
Abstract
Background
Inner ear malformations may cause sensorineural hearing loss (SNHL). However, the correlation between the small lateral semi-circular canal (LSCC) and SNHL is controversial.
Purpose
To determine whether there is a correlation between the two using CT-based measurement.
Material and Methods
We retrospectively reviewed the high-resolution CT images of the temporal bone obtained from consecutive patients. A total 136 ears of 68 patients (25 men and 43 women; age range 20–85 years, mean 49.8 years) were included in this study. Patients who were clinically suspected to have otosclerosis were also excluded. Two radiologists independently measured the width and cross-sectional area of the bony island of LSCC. We evaluated the correlation between LSCC bone island width or cross-sectional area and hearing level in all cases using Pearson correlation co-efficients. In addition, we compared hearing levels among the patient group with normal-sized LSCC (≧mean-SD), small LSCC (<mean-SD) and very small LSCC (<mean-2SD) as defined by the width and cross-sectional area of the bony island using Student's t-test.
Results
A total 136 ears of 68 patients (25 men and 43 women; age range 20–85 years, mean 49.8 years) were included in this study. No significant correlation was shown between LSCC bony island width or cross-sectional area and hearing level (P > 0.05). No significant difference in hearing levels were found among groups of the normal-sized, small and very small LSCC (P > 0.05).
Conclusion
We conclude that there is no correlation between isolated small LSCC and SNHL.
Inner ear malformations may cause sensorineural hearing loss (SNHL). In particular, cochlear anomalies such as Mondini's dysplasia and complete labyrinthine aplasia (Michel deformity) are common forms of inner ear malformation associated with SNHL, and such anomalies can be depicted by imaging methods, especially by high-resolution CT.
The lateral semi-circular canal (LSCC) is the last to complete ossification among the semi-circular canals and is the most susceptible to anomalous development (1). Disturbance of normal fusion and ossification may lead to a short LSCC complex or to a persistent anlage of the LSCC with the lack of a central ossified bony island (2–4). A correlation between small LSCC and SNHL has previously been reported. Johnson et al. reported 15 patients (28 ears) of LSCC malformation using temporal bone CT, concluding that LSCC malformation was associated with SNHL (5). However, in their study, 20 of 28 ears (11 patients) had other ear malformations including cochlear abnormalities. Additionally, more recent studies have shown conflicting results (6–8), and thus the correlation between LSCC morphology and SNHL remains controversial.
Our purpose was to determine whether there is a correlation between the isolated small LSCC and SNHL.
Material and Methods
Case selection
This study was approved by the Institutional Review Board of our university hospital. We retrospectively reviewed CT images and medical charts of 575 consecutive patients who underwent temporal bone CT scan at our hospital between January 2007 and August 2008. Patients under 20 years old, those with conductive hearing loss or mixed hearing loss, and those who had head trauma were excluded from the study. Patients who were suspected of having otosclerosis by otolaryngologists and those who had visually obvious abnormalities other than LSCC on CT such as cochlear dysplasia, temporal bone tumor, and lesion in the internal auditory meatus were also excluded. Five hundred and seven patients were excluded from the study, leaving 136 ears of 68 patients (25 men and 43 women; age range 20–85 years, mean 49.8 years) who met the inclusion/exclusion criteria were included in this study. Among them, 42 ears were of normal hearing level (0–20dB) and the remaining 94 ears were found to have SNHL (>20dB). The morphology of the cochlea and SSCC was screened by CT measurement as described in the following sections. Other inner ear structures such as the PSCC and internal acoustic meatus were visually evaluated.
CT scan of the temporal bone
All CT images were obtained using a 64-detector-row CT scanner (Aquilion, Toshiba Medical Systems Corporation, Tokyo, Japan) with 0.5-mm collimation and a 512 × 512 matrix. Transverse scans were acquired in a plane parallel to the orbitomeatal plane in the helical mode with 120 kV, 250 mAs, 1-s rotation time, 0.5 mm section thickness and overlap 0.3 mm with its adjacent slice, beam pitch 0.625, scan field of view (FOV) 240 mm, and display FOV 80 mm. Coronal reformatted multiplanar images were generated on the basis of the transverse images with a 1-mm section thickness and an overlap of 0.5 mm. All images were displayed at a window center of 400 HU and a window width of 4000 HU on picture archiving and communication systems (PACS) (Rapideye, Toshiba, Tokyo, Japan).
Inner ear measurements
Measurements on CT images were independently performed by two radiologists (KY as reader 1 and TD as reader 2) using the electronic calipers on the PACS and were recorded in millimeter units. We measured the maximum width and cross-sectional area of the LSCC bony island (central bony island bounded by LSCC lumen and vestibule) (Fig. 1). The LSCC bony island width was measured in the coronal section and at its greatest diameter (Fig. 1a). The LSCC bony island cross-sectional area was measured in the axial plane and at its greatest area (Fig. 1b). In order to exclude cases with abnormalities in the bony labyrinth other than LSCC, we also measured the width of the SSCC bony island and the cochlear height in the coronal section.
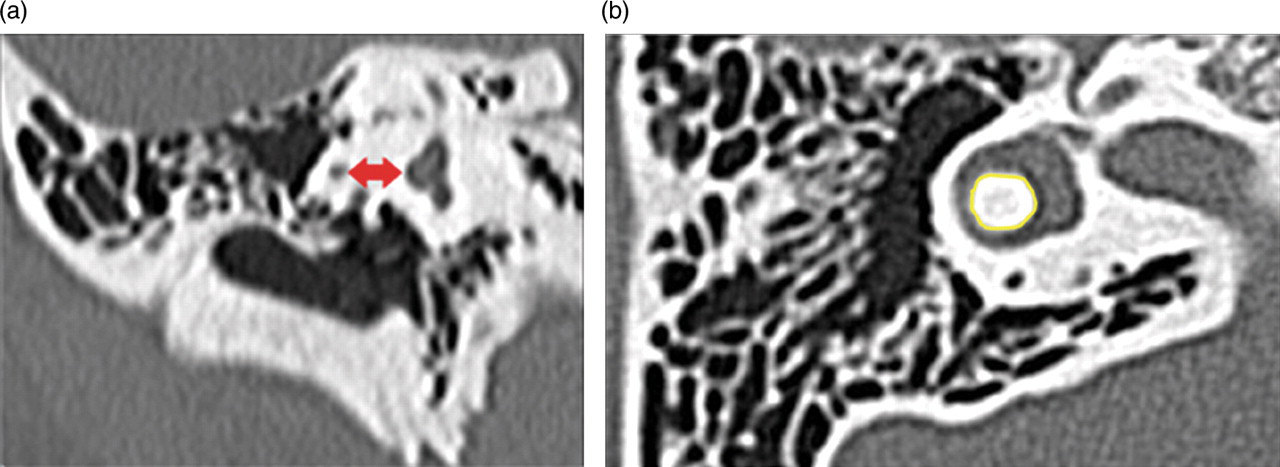
Measurements of the LSCC. (a) The LSCC bony island width was measured in the coronal section and at its greatest diameter; (b) The LSCC bony island cross-sectional area was measured in the axial plane at its greatest area
Audiometry
Each patient underwent an audiometric test in a double-walled sound room within 1 month before or after the CT examination. Air conduction, bone conduction, and the air-bone gap threshold were recorded at 250, 500, 1000, 2000, 4000, and 8000 Hz. The hearing levels for air conduction and bone conduction were calculated using the formula (500 Hz + 2 × 1000 Hz + 2000 Hz)/4.
Statistical analysis
We first evaluated the relationship between the LSCC bone island width or cross-sectional area and hearing level in all cases. Confidence ellipse with a probability of 0.95 were utilized to evaluate interobserver correlation of the measurements and Pearson correlation co-efficients were calculated to determine whether there is significant correlation between LSCC morphology (width and area of the bony island) and hearing level.
In addition, in order to determine whether small LSCC is associated with SNHL, all cases were classified into three groups according to each of the measured values (width and area of the bone island): ≧mean-SD (defined as a ‘normal’ group), <mean-SD (defined as a ‘small’ group) and < mean-2SD (defined as a ‘very small’ group). Hearing levels were compared using a one-tailed Student's t-test based on the hypothesis that small LSCC is associated with SNHL.
In all statistical analyses, the value of the significance level was P < 0.05.
Results
The width of the SSCC bony island of the normal hearing ears was 4.66 ± 0.52 mm (mean ± SD) and 4.81 ± 0.52 mm for readers 1 and 2, respectively. The SSCC bony island width of the ears with SNHL ranged 4.85 ± 0.69 mm and 4.94 ± 0.73 mm for readers 1 and 2, respectively. Thus each ear with SNHL was found to have normal-sized (> mean-2SD of the values of normal hearing patients) SSCC. Similarly, the cochlear height of the normal hearing ears was 4.72 ± 0.34 mm and 4.74 ± 0.36 mm for readers 1 and 2, respectively. Corresponding values of the ears with SNHL ranged 4.72 ± 0.36 mm and 4.78 ± 0.36 mm for readers 1 and 2, respectively, showing that, for each ear with SNHL, the size of the cochlea was found to be within the normal range. Moreover, we found no ear with a visually detectable abnormality in any inner ear structures other than the LSCC.
Fig. 2 shows scattered graphs of the relationship between the LSCC bony island width (Fig. 2a) or cross-sectional area (Fig. 2b) and hearing level in all cases. Pearson correlation co-efficients between the LSCC bony island width and hearing level for readers 1 and 2 were 0.03 (p = 0.90) and 0.01 (p = 0.75), respectively, and those between the LSCC bony island cross-sectional area and hearing level for the two readers were 0.07(p = 0.42) and 0.13 (p = 0.22). No significant correlation was found in any of those comparisons.
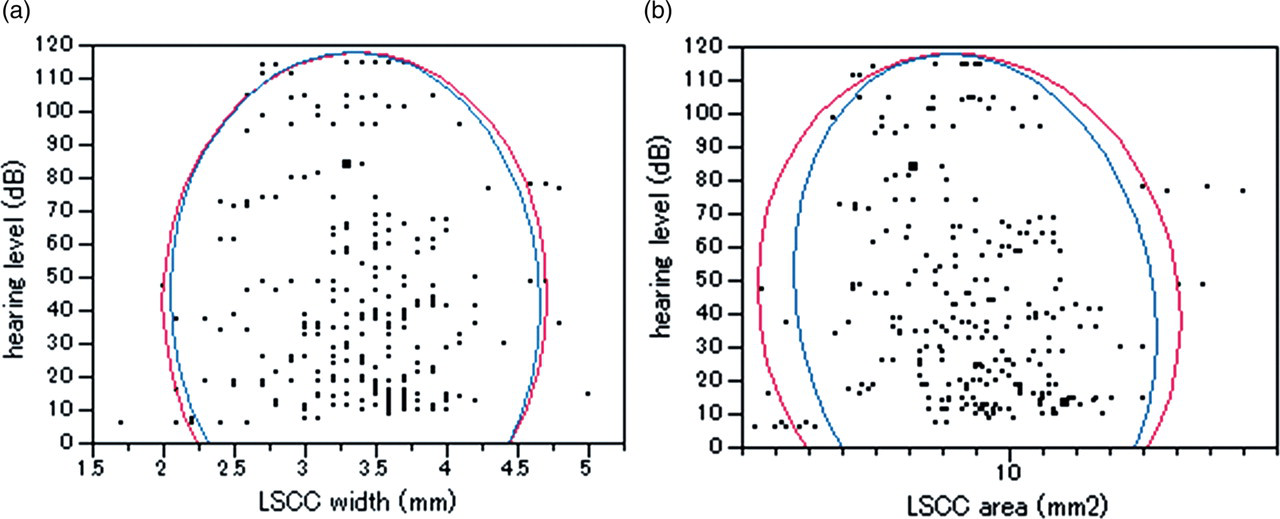
Scattered graphs of the relationship between (a) LSCC bony island width and (b) cross-sectional area and hearing level in all cases. Confidence ellipses with probability of 0.95 were superimposed on each graph. Blue arc indicates the 95% probability circle of data from reader 1, and red arc indicates that of data from reader 2. The graphs reveal low correlation coefficient. Pearson correlation co-efficients between the bony island width and hearing level were 0.03 and 0.01 for readers 1 and 2, respectively, and those between the bony island cross-sectional area and hearing level were 0.07 and 0.13 for readers 1 and 2, respectively
Fig. 3 shows the results of hearing level comparisons among the ‘normal’, ‘small’ and ‘very small’ groups defined according to the size of the LSCC. Grouping by the width of the LSCC bony island allowed 117 ears to be placed in the ‘normal’ group, 19 ears in the ‘small’ group and six ears in the ‘very small group’ for reader 1, and 115 ears in the ‘normal’ group, 21 ears in the ‘small’ group and six ears in the ‘very small group’ for reader 2. Correspondingly, grouping by the cross-sectional area of the LSCC bony island resulted in 115 ears in the ‘normal’ group, 21 ears in the ‘small’ group and six ears in the ‘very small’ group for reader 1, and 118 ears in the ‘normal’ group and 18 ears in the ‘small’ group and six ears in the ‘very small’ group for reader 2, respectively. For both readers, none of the comparisons yielded a significant difference in hearing level between the ‘small’ and ‘normal’ groups or between the ‘very small’ and ‘normal’ groups (P > 0.05, one-tailed Student's t-test) (Fig. 3).
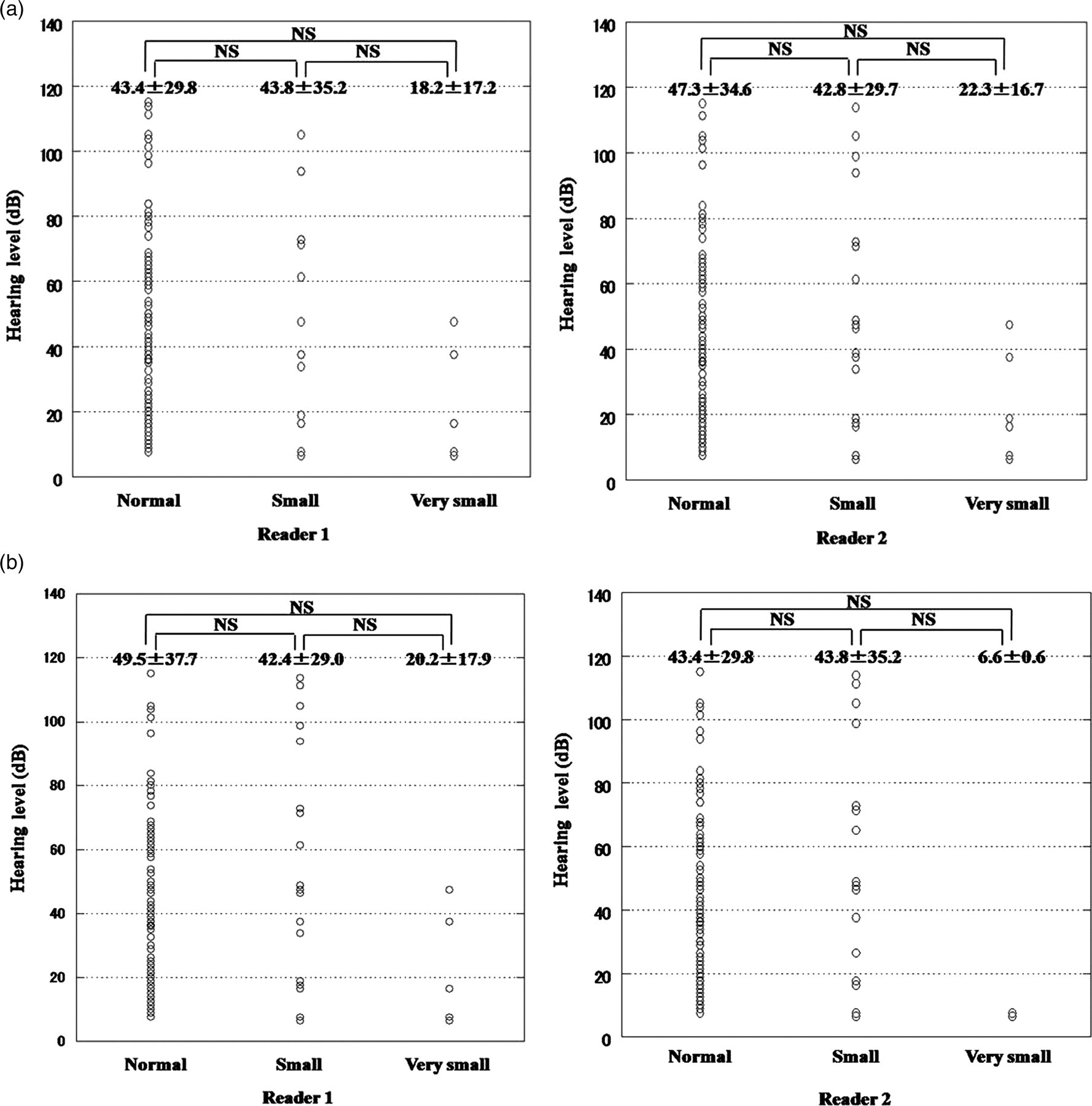
Comparisons of hearing levels among the patient group with the normal-sized LSCC (≧mean-SD), small LSCC (<mean-SD), and very small LSCC (<mean-2SD) as defined by (a) the width and (b) cross-sectional area of the bony island. The number above each plot indicates mean ± SD. No significant differences were found in any of the comparisons (one-tailed t-test)
Discussion
Our study showed that there is no significant correlation between the LSCC bony island width or cross-sectional area and hearing level, and that small LSCC is not associated with lower hearing levels.
Traditionally, inner ear malformations have been thought to be associated with SNHL, and Johnson et al. have shown a correlation between LSCC malformation and SNHL (5). Previous studies have found bony labyrinth abnormalities in 6.8–41% of children with SNHL (9–12). However, any labyrinthine anomalies were included in these studies. Recently, some studies suggested that there was no consistent association between LSCC morphological abnormalities and SNHL (6, 7). In addition, Dallen et al. have reported a patient with bilateral LSCC aplasia but without hearing loss (8). Yu et al. found no correlation between the severity of hearing loss and frequencies of radiologic abnormality, and speculated that the hearing loss associated with semicircular canal dysplasia is most likely due to anomalous membranous labyrinth development, which is not radiologically detectable (4). Nam et al. have stated that occlusion of the injured semi-circular canal might be an effective method in preserving postoperative hearing (13). These previous studies were based on observations of ears with SNHL. We evaluated ears with and without SNHL and found no significant correlation between small LSCC, as determined by bony island size, and SNHL.
The advent of MDCT has allowed us to obtain accurate radiologic measurements of the inner ear. However, there have been no previous reports in which the correlation between LSCC morphology and SNHL was investigated by comparing CT measurements from subjects with and without SNHL. This study confirms the lack of correlation between isolated dysplasia of the lateral semi-circular canal and SNHL.
In this study, we measured the size of bony island instead of that of the LSCC lumen. In LSCC dysplasia, it is partially or completely confluent with the vestibule (1), making direct measurement of LSCC difficult. Moreover, many authors have reported useful measurements of the LSCC bony island (6, 14, 15). Therefore, we measured the maximum width and cross-sectional area of the LSCC bony island.
This study has several limitations. First, due to its retrospective nature, it was subject to potential bias in patient selection, although the subjects were selected from consecutive patients according to consistent inclusion/exclusion criteria. Measurement of PSCC length was done in the axial plane in a previous study (14). However, we could not in most cases identify the maximum length of the PSCC using only axial images. Therefore, the PSCC length was evaluated visually. In measurements of the SSCC and cochlea, our results were similar to those obtained from previous measurements (16). Finally, the difference in cranium size or body height was not taken into account. However, Purcell et al. have stated that the inner ear labyrinth does not change in size after birth (14). We therefore believe that the effects of these parameters are negligible.
In conclusion, we revealed no correlation between the width and the cross-sectional area of the LSCC bony island, and hearing level. Isolated small LSCC was not associated with low hearing ability.
Footnotes
ACKNOWLEDGEMENT
The authors are grateful to Dr Junji Kishimoto for his helpful statistical analyses and to Professor Shizuo Komune for his helpful discussions pertaining to this work.