
Abstract
Objectives:
To identify the continuity mechanisms central to a smooth transition from child to adult diabetes care, the service components through which these can be achieved and their inter-relations in different contexts.
Methods:
A realistic evaluation study of five models of transition in England comprising: organizational analysis (semi-structured interviews with 38 health care professionals and selected observations); case studies of 46 young people under-going transition and 39 carers (three qualitative interviews over a 12-18 month period, medical record review and clinical interviews); surveys of 82 (32% response rate at least once and 11% response rate at two time points) young people in the population approaching, undergoing or less than 12 months post-transition, and their carers (questionnaires included psychosocial outcome measures); and a costs and consequences analysis.
Results:
Seven continuities contribute to smooth transition: relational, longitudinal, management, informational, flexible, developmental and cultural. Relational, longitudinal, flexible and cultural continuity are the most important. Models with high levels of relational, longitudinal, flexible and cultural continuity achieve smooth transition with relatively informal, low-cost informational and management continuity mechanisms. Models with low levels of relational and longitudinal continuity need to invest in more formal interventions to facilitate management, flexible and informational continuity so that smooth transition is not compromised.
Conclusions:
Focusing on continuity mechanisms, their inter-relations and the effectiveness of different constellations of service components in achieving smooth transition has furnished evidence to inform the development of innovative models which build on the logic of these findings but are sensitive to local context. Further studies are needed to confirm the quantitative findings from a broader range of services and patients.
Introduction
During adolescence many young people with diabetes experience deterioration in their condition.1-3 This is attributable to the physiological changes associated with puberty and psycho-social changes at this stage of the life-course. Confounding these challenges is their co-occurrence with transfer from child to adult services.
4
High rates of non-attendance by young people at clinic appointments have been reported after transfer to the adult service
4
and less frequent clinic contact has been linked to poorer blood glucose control.
5
The United Kingdom National Service Framework (NSF) for Diabetes states that: ‘all young people with diabetes will experience a smooth transition of care from paediatric diabetes services to adult services’.
4
However, whilst there is professional consensus on best practice,4,6 there is little research evidence to inform service commissioning. This paper summarizes findings from a realistic evaluation
7
study designed to address this gap in understanding. The study objectives were to:
Develop a typology of diabetes transition models, building on previous research on continuity of care; Identify users'/carers'/providers’ experiences of, and preferences for, transition services, the processes and organizational challenges involved and assess costs; Identify what works best to promote ‘a smooth transition’, for whom and in what circumstances.
Method
Theoretical Framework
Realistic evaluation 7 is an alternative approach to experimental methods for researching models of health care. 8 The primary concern is not with producing a pass/fail verdict but with identifying what produces a particular effect. The intention is to develop an understanding of associations between variables by identifying the mechanisms producing an outcome. Continuity of care is the mechanism central to current concerns about ‘smooth’ transition. Forbes et al. 9 identify seven relevant continuities: experienced, information, cross-boundary, flexible (adjustment to individual need), longitudinal (care from as few professionals as possible), relational (therapeutic relationship with a named professional) and developmental (care which reflects and facilitates changing needs). These were used as an initial orienting framework and informed data generation. Our concern was to establish which continuities contributed to smooth transition, their inter-relations and the effectiveness of different constellations of service components in achieving smooth transition in different organizational contexts.
Sample
Diabetes services in England were surveyed to inform the development of a typology of transition models for sampling purposes. The instrument included questions about context and structure, mechanisms for transfer and organizational practices. It was administered to a 20% random sample of providers in the Directory of Diabetes Care. 10 Sampling continued until no new service arrangements were identified.
Service features were categorized according to the primary continuities they were designed to effect. This revealed overlap between Forbes et al.'s concepts making it difficult to assign service components to a single continuity mechanism. 9 Therefore the original framework was simplified with analysis based on three paired continuities: relational/longitudinal, informational/cross-boundary and developmental/flexible. Services were discriminated by the extent of developmental/flexible continuity practices and the stages in the transition process (the number of clinic interfaces between paediatric and adult services). Combining structural characteristics (one, two or three stages) with process characteristics (presence of developmental/flexible continuity interventions) produced a typology of six service models. 11
On the basis of this typology, a sample of six models would be required to cover the spectrum of services. However, the survey revealed a strong trend towards sequential transition (two or more stages) and the few identified examples of direct transition intended progressing to a sequential model. Therefore no examples of direction transition were included. The final sample comprised services representing the four remaining examples in the typology and a further two three-stage models with additional interesting features: one where transition entailed the management of an organizational interface between a children's hospital and adult hospital and one because it provided an integrated service for adults up to 40-years-old. The latter model withdrew from the study.
Five models were included in the evaluation. Model 1 has three stages and is operated by a regional children's hospital and a foundation hospital trust. Model 2 has three stages and is provided by a large city-based trust. Model 3 is a two-stage service delivered by a small integrated team located in a medium sized trust. Model 4 is a three-stage service provided by a foundation trust in which child and adult services sit within a single directorate. Model 5 has two stages and is provided by district general hospital. Diagrams and narrative summaries of each model are available in the full study report. 11
Design
Organisational analysis
Semi-structured interviews with providers (n = 38) yielded information on service configuration and resource inputs for each model. Interviews were audio-recorded or transcribed as contemporaneous fieldnotes. Selected observations provided contextual information. Model descriptions were verified with respondents and hypotheses formulated regarding their continuity mechanisms and service components.
Case studies
Case studies were undertaken with young people with type 1 diabetes undergoing transition (n = 46) and their carers (n = 39). Cases were stratified by gender and purposively selected to represent the full spectrum of each model. The desired sample size (12 per model) was not achieved, however, and did not include cases across the full transitional period in all models. Case study sample details for each model are available as appendices in the full report. 11
Interviews were conducted on three occasions over 12–18 months designed to elicit experiences of diabetes and perceptions of the service. The latter interview schedules were modified to reflect the emerging analysis. The final interviews tested the hypotheses for each model and the study as a whole. The first and third interviews (1 hour) were face-to-face and the second (30 mins) by telephone. In addition, medical record reviews were combined with clinical interviews (n = 38) to build case profiles and verified by service users. These informed the evaluation of each model and were taken into account in the analysis of users'/carers’ views to ensure these were interpreted in context.
Survey
Parallel surveys of young people with type 1 diabetes, approaching, undergoing or less than 12 months post-transition and their carer were administered. The young person questionnaire included the Healthcare Climate Questionnaire (HCCQ), the Diabetes Continuity of Care Scale (DCCS), the Patient Enablement Instrument (PEI), the Diabetes Management Self-Efficacy Scale (DMSES) and the Diabetes Quality of Life measure for Youth (DQoLY). The instruments were selected following a systematic review of the literature. 11 The carer questionnaire included the HCCQ, DCCS, the Perceived Competence for Diabetes Scale (PCDS) and the Short Form 36 (SF36).
The survey was administered at two time points to the same sample, but the number responding both times was small (82/739 = 11%). Both time points were therefore combined with one questionnaire randomly selected for those who had responded twice. Results were split by completer and type of clinic attended. Regression analyses were performed for the DQoLY and HCCQ scales for young people. Explanatory variables included age, gender, type of clinic (children's clinic as the reference category) and continuity descriptors specific to certain models developed from the qualitative analysis. For carers, regression analyses were performed for selected SF36 scales and the PCDS. Explanatory variables comprise those included in the young people's analysis, along with a variable indicating if the carer attended consultations with their child. 11 Given the low response rate, the aim of these analyses was to assess if the quantitative data supported the qualitative findings.
Costs consequences analysis
Service providers were asked to identify transition activities, and for each report the number and grade of staff involved and the hours per week devoted by each staff member, including travelling time. Total costs were converted to per patient costs using the number of patients registered with the service at the beginning of the study. (Unit costs and sources available 11 ).
A societal perspective was adopted for indirect costs which included use of other NHS resources including hospital admissions, A&E attendances and all contacts with health professionals plus costs borne by the young person/carer. Data were provided by case study respondents at each of the three interviews. Questions related to what had occurred during the previous three months. This provided cost data for a total of nine months reported as an average cost/patient per month. As case study participants represent a small proportion of those receiving care in each model, costs are indicative. Costs are reported in 2009 prices inflated where necessary using the Department of Health pay and prices inflation indices. As all costs are within one year no discounting has been applied.
Ethics
The survey was determined to be pre-research activity and not require ethics or research governance approval. NHS Research and Development Office and Research Ethics Committee approvals were received for the realistic evaluation (05/MRE08/90).
Results
Results from the provider interviews, case studies and survey were combined to consider the contribution of continuities to smooth transition, the relationship of continuities to psychosocial outcomes, service components’ effectiveness in achieving continuities and their inter-relations in achieving smooth transition in different contexts, and the costs and consequences of each model. While Forbes et al.'s continuity concepts 9 provided a useful orienting framework, this was limited by the quality of the literature from which it was derived, the dearth of research focusing on the young person's perspective 12 and the lack of a specific focus on transition in diabetes. As a result of preliminary data analyses and taking into account more recent literature,13,14 this was modified and used to analyse the five service models.
Forbes et al.'s original definition of ‘experienced continuity’ as the experience of a coordinated and smooth progression of care from the service users’ point of view (i.e. smooth transition) was retained and seven further continuities identified: relational (an ongoing therapeutic relationship between patient and one or more providers 14 in which health care professionals understand the fabric of individual's lives), longitudinal (uninterrupted relationships with service providers over time, consistent with need 13 ), management (continuity of diabetes management consistent with needs through a common purpose and plan 14 ), cultural (seamless progression from a child to adult service culture across service interfaces), flexible (care responsive to the needs of young people and families), developmental (care that proactively facilitates the transition to adulthood and/or adult services and supports young people to develop physically, psychologically and socially) and informational (provision of information to prepare young people and families for transfer and new service arrangements).
Organisational analysis
Relational and longitudinal continuity
Relational and longitudinal continuity emerged as the mechanisms central to smooth transition. Most young people and carers preferred to be seen by a professional with whom they had a therapeutic relationship, and a smaller number appreciated familiarity of service provider but wanted more detached associations. Respondents indicated that relational/longitudinal continuity promoted flexible continuity, as care could be tailored to individual need and any episodes of deterioration in control were understood in the context of the individual's care trajectory, rather than as ‘non-compliance’. Relational/longitudinal continuity also provide a sense of safety at times of change. Where these continuities were sustained, young people and carers were able to negotiate service interfaces and cope with other changes with relative ease. In models with high levels of relational/longitudinal continuity but limited informational continuity, families were still relatively relaxed about transfer (models 3, 5) but where a complete change of care provider occurred, families’ needs for information increased (models 1, 2). Relational/longitudinal continuity also facilitated management continuity.
Management continuity
Continuity of diabetes management can be sustained by informal low-cost communication systems in models with small co-located teams and high levels of relational/longitudinal continuity. In more complex divisions of labour and lower levels of relational/longitudinal continuity, additional management continuity mechanisms are required. Formal written communication was a key management continuity feature in models where young people transferred to the care of a new consultant; however the content tends to be exclusively clinical and experiences of transition are deeply embedded in psychosocial understanding, which is why relational/longitudinal continuity are so important. Whereas nursing teams appeared to operate in a consistent fashion and work interchangeably if necessary, team-based approaches in medical care seemed more difficult to achieve although this was more problematic in some models than others. This appears to be partly because of the need to accommodate transient members such as trainee doctors or locum staff and partly because of the strong ethos of professional autonomy in medicine.
Carers contribute to management continuity, but this is not formally recognised. Children's services all provided high levels of family support which was highly valued and enabled carers to access information to make decisions about their child's diabetes management. Only in model 3 in which there was already an established relationship with the diabetes specialist nurse did carers feel able to make contact with providers after the young person had moved into adult services. In other models many mothers experienced management discontinuity particularly when their child attended consultations alone. 15
Cultural continuity
The sample included culturally continuous and discontinuous models. Where paediatric and adult services were culturally continuous (models 2 and 3), transition was relatively seamless and there was little need for interventions to prepare for transfer. At the time of the study, model 1 was culturally discontinuous but a newly appointed transition nurse spanning both services had facilitated greater cultural understanding and there was evidence that the role would foster future cultural integration. Routine contact between services cannot guarantee cultural continuity, however. Despite a long history of joint working and high levels of structural integration between services, model 4 demonstrated marked cultural differences between paediatric and adult services. Clinical leadership and a commitment to adolescent health appeared to be the additional active ingredient in those services exhibiting highest levels of cultural continuity.
Informational continuity
Each model had different requirements for informational continuity. In those with high levels of relational/longitudinal continuity across service interfaces, young people and carers were able to make a smooth transition in the absence of formal informational continuity (model 3). However, in models with a complete change of service provider at transfer to adult care, informational continuity was more important (models 1 and 2). In model 1, information leaflets were produced by the paediatric service, but these were based on stereotypes of adult services and did not include specific information on the new arrangements for care. Families in this model expressed the highest levels of anxiety about transfer.
Flexible and developmental continuity
In all models service providers modified their approach to young people to encourage greater independence. This entailed engaging with young people directly rather than through carers, until they eventually began to consult on their own. In some models this was proactively encouraged (models 2, 3 and 5) in others, staff left the decision to families (models 1 and 4). Consultation style and interpersonal skills were highly consequential for the experiences of young people. In model 4 young people entered a joint adolescent clinic aged 13 in which there were few concessions to age and experienced negatively adult approaches.
All models recognised that young people who had transferred to adult services required high levels of access and support and there was a diversity of arrangements designed for this purpose: more frequent clinics, access to on-call nurses and email mentoring. There was little formal education in any model, although staff aspired to develop this component of the service. However, whereas carers viewed formal education favourably, young people were less enthusiastic. Most were reluctant to attend events beyond routine clinic appointments and few expressed a desire for peer-based support.
Beyond these broad similarities, the models had subtly different combinations of developmental and flexible continuity. Models with less flexibility of transfer and a complete handover of care to adult providers placed greater emphasis on developmental continuity (models 1 and 2) centred on the so-called ‘risk’ issues: alcohol, pregnancy, drugs etc. Whilst providing certain assurances about their preparedness to leave children's services, there is less scope for young people to set the pace of their own development than in those models which had greater flexibility about the timing of transfer and where there could be a greater emphasis on flexible continuity. Young people and carers value the ability of health care professionals to anticipate future needs but they prefer for this to be individually determined.
The effectiveness of service components in achieving service continuities is summarised in Table 1 (see online only supplement: http://jhsrp.rsmjournals.com/lookup/suppl/doi:10.1258/JHSRP.2011.011044/-/DC1).
User and carer surveys
Of 739 users approached across all models, a total of 234 young people responded at least once to the survey (a response rate of 32% and 11% at both time points). This response rate ranged between models, from 24% (model 4) to 42% (model 2). A total of 31% (230) carers responded at least once.
In order to assess whether continuity of care was associated with psychosocial outcomes we categorised models according to whether they exhibited high levels of the continuities indicated by the qualitative data to be most important in achieving smooth transition. Model categorization is given in Table 2 (see online only supplement: http://jhsrp.rsmjournals.com/lookup/suppl/doi:10.1258/jhsrp.2011.011044/-/DC1). Because they are so closely related, for the purposes of the regression analysis, relational and longitudinal continuity were combined. Not all qualitative descriptors were included in the regression model due to redundancy: management continuity (high levels of management and high levels of cultural continuity are present in models 2 and 3) and information continuity (high levels of informational and high levels of relational/longitudinal continuity are present in model 3). Results of the surveys are presented in Table 3, where arrows pointing upwards indicate significantly (at the 5% level) higher scores with the corresponding factor present. Arrows pointing downwards indicate significantly lower scores with the corresponding factor present, with no arrow an indication of a non-significant finding. Detailed regression estimates are available in the study report. 11
Regression analysis for young person and carer scales
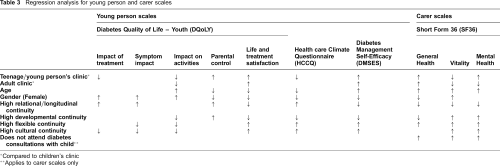
Compared to children's clinic
Applies to carer scales only
In models with high levels of developmental continuity respondents reported significantly higher parental control scores, lower impact on activities scores and lower life and treatment satisfaction scores. Satisfaction with the service and self-efficacy scores, were also significantly lower in young people consulting in models with high levels of developmental continuity and carers reported significantly lower general health scores and higher vitality and mental health scores. Young people consulting in models with high levels of flexible continuity reported significantly lower symptom impact and impact on activities scores, with significantly higher life and treatment satisfaction scores, and higher health care climate and diabetes management self-efficacy scores, whereas carers reported significantly higher general health, vitality and mental health scores. These findings suggest that models with high levels of flexible continuity have more positive outcomes than those with a predominantly proactive approach (developmental continuity).
Where relational and longitudinal continuity were high, young people reported significantly higher health care climate, impact of treatment, symptom impact and parental control quality of life scores and significantly lower life and treatment satisfaction scores and lower self-efficacy scores; carers reported significantly lower general health, vitality and mental health scores. Whereas the higher health care climate scores appear to support the qualitative findings, other outcomes associated with high relational continuity are more difficult to interpret and possibly counter-intuitive. One explanation might be that closer user-professional relationships stimulate greater self-awareness of diabetes and its management.
Users consulting in models with high levels of cultural continuity reported significantly lower impact of treatment, symptom impact and impact on activities quality of life scores. Life and treatment satisfaction, health care climate and self-efficacy scores were higher in users who consulted in models with high levels of cultural continuity and carers reported higher vitality and mental health scores.
Costs consequences analysis
Results are reported in Table 4. Per patient costs were highest in model 1 (£139) and relatively low in models 3, 4 and 5 (between £31 and £39). Mean monthly cost per patient of other NHS services ranged from £3.95 (model 2) to £15.42 (model 3). These low mean costs are due to most patients not having used any services during the reporting period. The samples were too small to attempt any statistical analyses of differences in these costs between models. Mean user-borne costs were low in all cases.
Monthly costs per model
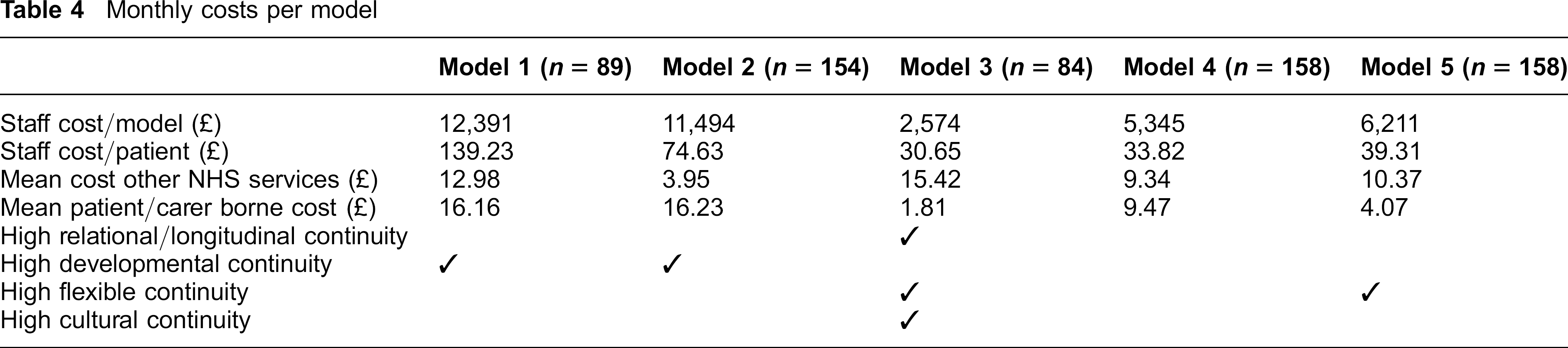
Table 4 also shows a summary of results in terms of the continuities featured in the regression analyses. Model 1 had an emphasis on developmental continuity. Its high costs were largely due to the high input by Diabetes Specialist Nurses (DSNs). Developmental continuity was also a feature of model 2 which also had high staff costs but lower costs per patient due to the higher number of patients cared for. Model 3 is characterized by high levels of relational/longitudinal, flexible and cultural continuity but had the lowest reported cost per patient suggesting smooth transition can be achieved in models exhibiting these features without the need for formal and more costly informational, management or development continuity interventions. Model 4 was not categorized as achieving high levels in any of these continuities. Finally, model 5 was categorized as exhibiting high levels of flexible continuity. It had a different combination of health professionals to the other four models including Community Children's Nurses (CCN)s, a staff nurse and with a small input by a health care assistant. The CCNs contribute just over half of the total professional input to this service (53%) lending evidence to the perception that the children's service was subsidising adult service provision.
Discussion
What works?
Seven continuities contribute to smooth transition: relational, longitudinal, informational, management, cultural, developmental and flexible. Relational and longitudinal continuities are the mechanisms central to transition because they also facilitate management and flexible continuity. They also provide a sense of safety at times of change, obviating the need for informational continuity interventions. Flexible and cultural continuities also emerge as important. We have considered the effectiveness of different service components in achieving these continuity mechanisms and how these inter-relate in achieving smooth transition in particular contexts (Table 1).
For whom?
There were high levels of agreement between young people and carers across all models about the mechanisms central to smooth transition and within models about the relative success of service components in achieving smooth transition. Mothers are an important source of continuity, but this is not formally recognised in policies in this field. Whilst the progression to lone consulting was a key developmental milestone for young people, many mothers felt cut off from the process and could no longer access the advice they needed to support their child. This is the primary area where what works for young people, does not work for carers.
In what circumstances?
Models with high levels of relational, longitudinal, flexible and cultural continuity are able to achieve smooth transition with relatively informal, low-cost informational and management continuity mechanisms. Models with low levels of relational and longitudinal continuity need to invest in more formal interventions to facilitate management, flexible and informational continuity to ensure smooth transition is not compromised. Models in which there is a complete transfer of responsibility at the child-adult interface are most costly because of the emphasis given to developmental continuity interventions and the need for arrangements which support handover of care.
There is relatively little empirical research on continuity of care in transition. However, two relevant reports were produced at the same time as the present analysis which strengthen our findings. Nakhia et al. 17 undertook a retrospective cohort study of 1507 young people with type 1 diabetes up to the age of 20 over a four-year-period. Five different models of transition were assessed. After controlling for confounding factors, young adults were 77% less likely to be hospitalised after transition if their physician had not changed compared with those who had been transferred to a new physician (relative risk, 0.23; 95% CI interval = 0.05 to 0.79). Although their original study design does not provide any explanation for this relationship, our findings suggest that continuity of physician is likely to act as a mechanism for relational and longitudinal continuity and therefore management, cultural and flexible continuity. As such, this offers further evidence of the centrality of these continuity mechanisms to achieving smooth transition. The findings of our study also resonate strongly with those from Parker and colleagues’ literature synthesis and conceptual analysis of continuity of care 16 and particularly their observations about patients’ desire to be dealt with in a wider context that acknowledges their life situation and the attention they draw to the neglect of carers in this field.
Methodological considerations
One of the strengths of realistic evaluation is that it focuses on generative mechanisms rather than service structures, producing insights which enable responsiveness to local operating constraints rather than ‘one size fits all’ recommendations. Moreover, by utilizing a range of data types we have been able to identify the continuities that contribute to smooth transition from the perspective of young people and their carers, the psychosocial outcomes associated with different kinds of continuity, the inter-relationships between different kinds of continuity and different service constellations, the trade-offs inherent in particular models and their resource implications. Nevertheless, there is rarely a direct relationship between a continuity mechanism and a single service component, which is why a simplified framework was used for the survey. For the purposes of the in-depth evaluation, a more detailed framework was necessary, though the problem of overlap remains and for ease of exposition we report closely related continuities together. Another challenge is that it is not always clear whether continuity of care is an outcome or a process. 16 In this study, experienced continuity was treated as an outcome and the other continuities conceptualized as generative mechanisms which interact to produce that outcome, or not as the case may be. However, each continuity mechanism is itself an outcome of a service component or components. Accordingly the question of what works, for whom and in what circumstances has to be addressed to two dimensions: the continuities most important in achieving smooth transition and the service arrangements most effective in achieving these continuities.
No service had well-defined boundaries which complicated estimation of costs. Time spent on transition had to be disentangled from that devoted to normal care. The absence of dedicated resources meant that costing had to be restricted to staff costs. Recruitment also proved challenging. We did not succeed in recruiting cases which spanned the full transition period in all models and so were unable to evaluate some service components. Similar challenges were faced with the survey. The sample size for the regression analysis across models is adequate for the number of explanatory variables, but caution is needed in terms of generalizability because of potential biases due to the low response rate (32%) and there was little information on non-responders in order to assess the potential biasing factors. Nevertheless the results were supportive and helped to develop a greater understanding of the potential mechanisms and impacts of different types of transition. However, further quantitative work is indicated to explore the relationship of continuities to these and a wider range of clinical outcomes.
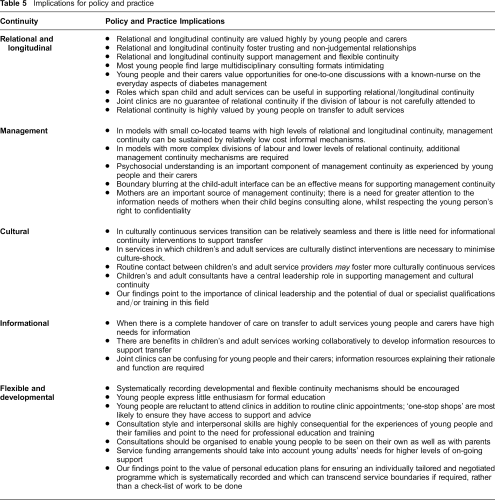
The majority of young people in our sample attended clinic regularly and had positive relationships with carers. We do not know to what extent these findings can be extended to young people who are poor clinic attenders and/or have strained familial relationships. This is an area where further research is indicated, firstly to develop and test methodologies for accessing hard to reach groups and secondly, to examine their reasons for non-attendance and their needs from the service. Of all the concepts in our conceptual framework, developmental and flexible continuities are the least well-developed and the most difficult to map on to specific service components. Given the breadth and variety of young people's lives there are clear challenges involved in achieving a balance between proactive developmental continuity interventions and responsive flexible continuity interventions. Further research is indicated on how to best meet the support needs of young people at this stage of the life-course. Cultural continuity was a new concept developed for the purposes of this research and was associated with more positive outcomes but questions remain as to how this can be fostered. The implications of our findings for policy and practice are summarized in Table 5.
Implications for policy and practice
Conclusion
This study has identified the continuity mechanisms central to achieving smooth transition and the constellation of service components by which smooth transition can be achieved in different contexts. There would be value in building on this work to develop validated measures of service continuity so that their relationship to clinical outcomes can be examined statistically. By focusing on continuity mechanisms rather than service structures we leave open the possibility of innovative approaches to managing transition or modifications to existing models which build on the logic of our findings and sensitive to local context and which could be evaluated through a randomized controlled trial.