (EPF) and its relationship to expected and recognizable conceptions might be a valuable tool to use in the near future.
Introduction
LNG is a potent synthetic progestin hormone which is contained in oral contraceptive pills and now widely used for EC. LNG-EC is taken either as a single 1.5 mg dose or as two doses of 0.75 mg 12 hours apart within 120 hours of unprotected intercourse, although it is most efficacious when taken within 72 hours (Cheng et al. 2008; Piaggio, Kapp, and von Hertzen 2011). The FDA label states that LNG-EC is “believed to act as an emergency contraceptive principally by preventing ovulation or fertilization (by altering tubal transport of sperm and/or ova). In addition, it may inhibit implantation (by altering the endometrium)” (Food and Drug Administration, FDA 2009).
Although LNG-EC is recommended to be taken at any time in the menstrual cycle, irrespective of when intercourse occurs, there is a “fertile window” of only 6 days during which the woman can become pregnant (Dunson et al. 1999). This window includes the 5 days before ovulation occurs, and the 1 day (24 hours) that the ovum (egg) can survive after ovulation.
Scientists have proposed that LNG-EC works in numerous possible ways: (1) by affecting cervical mucus, sperm transport, or sperm capacitance; (2) by delaying or inhibiting ovulation; (3) by preventing fertilization; (4) by altering early embryo transport in the fallopian tube; (5) by impairing corpus luteal formation (required for adequate progesterone production to support the endometrium); and (6) by decreasing endometrial receptivity, thwarting the embryo's implantation (Trussell and Jordan 2006; Croxatto et al. 2001). No direct test currently exists to identify fertilization of the egg by sperm, but it can be determined indirectly by a pregnancy test (hCG), that will not be positive until days after the embryo implants into the uterine lining, and EPF detection in the mother's serum (Morton 1984).
Official statements from the International Consortium for Emergency Contraception (ICEC), the Federation of Gynecology & Obstetrics (FIGO), and the American College of Obstetrics and Gynecology (ACOG) have repeatedly claimed that LNG-EC pills work with a dominant mode of ovulation suppression, asserting for example in multiple FIGO's statements that “inhibition or delay of ovulation is LNG-EC pills’ principal and possibly only mechanism of action” (FIGO 2011; International Federation of Gynecology & Obstetrics (FIGO) and International Consortium for Emergency Contraception (ICEC) 2012; ACOG 2014). Our findings confirm and extend earlier reviews of the topic suggesting that post-fertilization MOA of LNG-EC play a not negligible and possibly dominant role (Peck and Velez 2013; Mozzanega and Cosmi 2011; Kahlenborn, Stanford, and Larimore 2002).
Material and Methods
This article extends previous work published by the same first author (Peck and Velez 2013; Kahlenborn, Peck, and Severs 2015). Eligible articles were identified by an electronic literature review using the Cochrane Libraries (accessed in March, 2013) and PubMed (1970–January 2014) last accessed July 2014 with the assistance of a medical librarian experienced in systematic reviews. Inclusion criteria were: peer-reviewed journals, human subjects, and English language. Participants included women who had received LNG at usual doses used in vivo for EC in a clinical trial (cohort or RCT) or in vitro studies which exposed a specific target tissue to the drug (i.e., fallopian tubes, endometrial biopsies). We excluded efficacy and pharmacokinetic trials which did not seek to determine the MOA. Search terms included levonorgestrel, EC, mechanism of action, cervical mucus, sperm, fallopian tube, corpus luteum, and endometrium. Independent extraction of articles by five authors using sheets containing predefined data fields, including target tissue of MOA were utilized. The drug's effect on each target tissue was reviewed. A total of 2,425 titles were retrieved. After exclusion of duplicates and title review, 254 abstracts were reviewed for eligibility. Forty-one full text articles were then read in full and bibliographies hand searched for any missing studies. A total of thirty-eight studies were included, and six of these studies examined overlapping MOAs (i.e., ovulation and luteal effects).
The subsection on LNG-EC effects on sperm captured thirteen studies of which seven were retained. The excluded studies evaluated a different drug. The subsection examining LNG-EC effects on ovulation captured eleven studies of which ten were analyzed, and the quality of evidence was rated using adapted Oxford criteria (Daramola and Rhee 2011). One study was subsequently excluded because ovulation indicators were not assessed (Novikova et al. 2007). Ten studies were phase I; they were compiled (Table 1), and a logistic regression function was constructed to determine the relationship between follicle size (time to ovulation) and LNG-EC's ability to suppress or delay ovulation beyond 5 days. 1 This function was then used to estimate the ovulation inhibitory potential of the drug in the so far unique phase III study (Noé et al. 2011) (Table 2), whose implications seem not have been fully acknowledged.
Inhibition or significant delay of ovulation when LNG is taken on periovulatory days (number of women with no follicular rupture per number of women examined)
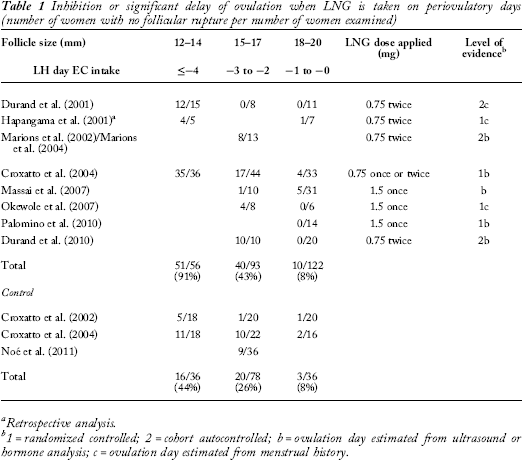
Retrospective analysis.
1 = randomized controlled; 2 = cohort autocontrolled; b = ovulation day estimated from ultrasound or hormone analysis; c = ovulation day estimated from menstrual history.
Percentage of pregnancies prevented by inhibition or delay of ovulation in 103 women receiving preovulatory LNG-EC a
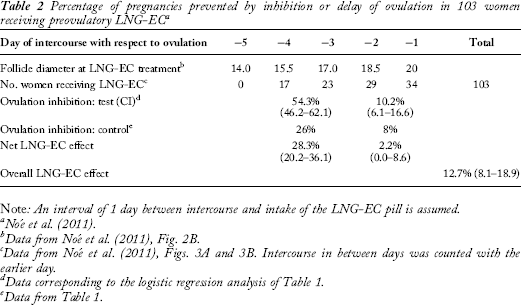
Note: An interval of 1 day between intercourse and intake of the LNG-EC pill is assumed.
Data from Noé et al. (2011), Fig. 2B.
Data from Noé et al. (2011), Figs. 3A and 3B. Intercourse in between days was counted with the earlier day.
Data corresponding to the logistic regression analysis of Table 1.
Data from Table 1.
The search on fallopian tube effects resulted in twelve studies pertinent to LNG-EC and tubal transport mechanisms, but the studies on LNG-IUS (intrauterine system) were excluded. LNG-EC on corpus luteum effects captured eleven studies of which two were subsequently excluded (Marions et al. 2002, 2004) due to the majority of patients being anovulatory and one study which had no controls (Massai et al. 2007). Three additional studies, one of which was a Cochrane review, reported luteal changes based upon anamnestic reports (i.e., bleeding), and so the methodology differed from the luteal indicators reported in Table 3.
LNG-EC studies which show luteal effects secondary to pre-ovulatory LNG
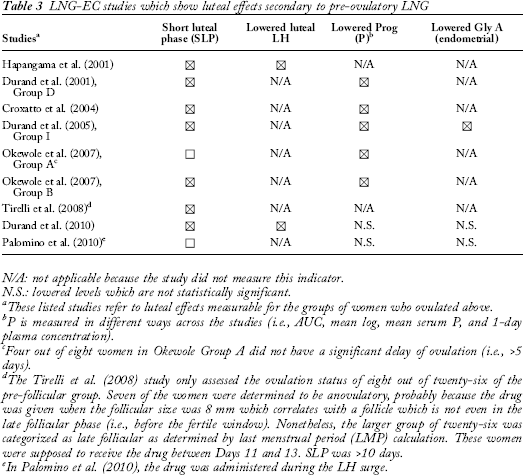
N/A: not applicable because the study did not measure this indicator.
N.S.: lowered levels which are not statistically significant.
These listed studies refer to luteal effects measurable for the groups of women who ovulated above.
P is measured in different ways across the studies (i.e., AUC, mean log, mean serum P, and 1-day plasma concentration).
Four out of eight women in Okewole Group A did not have a significant delay of ovulation (i.e., >5 days).
The Tirelli et al. (2008) study only assessed the ovulation status of eight out of twenty-six of the pre-follicular group. Seven of the women were determined to be anovulatory, probably because the drug was given when the follicular size was 8 mm which correlates with a follicle which is not even in the late follicular phase (i.e., before the fertile window). Nonetheless, the larger group of twenty-six was categorized as late follicular as determined by last menstrual period (LMP) calculation. These women were supposed to receive the drug between Days 11 and 13. SLP was >10 days.
In Palomino et al. (2010), the drug was administered during the LH surge.
There were certain studies in the ovulation and endometrial subsections which introduced a reporting bias which we have acknowledged in the text of the results.
Results
The evidence available for each of the above-mentioned MOAs will now be considered.
Cervical mucus effects, sperm transport, and capacity to fertilize
Sperm can live up to 5 days in the cervical crypts or the fallopian tubes, waiting to fertilize the ovum when released (Wilcox, Weinberg, and Baird 1995). Sperm survival is affected by changes in cervical mucus and the endometrial environment (Odeblad 1978). To be able to fertilize the egg when released, sperm must additionally undergo capacitance and the acrosome reaction (Crucker and Lipford 1995). In patients using long-term progestin only contraceptives (pills, implants), the decreased cervical mucus quality makes it inhospitable to sperm, and this is one main mechanism by which these drugs exert their anti-fertility action (Moghissi, Syner, and McBride 1973; Lewis et al. 2010). However, evaluating these agents alongside a one-time administration of LNG is not a valid comparison because the continual release of the drug from implants and daily administration of progestin only pills represent a very different environment than the emergency contraceptive one-time, oral post coital use (11).
Several studies have documented that sperm can be retrieved from the fallopian tubes within 5 minutes to 2 hours after insemination of semen in the vagina (Kesseru et al. 1974; Kunz et al. 1996; Settlage, Motoshima, and Tredway 1973; Ahlgren 1975). Kunz et al. note that spermatozoa are directed preferentially into the tube ipsilateral to the dominant follicle, thereby suggesting that there will be a preferential accumulation at the site of fertilization (Kunz et al. 1996). Suarez and Pacey have noted that the main functional human sperm-reservoir is in the fallopian tubes, where sperm which can maintain fertilization capacity are adhered to the endosalpingeal epithelium (Suarez and Pacey 2006).
In 1974, Kesserü showed that after a single dose of d-norgestrel, there was a modification of cervical mucus and a decrease of spermatozoa recovered from cervical and uterine fluid as a possible consequence of alkalinization which was manifest from 7 hours until 48 hours after LNG exposure (Kesseru et al. 1974). However, d-norgestrel at 400 mcg was used (which is different from LNG at 1.5 mg now used), and cervical mucus and sperm mobility were studied only from 3 hours after d-norgestrel administration up until 10 hours after drug exposure. While this study had been widely cited as evidence supporting LNG's contraceptive mechanism of action, recent studies contradict this view (Brito et al. 2005; Hermanny et al. 2012; do Nascimento et al. 2007; Yeung et al. 2002; Munuce et al. 2005; Bahamondes et al. 2003).
Specifically, a 2007 double-blind, placebo controlled, in vivo study demonstrated no impairment in cervical mucus after LNG was administered (do Nascimento et al. 2007). Viable spermatozoa were found in the genital tract 36–60 hours after coitus and 24–48 hours after LNG administration which is incompatible with sperm being killed within 7 hours by the induced alkaline milieu as suggested by Kesseru et al. (1974). The in vitro studies we reviewed found no significant effect of LNG on sperm function at doses which would actually be achieved in vivo (Hermanny et al. 2012; Yeung et al. 2002). The researchers noted the lack of effect on sperm from LNG at usual doses and postulated that the methodology of spermatozoa retrieval that the newer studies used was quite superior to the methods used in the older studies (do Nascimento et al. 2007).
Emergency contraceptive expert Gemzell-Danielsson noted that, “The observations described by Kesserü et al. of LNG effects on cervical and intrauterine mucus are probably of importance when LNG is used as a regular contraceptive but unlikely to be the main mechanism of action of LNG used for EC since sperm can be retrieved from the fallopian tube within five minutes after insemination of semen in the vagina” (Gemzell-Danielsson 2010).
In summary, according to available scientific evidence, LNG used at usual doses for EC has little or no effect upon cervical mucus or sperm mobility or capacitance and cannot explain LNG's effectiveness in avoiding pregnancy.
Prevention of fertilization
It has also been postulated that increased levels of glycodelin-A expression in serum and in human endometrium may result from peri-ovulatory administration of LNG, leading to decreased fertilization (Durand et al. 2005). However, do Nascimento et al. (2007) and Palomino, Kohen, and Devoto (2010) found no effect of increased glycodelin-A expression or inhibitory action on the ability of sperm to fertilize the egg, although Durand observed an increase in peri-ovulatory glycodelin (Durand et al. 2005), but noted that the levels were not high enough to explain an effect in vivo (Durand et al. 2010). Moreover, it has been demonstrated that glycodelin-A (which was found to inhibit fertilization in vitro) can be displaced from spermatozoa when passing through the oocyte-cumulus cell complex (Chiu et al. 2007). In other words, previous studies showing possible interference with glycodelin-A on sperm/egg binding, proved an event occurring only in vitro. The net effect of this interaction was that the “spermatozoa acquired enhanced zona pellucida binding ability” in vivo (Chiu et al. 2007). Thus, it is doubtful that the recent evidence regarding LNG-EC induced increase in glycodelin leading to impaired fertilization is a credible MOA.
Prevention of ovulation
Preliminary remarks
Inhibition or delay of ovulation has been claimed by leading emergency contraceptive experts and consortiums to be the principal mechanism of action of LNG-EC (Gemzell-Danielsson, Berger, and Lalitkumar 2013). This conclusion has been called into question earlier, though, by Mikolajczyk and Stanford (2007) using a computer simulation approach and by Mozzanega and Cosmi (2011) who analyzed seven related papers from prior to 2010. The present review synthesizes the available recent literature with particular reference to the large phase III clinical study (Noé et al. 2011). This study, together with the previous ones (Palomino, Kohen, and Devoto 2010; Durand et al. 2010; Croxatto et al. 2004; Durand et al. 2001; Marions et al. 2002; Marions et al. 2004; Okewole et al. 2007; Hapangama, Glasier, and Baird 2001; Massai et al. 2007), enables for a direct modeling of the relationship between follicular size, the time to ovulation, and the effects of LNG-EC, as proposed by Mikolajczyk and Stanford (2007).
In order to assess the role of ovulation inhibition, it is necessary to know the day with respect to ovulation when the LNG pill is ingested.
Currently, the gold standard to observe ovulation is a trans-vaginal ultrasound (TVUS) capturing follicular rupture (Severi et al. 2003). Follicular rupture is measured by tracking a dominant follicle and noting when the follicle collapses from one day to the next (follicular rupture = >50% collapse of the follicle). In lieu of detecting follicular rupture, other studies have relied on serum or urine hormonal levels of LH, estrogen, and progesterone to assess ovulation. However, determining the drug administration day before the LH surge has begun is difficult because it must be made retrospectively, using women's historical menstrual cycle data for estimations, which were very often inaccurate (Mikolajczyk and Stanford 2005). To circumvent these problems, some studies have tried to detect the rise of LH in serum or capture ovulation by ultrasound after administration of the EC pill and to determine whether ovulation occurred within or beyond the 5-day period following EC administration during which fertilization could take place.
Review of studies analyzing the inhibitory effect on ovulation after intake of the LNG-EC during peri-ovulatory days
Ten studies have been identified which examined the ability of LNG-EC to prevent or delay ovulation. Nine were phase I studies whose results are summarized in Table 1. Each of them included between 12 and 113 volunteers, who were either sterilized or were using non-hormonal methods of contraception during the study. Only one study was randomized, double blinded, and placebo controlled (Croxatto et al. 2004). Ovulatory dysfunction caused by the LNG-EC was considered no obstacle for fertilization. The reason is given later in this review.
As can be seen from Table 1, when given at the border of the fertile window, i.e., on day ≥ LH-4 (follicle diameter 12–14 mm), the LNG will inhibit ovulation in most women. If the pill is administered on day LH-3 or LH-2 (follicle diameter 15–17 mm) ovulation is inhibited in 43 percent of women, but also 26 percent of placebo-treated women fail to ovulate within the next 5 days. If the LNG is taken on day LH-1 or LH-0 (follicle diameter 18–20 mm), the rate of ovulation-inhibition becomes 8 percent compared to 8 percent in placebo-treated controls, i.e., the effect disappears. The application of a logistic regression model yields an ovulation inhibitory potential of 92.4 percent (84.5–96.5), 54.3 percent (46.1–61.2), and 10.2 percent (6.1–16.6) for follicle sizes 12–14, 15–17, and 18–20 mm, respectively.
Table 2 gives estimates for the ovulation inhibitory role in the prevention of pregnancies in the so far unique phase III clinical study by Noé et al. (2011). In this study, follicle growth in 148 women having received LNG-EC in their fertile period was tracked daily by ultrasound from the day of LNG-EC ingestion until ovulation occurred or for a maximum of 5 days. The pill was taken within 24 hours after unprotected intercourse by 64 percent of the women and later after, up to 120 hours, by 36 percent. For the purpose of this analysis, a convenient mean delay of 24 hours between intercourse and LNG-EC treatment is admitted. Noé et al. report that about 80 percent of the women ovulated within the expected range of days. Figure 3A and B from that paper (Noé et al. 2011) depicts the number of women who had unprotected intercourse on specific days in their fertile window and who were treated either before or after ovulation.
Taking these data and data from Table 1 as the basis, it is possible to calculate the fraction of pregnancies prevented by the ability of the drug to inhibit or significantly delay ovulation. As can be seen from Table 2, in this most recent and extensive study only 12.7 percent (8.1–19.8) of pregnancies are prevented by the inhibitory activity of the LNG-EC at the pituitary-ovarian level.
This contrasts to the reported effectiveness of 100 percent when LNG-EC was given on pre-ovulatory days. In order to explain the difference, Noé et al. referred to hypothetical effects on mucus quality and to the possibility of dysfunctional ovulation. The next paragraph will briefly address the latter of these arguments.
The Case of Dysfunctional Ovulation: A Review of Related Studies
In order to support a pre-fertilization effect for LNG-EC pills, Croxatto et al. postulated that even if ovulation could be demonstrated via follicular rupture, that ovulation would be “dysfunctional.” This important theory emerged in his 2004 study, in which he defines ovulatory dysfunction as follicular rupture not preceded by an LH peak or preceded by a blunted LH peak (<21 IU/L), or not followed by elevation of serum P over 12 nmol/L (Croxatto et al. 2004). Subsequent studies on LNG-EC MOA referred to this possibility (Noé et al. 2011; Croxatto et al. 2004; Massai et al. 2007).
Croxatto proposed that if the LH is deficient after the administration of LNG-EC, then the women who went on to ovulate had ova that were not able to become fertilized (due to the decreased LH levels). Although there were no LNG-EC studies that provided this evidence, Croxatto referenced the work of Verpoest when discussing his theory. The study by Verpoest involves a totally different population (i.e., infertile women) (Verpoest et al. 2000). Still more important, Verpoest's definition of fertilizable ova used was “the presence of two pronuclei at 24 hours and continued cleavage until embryo transfer at 2–3 days.” Thus, they define as unfertilizable ova embryos which cannot continue to divide properly, which is actually a post-fertilization event. Moreover, Croxatto and others have failed to realize that the addition of LNG-EC (itself a powerful progestin) would alter the proposed scenario of “low LH.” In fact, progestins have been shown in animal studies to promote oocyte maturation and meiosis resumption in the absence of an LH surge (Siqueira et al. 2012; Borman et al. 2004), which indicate (at least in animal studies) that the addition of LNG-EC (a progestin) would actually facilitate the ovulation process, even in the midst of a blunted LH environment.
In summary, two alternatives emerge with LNG given before ovulation: either a fully functional egg is set free despite a blunted LH peak, or pre-ovulatory drug-induced post-fertilization damage occurs to the embryo.
Despite the above data showing that LNG-EC pills do not work with a dominant mode of ovulation suppression, the official statements “How do levonorgestrel-only emergency contraceptive pills (LNG-ECPs) work to prevent pregnancy?” that were issued by the International Consortium for Emergency Contraception (ICEC) and the International Federation of Gynecology & Obstetrics (FIGO) in 2008, 2011, and again 2012 (FIGO 2011; International Federation of Gynecology & Obstetrics (FIGO) and International Consortium for Emergency Contraception (ICEC) 2012) assert that “inhibition or delay of ovulation is LNG-EC pills’ principal and possibly only mechanism of action.”
Two out of four of the statements’ authors, however, in their own studies, report and acknowledge that LNG can inhibit ovulation only when it is taken before LH levels rise, while it is quite ineffective when it is taken in the most fertile, pre-ovulatory days of the cycle (Croxatto et al. 2004; Massai et al. 2007).
Altered embryo transport through the fallopian tube
The tubal transport mechanism is essential for carrying the embryo to the uterus, so that arrival occurs within the narrow implantation window (days 20 to 24) (Norwitz, Schust, and Fisher 2001; Wilcox, Baird, and Weinberg 1999).
Although Cleland et al. found no clear relationship between the oral administration of LNG in EC and the increase in the number of ectopic pregnancies (Cleland et al. 2010), two previous studies report an increase in the likelihood of ectopic pregnancy. The first one finds a chance of ectopic pregnancy of 4.17 percent after administration of LNG in one or two doses (Von Hertzen et al. 2002), and the second shows an estimated probability of 4.11 percent, more than double that expected (Gainer, Méry, and Ulmann 2001). Moreover, in a more recent study published after Cleland et al., Lo and Ho (2012) noted an increased ectopic pregnancy rate of 2.3 percent after LNG-EC (3 in 128 pregnancies).
Two studies have analyzed the effect of LNG on tubal motility and epithelial ciliary beat frequency in vitro. In 2008, Wanggren et al. treated in vitro fallopian tubes obtained after hysterectomy with different products individually to observe their influence on tubal motility (Wånggren et al. 2008). One of the agents was LNG, which was added in two concentrations of 0.02 and 0.2 µM. That paper demonstrates that LNG reduces tubal motility—as measured by the area under the curve (AUC)—at least fifty times more efficiently than progesterone in comparable dose.
In a previous study, Mahmood et al. 1998 showed that high progesterone levels (10 µmol/L or higher), caused a significant reduction in the fallopian tube epithelial ciliary beat frequency. Given the higher affinity of LNG for progesterone receptors, its effects on fallopian tube epithelial ciliary beat frequency could be significant at the doses of LNG used in EC.
The tubal transport of embryos is slowed down by either mechanism, and this would have critical consequences on their nesting, as the narrow window might have been passed. This effect, coupled with the shortened luteal phase, as discussed in the next section, could preclude successful implantation.
Corpus luteum dysfunction
LNG-EC, when given in the pre-ovulatory period, has been demonstrated to have 100 percent efficacy in preventing clinical pregnancy and no effectiveness when given at or after ovulation (Novikova et al. 2007; Noé et al. 2011). From this it has been concluded that the drug has no post-fertilization effect. However, if LNG is given in the late follicular phase of the fertile window (before ovulation), it could alter LH secretion, decrease progesterone levels, shorten the luteal phase, and lead to aberrant vaginal bleeding (Soules et al. 1989). All of these findings would impair the embryo's ability to survive. Thus, pre-ovulatory drug administration could lead to post-fertilization effects. Table 3 summarizes this evidence.
Seven out of eight of these studies examined key luteal parameters after the drug was given pre-ovulatory. These findings were gathered from the groups of women who ovulated after receiving the drug in the late follicular phase. Hapangama showed decreased LH and a shortened luteal phase (Hapangama, Glasier, and Baird 2001). Durand et al. (2001) Group D, composed of eight participants in which the administration of LNG took place 3 ± 1 day prior to serum LH surge, exhibited deficient P4 production and significantly shorter luteal phase lengths following normal ovulation (Durand et al. 2001). Croxatto et al. reported significantly shorter cycles in 30 percent of the two-dose LNG and in 23 percent of the single-dose LNG women respectively, and found decreased progesterone concentrations in the LNG-treated cycles (Croxatto et al. 2004). Okewole's Group A treated on the day LH-3, had insignificantly delayed ovulation in half of the women, 2 but showed significantly lowered progesterone levels and increased vaginal bleeding; the six women (Group B) treated on the day LH-1, had a shortening of the whole cycle length (by 5 days), while the LH peak was only insignificantly delayed, suggesting a normal ovulation and a significantly shorter luteal phase with lowered mean progesterone levels (Okewole et al. 2007). These observations show that the occurrence of a blunted luteal phase is not restricted to cycles in which the ovulatory process is impaired, as some authors suggest (Gemzell-Danielsson, Berger, and Lalitkumar 2013).
Tirelli et al. reported that EC given before the LH surge significantly shortened cycle length in sixty-nine women by a mean of 11 days (Tirelli, Cagnacci, and Volpe 2008). Consistent with their 2001 paper, Durand et al. found that LNG delivered before the LH surge had significant effects on key luteal function parameters needed for implantation of embryos. Reduced progesterone levels, shortened luteal phases, blunted LH levels, and impaired luteal phase endometrial expression of progesterone-dependent glycodelin-A, were prominent findings of this serial research (Durand et al. 2005, 2010, 2001). Three final studies suggest that LNG-EC alters luteal function with respect to shortened luteal phase and increased vaginal bleeding (Cheng et al. 2008; Raymond et al. 2006; Gainer et al. 2006).
What is clear from these studies, the same quoted by the ICEC's and FIGO's statements in support of a dominant anti-ovulation MOA, is that inadequate or insufficient corpus luteum function occurs regularly in most women who ovulate after LNG-EC pills administration in the pre-ovulatory days, the most fertile days in the cycle, those in which most intercourse does occur and fertilization is most likely (Mozzanega et al. 2014).
These possible post-fertilization MOA are frequently ignored in recent work or reviews on LNG-EC. For example, data matching the length of the luteal phase with timing of pre-ovulatory LNG-EC intake are not available unfortunately from Noé et al.'s large phase III study (Noé et al. 2011), in spite of a significant shortening of the luteal phase being known from previous studies. Likewise, Brache et al. report on a significant reduction in mean highest P-levels after pre-ovulatory administration of LNG-EC at a follicle size ≥18 mm, but do not comment on this observation (Brache et al. 2013). Gemzell-Danielsson in her latest review (2013) emphasizes the pre-ovulatory MOA of LNG-EC and its lack of effect on implantation, but does not discuss the evidence concerning luteal phase defects.
Endometrial effects/implantation studies
Several early histology studies showed that LNG-EC given in the follicular phase led to insufficient luteal function or abnormal histology (Landgren et al. 1989; Spona, Matt, and Schneider 1975; Ugocsai, Ròzsa, and Ugocsai 2002). Vargas et al. (2012) gave LNG-EC on the first day of the luteal phase and determined that endometrial receptivity molecules were not affected by LNG-EC administration. However, since LNG-EC is not efficacious at or after ovulation (Noé et al. 2011; Novikova et al. 2007), this study is not able to answer the question of whether LNG-EC given pre-ovulatory has endometrial effects.
A study by Palomino showed that LNG-EC given at LH surge did not affect endometrial receptivity proteins, but did alter histology. In that study, “the endometrial biopsies from the LNG-EC treated subjects administered by the oral route showed areas of irregular development that were characterized by glandular atrophy and intense stromal decidualization” (Palomino, Kohen, and Devoto 2010).
Durand et al. (2001) studied endometrial biopsy specimens obtained from all her thirty-three patients 9 days after the LH surge. The twenty-four biopsies evaluated and considered normal came almost entirely from the Groups B and C (which were the women who received LNG at or after the LH peak), while nine specimens from women who received LNG 3 to 4 days before the LH peak and ovulated were out of phase or insufficient and were excluded. Thus, the findings of normal endometrial histology in women given LNG at or after ovulation does not answer the question of whether pre-ovulatory LNG effects endometrial histology. Moreover, when re-analyzed in the 2005 study, the “histologically normal” endometria from Durand's 2001 Group D in fact showed decreased glycodelin-A, a necessary endometrial implantation molecule (Durand et al. 2005).
Not surprisingly, the study by Marions in 2002 evaluated pre-ovulatory LNG-EC on endometrial histology and pinopodia and concluded that there was no effect on endometrial receptivity but that three out of six biopsies were “out of phase” (Marions et al. 2002). Two studies by Meng were carried out to determine if LNG-EC could alter endometrial receptivity markers (Meng et al. 2009, 2010). The 2009 study sampled endometrial biopsies from women on days LH +4 to +5 using a three dimensional endometrial construct and found that LNG-EC exposure in the luteal phase did not alter endometrial receptivity factors, but the women were never given LNG-EC during the fertile window (Meng et al. 2009). The 2010 study administered LNG-EC repeatedly either orally or vaginally on days LH +1 to LH +4 and examined endometrial receptivity markers on days LH +6 to LH +8. They found that the group receiving the oral regimen had minor alterations in their markers, but were given the drug at or after ovulation when the drug is likely to be ineffective (Meng et al. 2010).
Lalitkumar created an artificial tridimensional endometrial model and studied the differences of human blastocysts implanting in LNG-exposed tissue as compared to controls (Lalitkumar et al. 2007). As expected, in these normal endometrial samples (collected from women who had not been given LNG in their fertile days), there was no measurable difference in the implantation rate compared to controls, suggesting that exposure of secretory endometrium to artificial gestagen does not affect endometrial function. What these studies can say is that LNG, when taken 5–6 days following fertilization at the moment of implantation, does not affect its evolution. But this is not the typical time when EC is usually administered (Mozzanega and Cosmi 2011).
Thus, in conclusion, the methodology of many of the histological and endometrial analyses performed to explore LNG-EC's effect on endometrial receptivity and implantation was inadequate to answer the question of LNG-EC's pre-ovulatory use leading to post-ovulatory changes.
Conclusion
Much of the published scientific information relating to EC in general and LNG (LNG-EC) in particular, has strongly and repeatedly insisted that the main mechanism of action of these drugs, if not the only one, is to inhibit or delay ovulation. The therapeutic guidelines used in family planning which have been provided by scientific societies have likewise stated that there are no post-fertilization mechanisms that could raise ethical objections to the use of LNG-EC.
Our analysis strongly suggests that pre-fertilization activity of the drug could, in a routine clinical setting, prevent less than 15 percent of expected conceptions. The drug has minimal effects on cervical mucus or sperm functions and has limited ability to prevent ovulation on the most fertile days of the cycle. However, pre-ovulatory drug administration can lead to post-fertilization luteal effects (such as lowered progesterone, LH, glycodelin levels, shortened luteal phase, and altered endometrial histology) and may explain its clinical efficacy when used before ovulation.
In conclusion, LNG-EC administration during the pre-ovulatory days, the most fertile in the cycle, cannot prevent ovulation or fertilization with a dominant pre-fertilization MOA, but can be demonstrated to impair luteal function and may adversely affect the survival of the embryo.
This information should be made available to users of LNG-EC so that they can make their choice based on informed consent.
Footnotes
Biographical Note
Rebecca Peck, M.D., is a clinical assistant professor at Florida State University, College of Medicine, Daytona Beach, FL.
Walter Rella, M.D., is a family practitioner, Institut für Medizinische Anthropologie und Bioethik (IMABE), Wien, Austria.
Julio Tudela, Pharm.D., Ph.D., is a member of the Observatory Bioethics of the Catholic University of Valencia and professor at the Catholic University of Valencia, Spain.
Justo Aznar, M.D., Ph.D., is a director of the Life Sciences Institute of the Catholic University of Valencia, Spain.
Bruno Mozzanega, M.D., is a professor of gynecology in the Department of Woman's and Child's Health, University of Padua, Obstetrics and Gynecology Unit, University of Padova, Italy.
Acknowledgements
The authors thank Shaobo Jin, Ph.D. candidate, Department of Statistics, Uppsala University, Sweden, for his contribution to the statistical analysis and treatment of the data.
1
Due to the small number of studies, the controls from one study (Croxatto et al. 2002) were pooled with the other controls (Noé et al. 2011; ![]() ) since the methodologies were the same.
) since the methodologies were the same.
2
In Okewole's study, only four out of eight women had a “significant” delay over 5 days. Okewole reported that the women in Group A had a significant delay in LH peak by about 96–120 hours compared with their control cycles, but this finding was a reported mean value based on all eight subjects. So, for example, in subject 7, her delay in LH surge was as small as 1 day, and subject 4 had a 2-day delay. The mean reporting measure obscures these findings.