
Abstract
Background
Early detection and treatment of pulmonary fungal infection in immunocompromised patients has a profound impact on mortality. However, information available about the thin-section computed tomography (CT) findings of Candida pneumonia has largely been limited to isolated cases seen in reviews of various infections and to other acute lung diseases seen in immunocompromised patients.
Purpose
To dynamically observe and evaluate CT findings in immunosuppressed animals with histopathologically confirmed pulmonary candidiasis at the acute stage.
Material and Methods
Twenty-four New Zealand rabbits were randomly divided into an experimental group (n = 21) and a control group (n = 3). Pulmonary candidiasis was established by C. albicans inoculation via a transtracheal route in immunosuppressed rabbits in the experimental group, and an equivalent amount of normal saline was injected via the same way in the control group. Chest CT scan was performed before and on alternative days after inoculation/injection. Microbiological and pathological results were obtained by autopsy.
Results
In the experiment group, pulmonary candidiasis was successfully established in 13 rabbits as confirmed by microbiology and pathology. Areas of air-space consolidation were present in 10 (10/13) rabbits, with lobular distribution in six and lobar or segmental distribution in four, pathologically presenting as bronchopneumonia or hemorrhagic lung infarcts. Areas of ground-glass opacity (GGO) were identified in five (5/13) rabbits, three of which were associated with other abnormalities, presenting as bronchopneumonia or interstitial pneumonitis. Multiple nodules were seen in three (3/13) rabbits. They were clustered around bronchovascular bundles in two rabbits, and subpleural in the remaining one, pathologically presenting as hemorrhagic granulomas. Other less common CT findings included thickening of bronchovascular bundles (n = 3), linear opacity (n = 1), and pneumothorax (n = 1). No abnormality was detected by CT scan and pathological examination in the three rabbits of the control group.
Conclusion
Peripheral multiple areas of lobular consolidation and/or GGO representing bronchopneumonia were the most common thin-section CT findings of pulmonary candidiasis at the early stage.
Fungal infection of the lung in immunocompromised patients has received increasing attention during the past decade. Pulmonary complications induced by fungal infection may cause high morbidity and mortality despite improved antifungal therapy. Pulmonary candidiasis typically affects immunosuppressed critically-ill patients, especially those with indwelling catheters, patients receiving broad-spectrum antibiotics, and those with diabetes. Between 1980 and 1990, Candida species were isolated in up to 86% of immunocompromised patients with fungal pneumonia (1). C. albicans, which was detected most frequently, was isolated from 60–70% of all samples every year (2). In the 1990s, with the widespread use of prophylaxis in high-risk patients, the number of cases of candidiasis decreased. Although disseminated candidiasis is common in these groups of patients, pulmonary disease is relatively rare (1). As the clinical symptoms of pulmonary candidiasis such as fever and productive or non-productive cough are non-specific, it is difficult to detect the disease early and the condition may progress to hypoxemia and dyspnea quickly in such patients. Therefore, an early and definite diagnosis followed by quick and effective treatment based on the diagnosis is very important, which has a profound impact on mortality rates. The diagnosis of pneumonia due to Candida sp, which is a normal flora in the upper respiratory tract, may be based not only on a fungal culture of sputum, tracheal suction fluid, or bronchoalveolar lavage fluid, but on histopathological identification of fungi in tissues through transbronchial or surgical biopsy (3–7). However, these diagnostic methods are invasive and relatively late for early treatment of pulmonary candidiasis. Computed tomography (CT) is a non-invasive technique in examining immunocompromised patients with suspected pulmonary fungal infection. To our knowledge, there are few reports in the literature about CT findings of Candida pneumonia. Thus, the purpose of the present animal study was to examine and illustrate thin-section CT findings at the acute stage, and assess their correlations with histopathologic changes.
Material and Methods
Experimental animal and materials
Ethical approval was obtained from the institutional review board of our university. A total of 24 New Zealand white rabbits of either sex weighing 1.5–2.5 kg were purchased from Haike Laboratory Animal Department (Minhang District, Shanghai, China). All rabbits were proved healthy by quarantine (SCXK [Shanghai] 2002-0015). C. albicans (ATCC10235 standard strain), Sabouraud's medium, and Rice Tween Agar Mediums were provided by Fungi Laboratory of Dermatology, Changzheng Hospital Affiliated to the Second Military Medical University (Shanghai, China). Experimental drugs including ketamine (Shanghai Biochemical Pharmaceutical Company, Shanghai, China), cytosine arabinoside (Ara-C) (Haizheng Pharmaceutical Co., Ltd, Zhejiang Province, China), vancomycin (Eli Lilly Japan K.K, Seishin Laboratories), ceftazidime (Luoxin Pharmaceutical Co., Ltd, Shandong Province, China), and gentamycin (Luoxin Pharmaceutical Co., Ltd, Shandong Province, China) were purchased from Changzheng Hospital.
Experimental grouping
The 24 rabbits (Nos. 1–24) were randomly divided into an experimental group (n = 21) and a control group (n = 3). All rabbits were individually housed and maintained with water and standard rabbit feed in the Animal Center of Shanghai Public Health Clinical Center.
Preparation of fungal suspension
C. albicans was picked by an inoculating loop under sterile conditions, and subcultivated in Sabouraud medium, then sealed and cultivated in a 37°C incubator for resuscitation for 3 days. The resuscitative colony was picked by a sterile inoculating loop into the test tube and mixed with normal saline, shaken well gently to prepare fungal suspension. The final concentration of the saline suspension of C. albicans was regulated to 5 × 108 cfu/mL.
Establishment of the animal model
During the first five days of the experiment, Ara-C at a dose of 440 mg/m2 (body surface area) was injected daily via the ear vein in both experimental and control groups to produce profound and persistent neutropenia. The body surface area was calculated by body weight conversion formula:
body surface area (A) = 0.05*Weight + 0.05
After six days, Ara-C was injected on alternative days to maintain a low immune status. The results of blood routine tests on day 1 and 6 were compared. On and after day 4, antibiotics were given intravenously via the ear vein in both groups, including vancomycin 15 mg/kg, ceftazidime 150 mg/kg daily, and gentamycin 5 mg/kg on alternative days to prevent the occurrence of invasive bacterial infections during neutropenia. On the sixth day, 0.2 mL C. albicans suspension at 5 × 108 cfu/mL was injected into the trachea of the rabbits in the experimental group through percutaneous tracheal puncture. An equivalent amount of normal saline was injected intratracheally in the control group. Inoculation was performed under general intravenous anesthesia with ketamine (25 mg/kg). All the above operations were carried out in a bio-safety cabinet (NU-430 cabinet, Class II, Type B2, NuAire, Doylestown, PA, USA) in the Biological Safety Protection Laboratory (BSL-2) of the Animal Center, Shanghai Public Health Clinical Center.
Chest CT scan was performed with a 16-slice spiral scanner (Somatom Sensation 16; Siemens Medical Systems, Forchheim, Germany) in both groups before and on days 2, 4, 6, 8, 10, 12, and 14 after inoculation. Ketamine (25 mg/kg) was given intravenously before CT scan to calm down the animals in a supine position during scanning. The scanning parameters were 120 KV, 200 mAs, pitch 1.5, reconstruction thickness 1 mm, interval 1 mm, lung algorithm, and standard algorithm. The scans were viewed at the standard lung window (level –600 HU, width 1200 HU) and the mediastinal window (level 40 HU, width 350 HU).
On day 14 after inoculation, all rabbits were sacrificed if they did not die naturally. Lung tissue samples of all rabbits were obtained by autopsy according to the location of CT findings. All samples were pathologically diagnosed by HE (Hematoxylin-eosin) and PAS (periodic acid-Schiff) staining and microbiologically diagnosed by fungal culture.
CT interpretation
Two radiologists (SY LIU and LX XIE with 23 and 6 years of experience with chest CT, respectively) who were blinded to the identity of each rabbit in the study group reviewed the scans and arrived at decisions in consensus. The scans were evaluated for nodules, masses, areas of ground-glass opacity, areas of consolidation, linear opacities, thickening of bronchovascular bundles, pleural effusions, and lymphadenopathy. The time in which abnormalities presented and the extent were also noted. Ground-glass opacity (GGO) was defined as an area of hazy increased attenuation without obscuration of underlying vascular markings. Air-space consolidation was considered present when the opacities obscured the underlying vessels. Nodules were defined as round or oval opacities that were less than 3 cm in greatest diameter. If these opacities were 3 cm or larger in greatest diameter, they were referred to as masses. The nodules were subcategorized according to their diameter (smaller or larger than 10 mm), distribution (centrilobular, around bronchovascular bundles, subpleural, or random), location (upper or lower lung zone), marginal characteristics (smooth or irregular), and number (single or multiple). Nodules were also assessed as to whether or not they were surrounded by a halo of GGO. Lymphadenopathy was determined when the short-axis diameter exceeded 1 cm.
The anatomic distribution was assessed as predominantly in the upper or lower lung zones or as predominately peripheral, central, or peribronchial. Peripheral distribution was considered present when the abnormalities were seen mostly in the outer third of the lung; central distribution, if most abnormalities were in the inner third of the lung; peribronchial distribution, if abnormalities occurred along the bronchovascular bundles; and random distribution, if abnormalities did not fall into any of the aforementioned categories. The distribution was further subclassified as lobar, segmental, and lobular or patchy. Zonal predominance was divided into being upper or lower. Upper lung zone predominance was considered present when most of the abnormalities were above the level of carina, and lower zone predominance was considered when the abnormalities were below that level.
Diagnostic criteria
The following diagnostic criteria for Candida pneumonia were adopted in our study: (a) The inoculated C. albicans was identified in the lung tissue samples by fungal culture from Sabouraud's medium; (b) The focus of infection was detected by CT scan; (c) HE staining of the lung tissue samples showed fungal invasive appearance and inflammatory histological findings, including hemorrhage, hyperemia, exudation, inflammatory cell infiltration, interstitial hyperplasia, vascular thrombosis and necrosis; and/or (d) yeast cells or pseudohyphae were found by HE or PAS staining. Microbiological diagnosis of fungal culture was given by a dermatologist of the Fungi Laboratory of Dermatology, and histological findings of HE and PAS staining were verified by two pathologists of Changzheng Hospital. If the first criterion was confirmed, the inoculation was considered successful. If all above criteria were confirmed, the rabbit model with C. albicans pneumonia was considered to have been established successfully. If the first criterion was confirmed but the second or the third was not meanwhile, it was thought of as the situation of dormant infection with C. albicans field planting in rabbit lungs.
Results
Modeling results of pulmonary C. albicans infection in immunosuppressed rabbits
The neutrophil count in venous blood decreased to less than 0.5 × 109/L in 17 rabbits and to 0.5 × 109–1 × 109/L in 7 rabbits on the day of inoculation in all rabbits Two rabbits in the experimental group died of excessive anesthesia before inoculation. The remaining 19 rabbits underwent inoculation successfully. According to the diagnostic criteria, the diagnosis of C. albicans pneumonia was ascertained in 13 (13/19) rabbits in the experimental group, of which six (6/19) rabbits were judged as field planting of C. albicans in lungs. All 19 rabbits in the experimental group and one rabbit in the control group died naturally within 14 days after inoculation. The mean living time of the 13 rabbits with C. albicans pneumonia and six rabbits with C. albicans field planting in lungs was 7.23 ± 2.01 days and 12.30 ± 1.58 days, respectively. The other two rabbits in the control group were sacrificed on day 14 according to the plan. No abnormity was found in pathological and microbiological examination of the lung tissue samples of all three rabbits in the control group.
Thin-section CT findings
Chest CT examination was normal in all rabbits before inoculation (Figs. 1a, 2a, 3a). Abnormalities were detected on thin-section CT scans from day 2 to day 14 after inoculation (Table 1). The main CT findings (Table 2) were consolidation (10/13), GGO (5/13), multiple nodules (3/13) and thickening of bronchovascular bundles (3/13). Other less common CT findings included linear opacity (n = 1) and pneumothorax (n = 1). No lymphadenopathy was found.
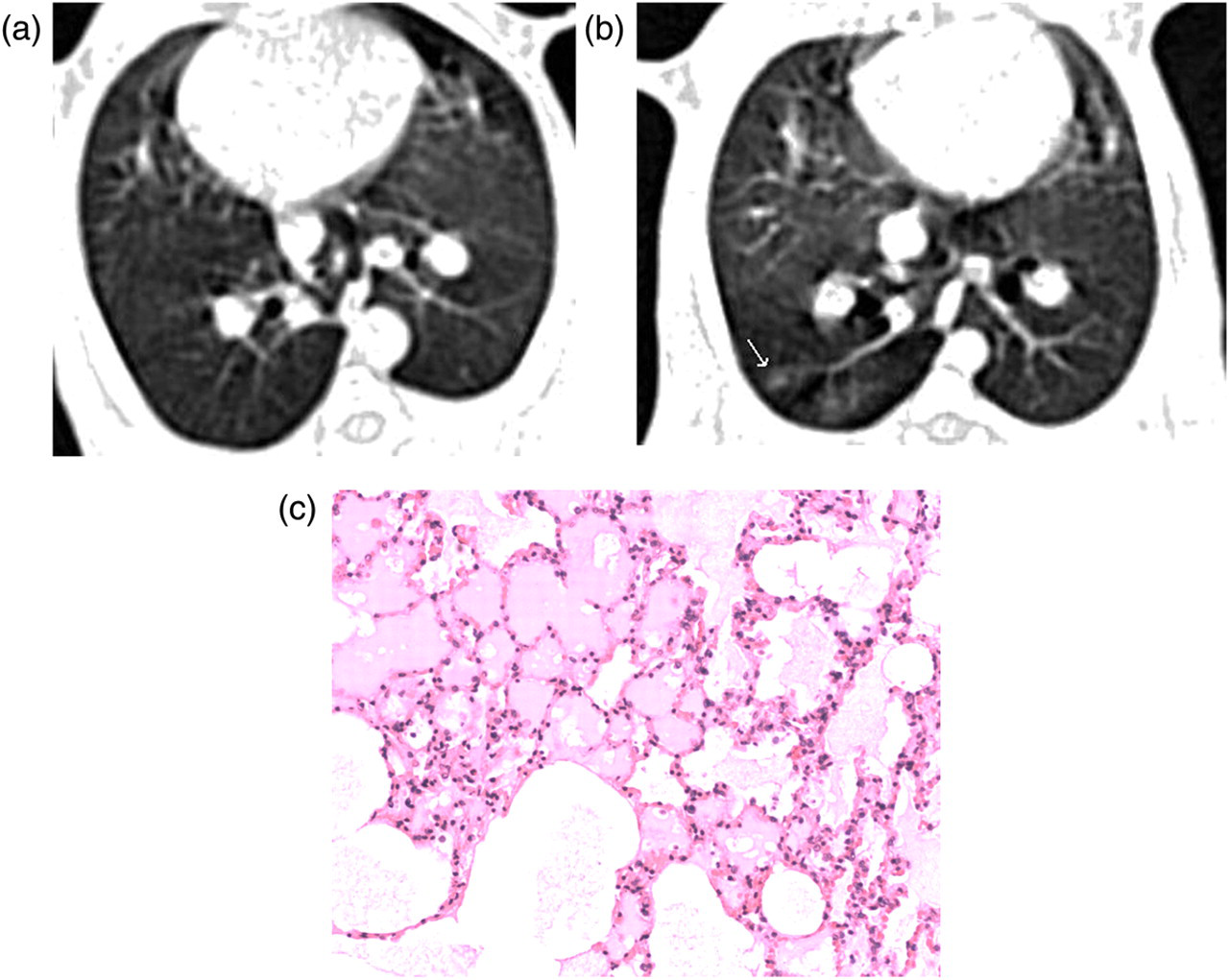
Rabbit no. 1: Compared with the normal CT image (a) before inoculation, areas of lobular consolidation with peripheral distribution were detected on day 2 after inoculation (b); Photomicrography showed intra-alveolar exudates (c, Hematoxylin-eosin stain; original magnification ×100)
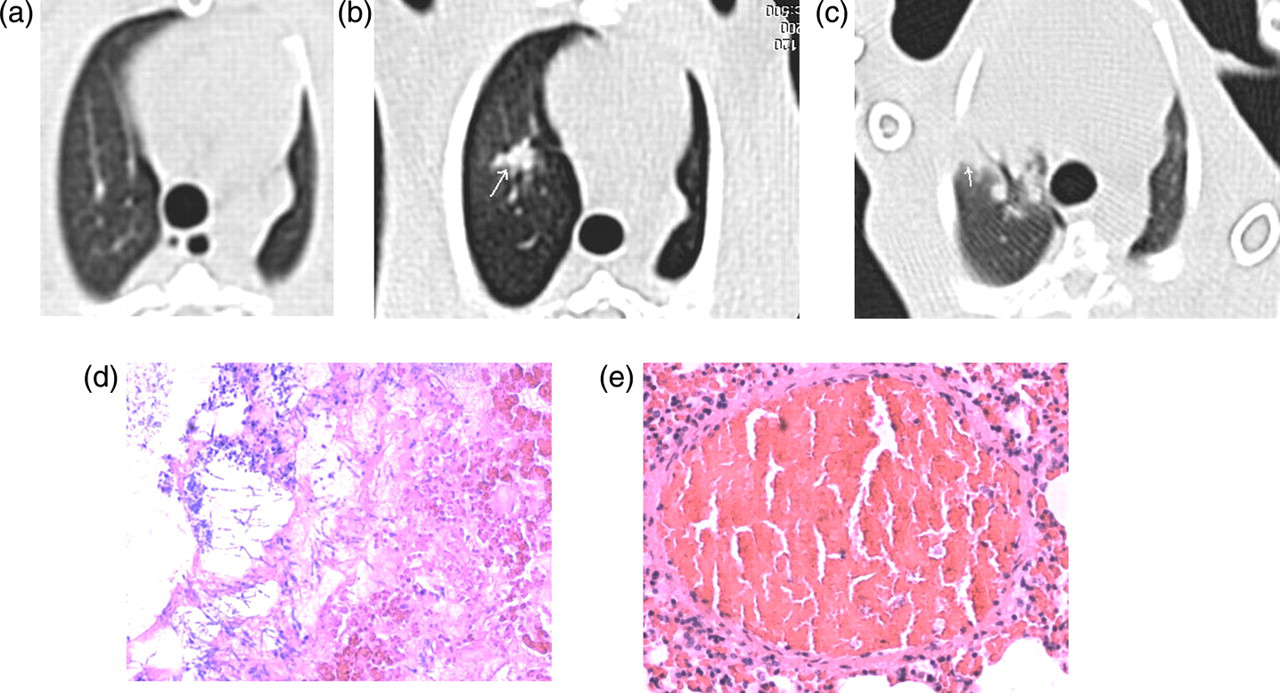
Rabbit no.13: CT scan showed normal appearance (a) before inoculation and detected multiple and clustered nodules of similar sizes surrounding the bronchovascular bundle of the right upper lung on day 10 after inoculation (b), and on the 12th day they developed into lobar consolidation (c). Photomicrography showed hemorrhagic infracts, in which a number of pseudohypha and blood cells were found (d, Hematoxylin-eosin stain; original magnification ×100), in addition to thrombogenesis found in pulmonary arteriole (e, Hematoxylin-eosin stain; original magnification ×100)
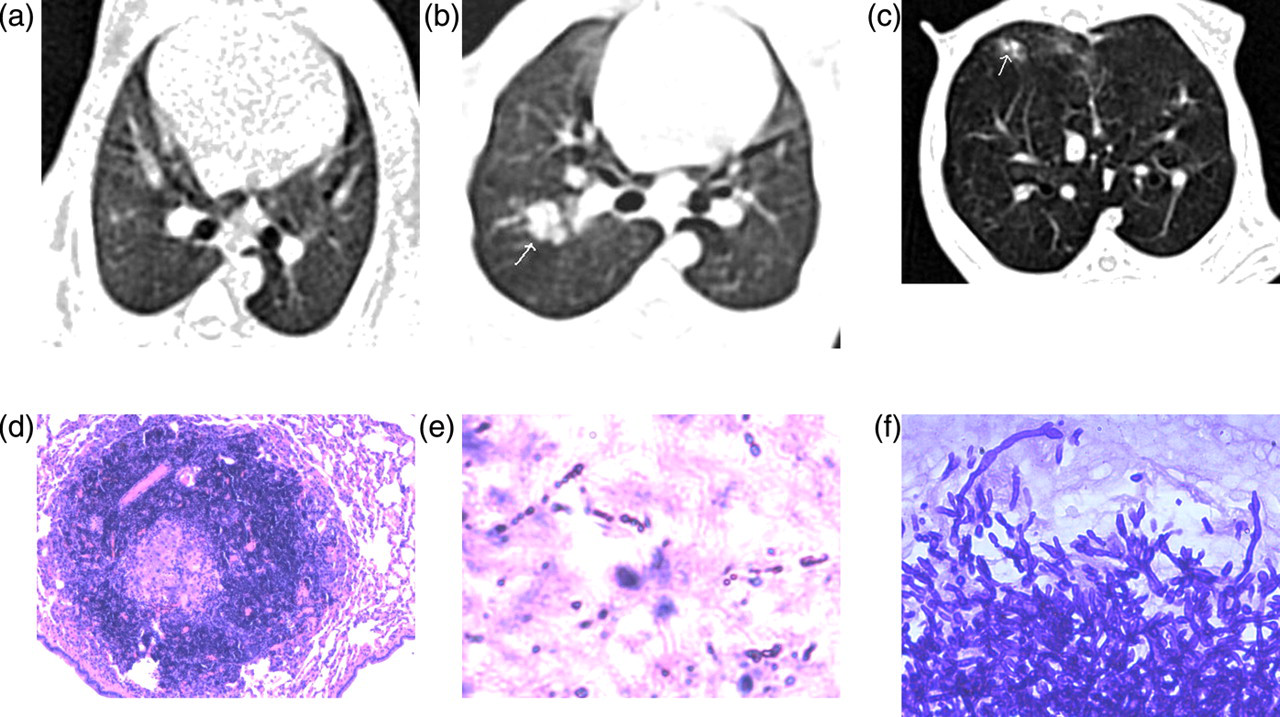
Rabbit no. 9: Compared with the normal CT image (a) before inoculation, multiple and clustered nodules surrounding by halo signs were found around the bronchovascular bundle of the right upper lung on day 6 after inoculation (b), and day 8 similar appearances were found at the end of the bronchus of the same lobe (c). Photomicrography showed granulomatous inflammation (d, Hematoxylin-eosin stain; original magnification ×100), and the central area of necrosis contained a number of pseudohyphae (e, Hematoxylin-eosin stain; original magnification ×100 and f, Periodic acid-Schiff staining ×400)
CT findings
All above rabbits were positively inoculated with candida
GGO = ground-glass opacity
The distribution of main CT findings
All above rabbits were positively inoculated with candida
GGO = ground-glass opacity
Areas of consolidation had a lobular distribution in six (6/10) rabbits (Fig. 1b) and a lobar or segmental distribution in four (4/10) rabbits (Fig. 2c). Five cases were associated with other abnormalities, with predominant appearance in four of them.
Areas of GGO were bilateral and symmetric in three rabbits and unilateral in two, which had no zonal predominance and were all multifocal. Three cases were associated with other abnormalities.
Nodules (n = 3) were all multifocal and bilaterally distributed, with smooth margins and less than 10 mm in diameter (Figs. 2b, 3b and 3c). They were found clustered in groups around the bronchovascular bundles in two rabbits and subpleural in one. In all three cases, at least one of the nodules was surrounded by a halo of GGO. Two cases were associated with other abnormalities and one of them was the predominant appearance.
CT examination showed normal appearance in all three rabbits in the control group.
Correlation between CT findings and pathological results
The histopathological material was correlated with the findings at thin-section CT. In the 13 rabbits with C. albicans pneumonia, 12 areas of consolidation or GGO seen on CT scans corresponded to the exudative or proliferative phase of diffuse alveolar inflammation. The histological findings of HE staining in these cases consisted of inflammatory infiltration in alveolus (Fig. 1c), thickening of alveolar wall and interstitial hyperplasia with infiltration of desmocytes and lymphocytes or with hemorrhage and congestion. Well-defined hemorrhagic infarcts were observed in four (4/10) consolidations, and in three of them cells of alveolar wall were seen necrotic but the structure remained basically intact with sphacelus, red blood cells and Candida organisms filled in alveolar space, and in the reaming one the alveolar structure was destroyed completely.(Fig. 2d). In addition, thrombi were observed in the pulmonary arteriole in two of them (Fig. 2e). Histologically, two (2/3) nodules showed well-defined granulomas (Fig. 3d and 3e), and the remaining one demonstrated focal necrosis and inflammatory reaction. The spore and/or pseudohypha of C. albicans were found by PAS staining in 11 (11/13) cases (Fig. 3f). In C. albicans field planting group, histological examinations were normal in four (4/6) rabbits and mild interstitial hemorrhage and congestion were found in two (4/6). Histological examination was normal in all three rabbits in the control group.
Discussion
Although Candida species are frequently isolated from samples from upper respiratory tract, it is difficult to ascertain whether a positive culture is consistent with a pathogen responsible for pneumonia or whether it occurs as a contaminant (7, 8). In the past, Candida pneumonia was usually diagnosed at autopsy. With the increased use of invasive biopsy procedures and aggressive surgical management, premortal diagnosis has become increasingly common. However, few reports on CT findings were available due to the difficulty of defining diagnosis and interference of combined infection. Animal experiments are advantageous over retrospective clinic studies in demonstrating the most common CT findings of pulmonary candidiasis at the early stage and clarifying their correlations with the pathology in that many conditions are strictly controllable in an animal experiment, such as immunosuppressive regimen, organism and preparation of inoculation, CT scan performing time, and morphological and microbiological studies. In this study, we established an animal (rabbit) model of Candida pneumonia. To our knowledge, this is the first study to evaluate CT findings of pulmonary candidiasis in a rabbit model. Compared to mice or rats, the lungs of a rabbit are relatively large and more anatomically similar to the human lungs. The routine position of the rabbit is prone, which differs from the human standing position, and therefore the distribution of CT appearances may have diversity when applied to humans.
Aspiration of contaminated oropharyngeal secretions is an important portal of entry for occurrence of pulmonary fungal infection. The result of fungal culture was positive in all 19 rabbits in the experimental group, indicating that upper respiratory tract contamination caused by injection of C. albicans suspension into the trachea well simulated the route of aspiration. Six rabbits in the experimental group did not show pulmonary candidiasis but showed field planting of C. albicans in the lungs after inoculation. We suppose that this is because the inoculated fungi could keep an aggregate state in the respiratory tract or alveoli, without causing inflammatory reaction and imaging changes. Based on our experience, strict sterile operation is the key point for successful establishment of the model, especially in procedures of inoculation and sample collection during autopsy. To prevent parasitic bacteria on the epidermis from entering the trachea, skin preparation and disinfection are necessarily before inoculation. The sterile instruments used in autopsy must be replaced promptly before opening every layer of tissue to ensure that all the instruments touching the lung samples are aseptic.
Dynamic observation of the CT appearances demonstrated that pneumonia caused by C. albicans in immunosuppressed rabbits progressed very quickly. All CT findings appeared for the first time between day 2 and day 10 after inoculation, and most of the abnormalities (9/13) were detected for the first time earlier than day 4 after inoculation. These results may reflect that patients infected with C. albicans have a relatively rapid clinical onset. No abnormal CT appearances or histological changes were found in all three rabbits in the control group, indicating that 0.2 mL liquid injecting in the rabbit trachea generally would not cause aspiration pneumonia, so that the possibility that the CT appearances could be caused by aspiration pneumonia in the experimental group could be excluded as well.
In the 13 rabbits with pathologically proved pulmonary candidiasis, areas of consolidation and areas of GGO were the most common CT findings (10/13 and 5/13, respectively). Areas of consolidation were associated with bronchopneumonia or hemorrhagic lung infarcts, and areas of GGO with bronchopneumonia or interstitial pneumonitis. This non-specific bronchopneumonia caused by localized Candida colonies in alveoli and/or bronchioles could not be differentiated from bacterial infections, which was the most common cause of bronchopneumonia in immunocompromised hosts, as well as mycobacterial, viral and other fungal infections (9, 10). Hemorrhagic lung infracts were similar to the characteristic CT appearance of invasive pulmonary infections caused by hyphomycete colonies such as aspergillus species and mucor species (11–13). Bronchopneumonia and hemorrhagic lung infarcts are the main early invasive manifestations of pulmonary candidiasis. These correlations between pathologic and radiological findings were confirmed in our study.
Nodules were detected in three (3/13) rabbits, in two of which they presented as the major CT findings, and in the remaining one they developed into lobar consolidation 2 days after first detection. The nodules were clustered around the bronchovascular bundles in two rabbits, which we consider is a characteristic way of distribution in the aspiration route and has not been reported in related reports. There was a halo sign surrounding the nodules in all cases, which was reported to associate with hemorrhagic nodules of varying causes (14), and with some non-hemorrhagic infections such as actinomycosis as well (15). Histologic correlation showed that the dense core of the nodules corresponded to a zone of coagulative necrosis due to growth of Candida pseudohyphae and obstruction of small blood vessels, and the halo corresponded to a mixture of edema and hemorrhage surrounding the infarct. These necrotic hemorrhagic nodules were previously described as the characteristic CT findings of invasive pulmonary aspergillosis (12, 16, 17), and may also appear in infections by mucor species, herpes simplex and cytomegalovirus, Wegener's granulomatosis, Kaposi's sarcoma (14), and hemorrhagic metastases. Similar appearance was also reported in the embolic form of pulmonary candidiasis by the route of hematogenous dissemination (18), due to thromboembolism with spores and pseudohyphae propagating from infected thrombi in the right atrium, central or peripheral vein, or tricuspid valve lodging in medium and small pulmonary arteries, but it was rarely seen in a bronchopulmonary form.
In a recent study including 17 hematopoietic stem cell transplant recipients with pulmonary candidiasis (19), multiple nodules with varying sizes from 3 to 30mm were reported to be seen in 88% of cases, which is different from what we observed in our rabbit model, where lobular consolidation and/or GGO was the main CT finding of bronchopneumonia. This discrepancy may be explained by the different routes of infection. Recipients of allogeneic hematopoietic stem cell transplants with the portal of entry such as the gastrointestinal tract or indwelling catheters were prone to have pulmonary candidiasis of embolic or disseminated form (7). But there was still some overlap between them.
Our study had several limitations. No other organ samples except the lung were obtained by autopsy, so whether the rabbits in C. albicans field planting group died of hematogenous dissemination via the pulmonary vein was not confirmed. In addition, the current model was established with the transtracheal route only, so pulmonary candidiasis of hematogenous dissemination was not investigated.
In conclusion, non-specific peripheral multiple areas of lobular consolidation and/or GGO representing bronchopneumonia are the main thin-section CT findings of acute-stage in our rabbit model.
Footnotes
Acknowledgements
This project was supported by the National Natural Science Foundation of China (No. 30970800).