
Abstract
Background
Coronary computed tomography angiography (CCTA) can delineate the coronary artery anatomy precisely. Basic knowledge of the normal coronary artery anatomy and familiarity with its common variations are essential in order to assess CCTA accurately.
Purpose
To determine the prevalence of coronary artery variations detected by 64-slice mutidetector CT.
Material and Methods
CCTA images of 2096 patients were evaluated retrospectively. Relatively unusual coronary artery morphological features that were seen in greater than 1% of the study population were classified as variations.
Results
Coronary artery circulation was right dominant in 86.6%, left dominant in 9.6%, and balanced in 3.8% of patients. The conus artery arose from the right coronary artery in 83%, or directly from the aorta with a separate ostium in 17% of cases which was much more common in men than women. The sinoatrial node artery originated from the right coronary artery (65.6%) or the circumflex artery (33.7%). The atrioventricular node artery originated from the right coronary artery in 86.4% or the circumflex artery in 13.6% of cases. The left main coronary artery was shorter than 0.5 cm in 4.7% of cases and trifurcated into the intermediate artery in 31.3% of cases. A myocardial bridge was observed in 21.6%, coronary ectasia-aneurysm in 2%, dual left anterior descending artery (LAD) type 1 in 1.38%, and a variant of type 1 in 0.1% of cases. The presence of coronary atherosclerosis was higher in patients with coronary ectasia-aneurysm than the patients who did not have coronary ectasia-aneurysm (90.5% vs. 72.2%, P = 0.000).
Conclusion
CCTA is a non-invasive imaging modality for the depiction of variations of the coronary arteries. The incidence of coronary artery variations is high and various, and readers should be familiar and looking for these conditions during interpretation of CCTA examinations.
Keywords
The coronary arteries have been previously evaluated only by conventional coronary angiography (CCA) which is an invasive and two-dimensional (2D) imaging modality (1, 2). After advances in multidetector computed tomography (MDCT) technologies, it is now possible to examine the coronary arteries and heart structures in a single and short breath-hold with high spatial and temporal resolution (1). MDCT can delineate the coronary artery anatomy precisely using multiplanar reformation (MPR), three-dimensional (3D) volume-rendering (VR), and maximum intensity projection (MIP) techniques and is an alternative to CCA for the evaluation of coronary artery disease in selected patients (1–3). It is essential that images of coronary computed tomography angiography (CCTA) are carefully interpreted in order to detect coronary artery variations and anomalies (3). In this article, our aim was to determine the prevalence of coronary artery variations detected by 64-slice MDCT in a single center.
Material and Methods
Patients
The study included a total of 2096 consecutive patients who underwent electrocardiography (ECG)-gated CCTA at one institution (29 May Hospital, Istanbul, Turkey) from March 2006 to June 2010. The mean age of the patients was 55 ± 11.5 years with a range of 6–80 years. Seventy percent were boys or men and 30% were girls or women. There were only three patients who were under 18 years old and scanned for coronary artery anomaly suspicion. The main indications for CCTA were atypical chest pain, angina pectoris, preoperative evaluation for non-coronary surgery, screening for coronary artery disease, and determination of the patency of bypass grafts or stents. Exclusion criteria for CCTA were severe arrhythmia, previous serious allergic reaction to contrast medium, pregnancy, renal and respiratory failure. The study was approved by the hospital's Ethics Committee.
Computed tomography (CT) protocols
All CCTA were performed using a 64-detector CT scanner (Lightspeed VCT, GE Healthcare, Milwaukee, WI, USA) with retrospective ECG gating. Images were obtained with detector collimation 64 × 0.625 mm; voltage 100 kVp or 120 kVp; tube current 400–500 mAs; pitch range 0.16–0.24 (mean 0.21); and gantry rotation time 0.35 s. ECG modulation was used to reduce radiation dose. Radiation dose was decreased during the systolic phase that was not necessary for interpretation of coronary arteries, and the full dose was delivered only during the diastolic phase (65–85% phase of the R-R interval) in which good quality images were formed. If there was no contraindication, oral beta-blockers (50–100 mg metoprolol, Beloc Zok, Astra Zeneca, Istanbul, Turkey) 1 h before the examination and/or intravenous beta-blockers (5 mg metoprolol IV bolus; Beloc ampule, Astra Zeneca, Istanbul, Turkey) just before the scan were used when the heart rate was greater than 70 bpm. The heart rate of patients ranged between 34–97 bpm (mean 59 bpm). Just before the scan, 0.4 mg nitroglycerine lingual spray (Nitrolingual pump spray, 0.4 mg, Farma-Tek) was administered to all patients to obtain dilatation and maximum opacification of the coronary arteries. An 18–20-gauge IV cannula was used for venous access in the upper extremity. The triphasic injection protocol, which is characterized by injection of 70–80 mL of non-ionic contrast medium with high iodine concentration (iohexol 350 mgI/mL, Omnipaque, Opakim, Istanbul, Turkey) at a flow rate of 5 mL/s followed by injection of a 40 mL solution of one half contrast medium and one half saline solution, and finally an injection of 50 mL saline with the same flow rate was used for CCTA. The scan time was determined using a bolus tracking technique by placing the region of interest over the ascending aorta and setting the trigger threshold to 150 Hounsfield units (HU). The scan was started manually and acquired during one breath-hold in 5–6 s with simultaneous ECG gating.
Image reconstruction and review
Images were reconstructed during the 75% phase of the R-R interval. Other cardiac phases were reconstructed in cases of bad image quality at the 75% of the R-R interval. Stored CT images in the picture archiving and communication system were transferred and processed on a separate cardiac dedicated workstation (Advantage Workstation 4.2, GE Healthcare, Milwaukee, WI, USA) and analyzed using curved MPR, 3D-VR techniques and thin-slab MIP reconstructions in addition to the axial source images. Images from all of the CCTA patients were evaluated retrospectively by one cardiovascular radiologist (5 years of cardiac imaging experience) in order to determine coronary artery variations and anomalies in the intrinsic coronary arterial anatomy.
Effective dose in millisieverts (mSv) was calculated by multiplication of the dose–length product by the conversion coefficient for the chest, 0.017.
Image quality of CCTA examinations was determined using a grading system: excellent image quality (grade 1) with no motion artifacts; good image quality (grade 2) with minor artifacts; moderate image quality (grade 3) with moderate artifacts due to motion or irregular heart beats; and non-diagnostic image quality (grade 4) with too many artifacts which make the evaluation impossible. Grades 1–3 were considered adequate for the evaluation of coronary artery anatomy and variations. Grade 4 patients were not included in the study.
The dominant coronary artery was determined by observing which coronary artery passed over the crux of the heart and gave off the posterior descending artery (PDA) branches. If both the right coronary artery (RCA) and the left circumflex artery (LCX) perfused the inferior interventricular septum, the coronary arteries were classified as co-dominant. Relatively unusual coronary artery morphological features that were seen in more than 1% of the study population were classified as variations. We also looked at variations in the conus artery, sinoatrial node artery, atrioventricular node artery, and intermediate artery. We used the classification system proposed by Angelini who divided coronary artery anomalies into anomalies of origination and course, anomalies of intrinsic coronary arterial anatomy, and anomalies of coronary termination (4).
Ectasia-aneurysm of the coronary artery was defined as a coronary artery diameter exceeding 1.5 times or more the diameter of the adjacent normal arterial segment. Coronary atherosclerosis was defined as presence of any soft or calcified atheroma plque in the coronary arteries.
Type 1 dual left anterior descending artery (LAD) was defined as a short LAD that terminates high in the anterior interventricular sulcus, and a long LAD that courses on the left ventricular side of the short LAD and re-enters the anterior interventricular sulcus at the distal part. The short and long LADs originate as a branch of the LAD proper in type 1 dual LAD. Atypical (variant) type 1 dual-LAD was defined as the origination of long and short LAD separately from the left main coronary artery (LMCA).
Statistical analyses
Each coronary artery variation and anomaly in the intrinsic coronary arterial anatomy was numbered and patient data (gender, age, presence of coronary atherosclerosis) were entered individually into a database. Data were analyzed using Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA) for Windows version 11.0 software. The frequencies and percentages of different variations and anomalies in the intrinsic coronary arterial anatomy were calculated. Continuous data were expressed as the mean ± standard deviation. Pearson's chi-square test was used for the analysis of how variations and anomalies in the intrinsic coronary arterial anatomy varied in distribution between genders and impact on coronary atherosclerosis. A P value of less than 0.05 was considered to be statistically significant.
Results
The prevalence of coronary artery variations
RCA = right coronary artery, RCS = right coronary sinus, LCX = left circumflex artery, LMCA = left main coronary artery, LCS = left coronary sinus
Coronary circulation was right dominant in 86.6%, left dominant in 9.6%, and balanced in 3.8% of patients (Fig. 1). No significant difference was detected between the sexes regarding the dominancy of the coronary circulation (P = 0.5). The conus artery, sinoatrial node artery, and atrioventricular node artery were visualized in 2092, 2072, and 2076 cases, respectively. The conus artery arose as the first branch from the proximal RCA (83%), or directly from the right coronary sinus (RCS) with a separate ostium (17%) (Fig. 2a). There was a statistical difference between male (18.7%) and female (13%) patients whose conus artery originated from the RCS (P = 0.009). The sinoatrial node artery (Fig. 2a and c) originated from the RCS (9 patients), descending aorta (4 patients), LMCA (1 patient), and left coronary sinus (LCS) (1 patient) in a small percentage of the patients. There was a statistically significant difference between the genders (men 34.2% and women 24.6%) with regards to the presence of an intermediate artery (P = 0.00) (Fig. 2b).
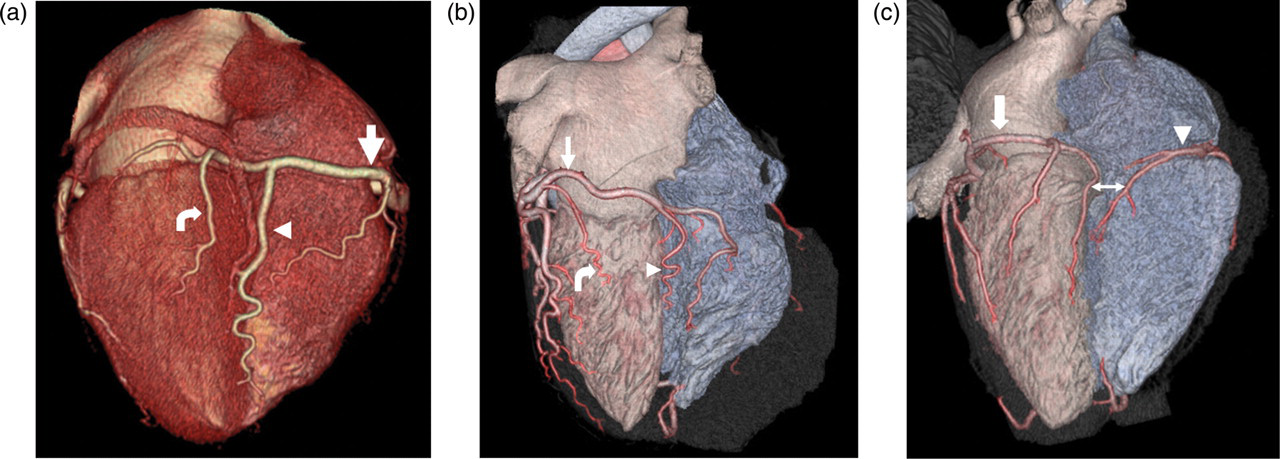
Three-dimensional volume-rendered CT angiography images of three different male patients. (a) A right dominant coronary circulation. The right coronary artery (RCA) (arrow) divides into the posterior descending artery (PDA) (arrowhead) and postero-lateral branch artery (PLB) (curved arrow) at the crux of the heart. (b) The PDA (arrowhead) originating from the left circumflex artery (LCX) (arrow) is perfusing the inferior interventricular septum in a left coronary dominancy. Curved arrow indicates a branch of obtuse marginal artery; (c) The RCA (arrowhead) and LCX (arrow) supply the inferior interventricular septum by a PDA (two-headed arrow) branch in co-dominancy
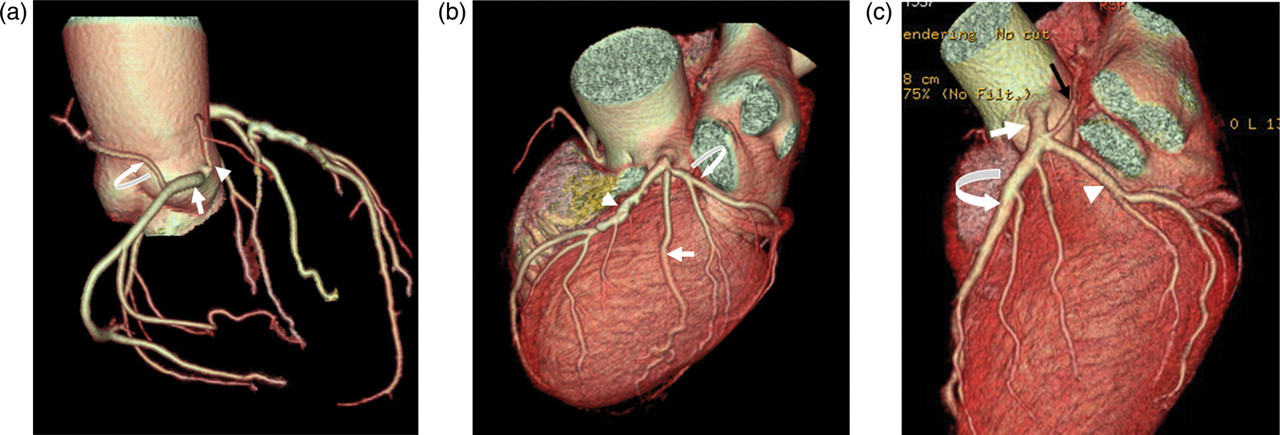
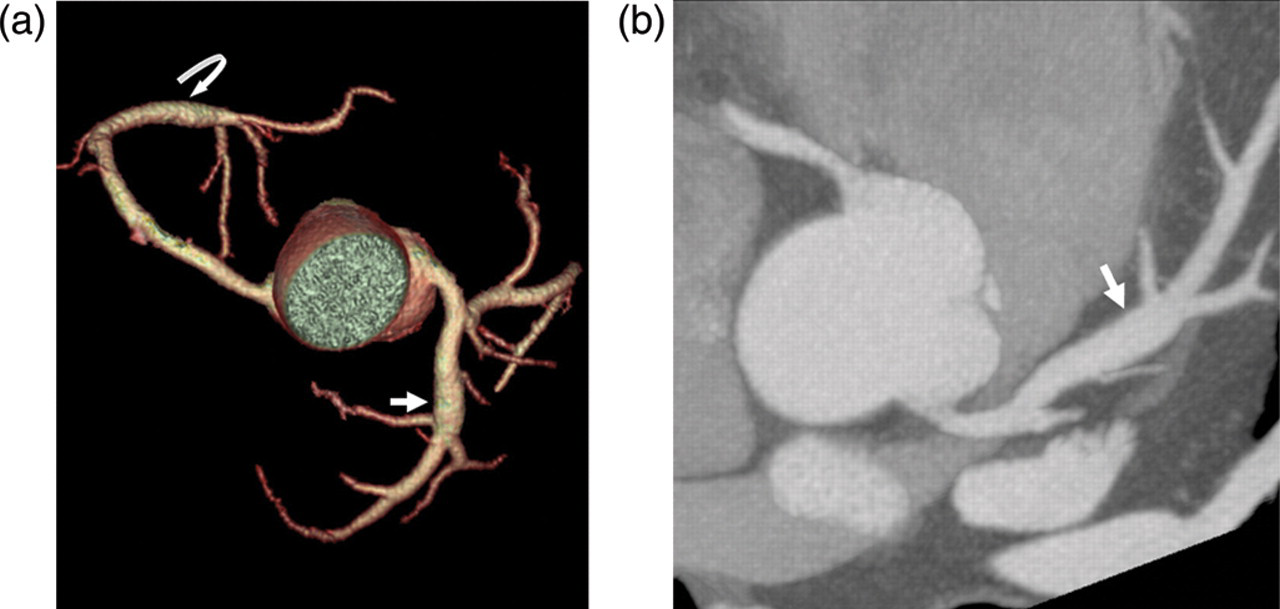
Three-dimensional volume-rendered (3D-VR) image of the aortic root and coronary tree (a) shows that the sinoatrial node artery (SAN) (curved arrow) originates from the right coronary artery (arrow), and the conus artery (CA) (arrowhead) arises from the aorta separately. 3D-VR image of the same patient (b) shows that the intermediate artery (arrow) originates from the left main coronary artery between the left anterior descending artery (LAD) (arrowhead) and left circumflex artery (LCX) (curved arrow). 3D-VR image of another patient (c) shows that the SAN (black arrow) arises from the left main coronary artery (white arrow) before origination of the LAD (curved arrow) and LCX (arrowhead)
The prevalence of variations in the intrinsic coronary arterial anatomy was 25.1% (Table 2). A total of 453 patients with 458 myocardial bridging (MB) were detected. Of these, 347 (76%) were located in the mid LAD, 84 (18%) in the distal LAD, 11 (2.4%) in the mid to distal LAD, four (0.9%) in the RCA, 4 (0.9%) in the intermediate artery, four (0.9%) in the PDA, one each in the proximal LAD, LMCA, LCX, and in short LAD of dual LAD (Fig. 3). Only 21% of MB cases (94 patients) were isolated and had not got any concomitant coronary artery disease or cardiac and extracardiac pathologies. Unfortunately there were no information about their outcome.
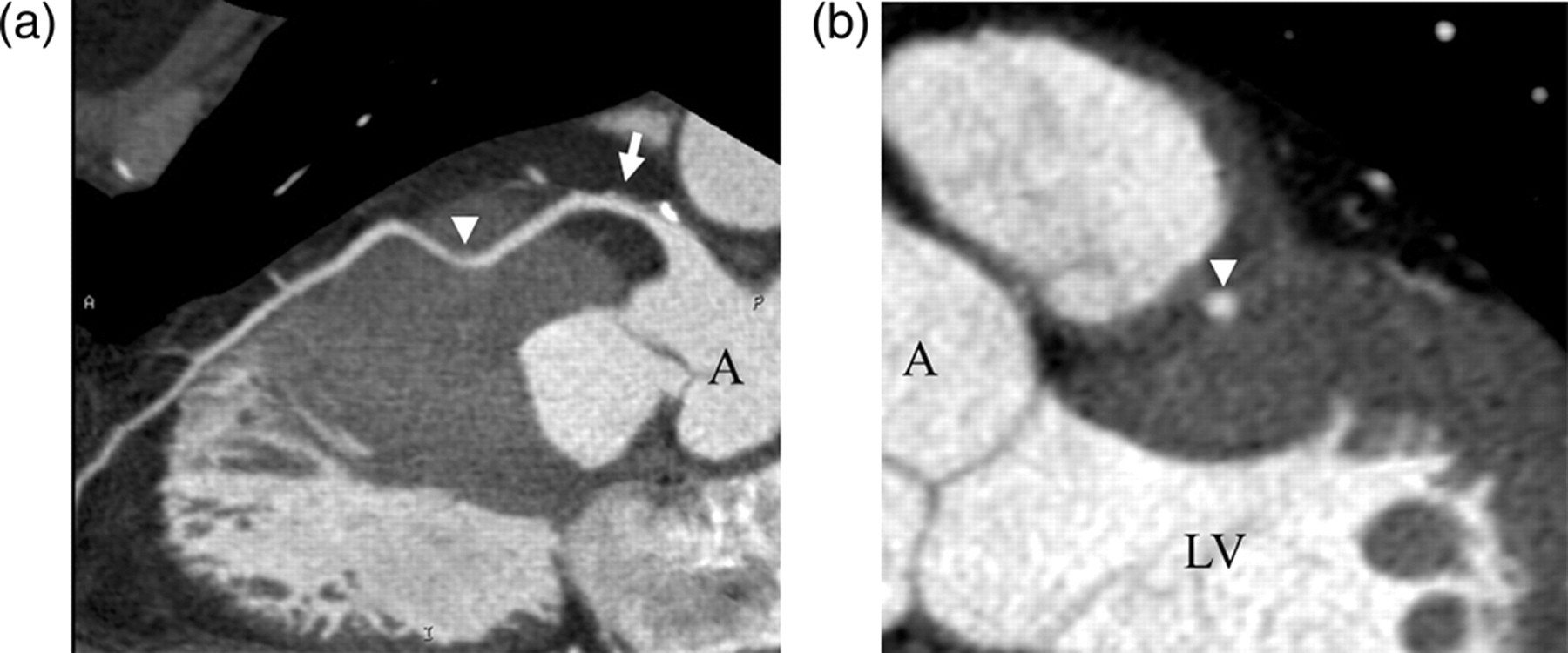
64-slice mutidetector CT coronary angiography images of a myocardial bridge. Curved reformatted (a) and true short axial (b) images of the left anterior descending artery (arrow) show tunneled 3 cm coronary artery segment in the mid LAD which is surrounded by thick myocardium (arrowhead). A = aorta, LV = left ventricle
Variations of intrinsic coronary arterial anatomy
LAD = left anterior descending artery
It was found that there was a type 1 dual LAD in 29 patients (Fig. 4a). In another two cases, short and long LAD originated from the LMCA separately (Fig. 4b). Coronary artery ectasia was found in 2% of the patients, of which 47.6% was located in the RCA, 21.4% in the LCX, 19% in the LAD, 4.8% in two major coronary arteries, and 2.4% in three major coronary arteries (Fig. 5). The mean diameter of coronary ectasia-aneurysm was 6.3 mm (4.4–11.2 mm). The percentage of coronary atherosclerosis was higher in patients with coronary ectasia-aneurysm (n = 42) than the patients who did not have coronary ectasia-aneurysm (2054 patients) in our study (90.5% vs. 72.2%, P = 0.000). No significant correlation among coronary atherosclerosis, MB, and dual LAD was found (P > 0.05).
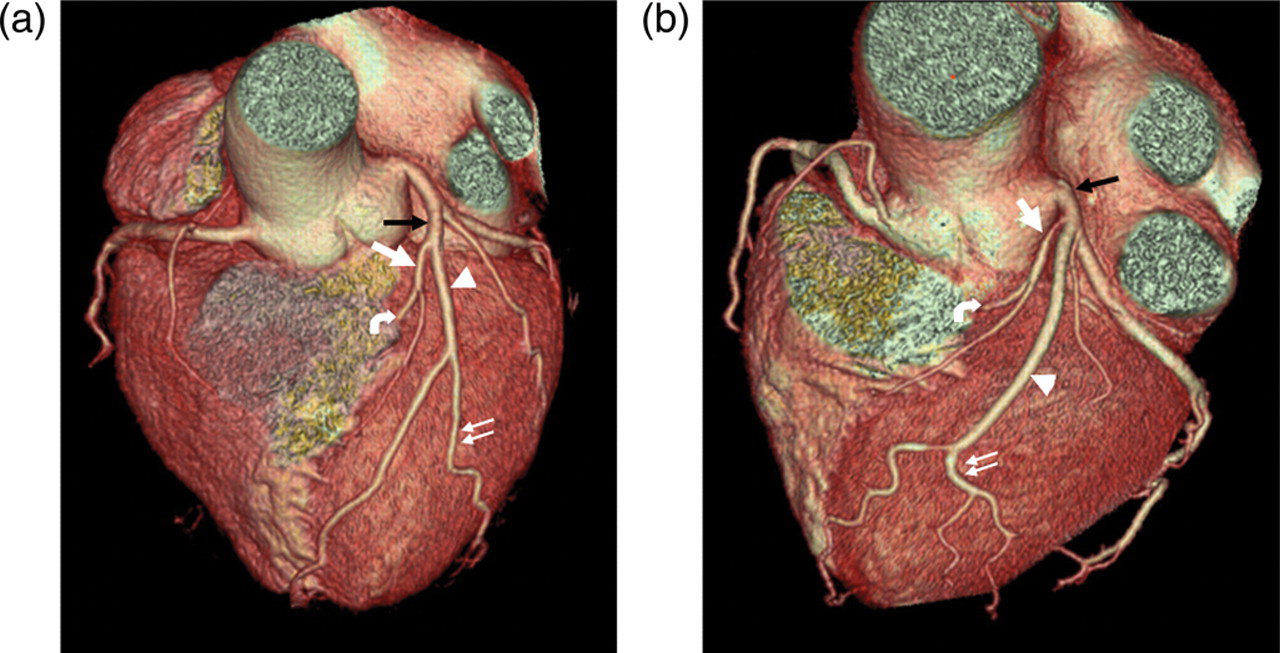
(a) A typical type 1 dual left anterior descending artery (LAD) is seen in a 56-year-old woman with chest pain. Three-dimensional volume-rendered image of the heart shows that short LAD (white arrow) originates from the LAD proper (black arrow) and terminates in the mid anterior interventricular sulcus after giving a septal branch (curved arrow). Long LAD (arrowhead) arises from the LAD proper (black arrow), courses on the left ventricular side of the short LAD, gives off a diagonal branch (double arrows) and re-enters the anterior interventricular sulcus at the distal part. (b) This is a case of variant dual LAD type 1. The three-dimensional volume-rendered image of the heart shows that short (white arrow) and long (arrowhead) LAD originates directly from the left main coronary artery (LMCA) (black arrow) and take the same route and give the same branches as seen in (a). The only difference between two images is the lack of LAD proper as the variant type
(a) Three-dimensional volume-rendered image of the coronary tree shows that the proximal left anterior descending artery (LAD) (arrow) and the distal right coronary artery contain ectatic segments. (b) Curved maximum intensity projection image shows fusiform ectasia of the proximal LAD (arrow)
Discussion
Basic knowledge of the normal coronary artery anatomy and familiarity with its common variations are essential in order to assess CCTA accurately (5, 6). The origin and 3D course of the coronary artery and structural relationship with other cardiac structures are important in the evaluation of coronary artery variations and anomalies and these data are best portrayed by MDCT (6). CCA is a 2D and invasive imaging technique in which selective catheterization and determination of coronary artery anomalies is possible in only 31–55% percent of cases (7, 8). CCTA is a non-invasive cardiovascular imaging technique which is superior to CCA due to its multiplanar postprocessing capability and ability to show the origin, complex 3D anatomy, course and termination of the coronary arteries, and it has become the gold standard to image coronary artery anomalies (1, 6, 7).
The incidence of coronary artery dominancy is variable in the literature because of different definitions of co-dominancy (9). We used the dominancy system, which was defined originally by Schlesinger (10), who described co-dominancy as a state where branches from both the distal RCA and the distal LCX perfuse the posterior interventricular septum. However, some authors define co-dominancy as a state where the PDA originates from the RCA, and the postero-lateral branch artery from the LCX (5). The reported incidence of right dominancy is 70% to 89%, left dominancy 7% to 13% and co-dominancy 2.5% to 20%, all of which are in concordance with our results (5, 9, 11–13).
The RCA normally arises from the RCS. The conus artery is the first branch of the RCA in most of the cases, or otherwise has an origin directly from the aorta (11.6–22%) (1, 9). In our study, a separate origin of the conus artery from the RCS was seen in 17% of the cases, and was much more common in men than women (P = 0.009). The conus artery arising separately from the RCS may sometimes cause problems during ventriculostomy used to treat ventricular septal defect or pulmonary stenosis (14).
The sinoatrial node artery originates from the RCA as the second branch in 55–60% of patients and from the proximal LCX artery in 40–45% of the population (6, 15). In the present study, the sinoatrial node artery originated from the RCA in 65.3%, and from the LCX in 34% of cases. It was also found that the sinoatrial node artery can originate directly from the LCS, RCS, LMCA, or from the ascending aorta in a small percentage of patients (0.7%). The atrioventricular node artery generally originates from the dominant coronary artery.
The LMCA arises from the LCS, is normally 5–20 mm long, and bifurcates into the LAD and LCX arteries (16). In the present study, an LMCA shorter than 5 mm was found in 4.7% of the cases. This is accepted as a normal variant without clinical significance (9). The most common variation in the LMCA anatomy is the intermediate artery that arises from the LMCA as the third vessel between the LAD and LCX and is seen in approximately 30% of the cases (5, 9). In accordance with previous studies, the prevalence of the intermediate artery was 31.3% in our study, and it was much more common in men than women (P = 0.000).
Coronary artery anomalies are reported in approximately 1.3% of patients undergoing CCA (17). Subtle and clinically unimportant coronary artery anomalies that may have otherwise remained undiagnosed by CCA can be detected by MDCT. The reported coronary artery anomaly incidence is higher with CCTA and ranges between 0.7% and 18% (1, 3, 13). In the majority of studies, reported coronary artery anomalies were predominantly anomalous origin and course of the coronary arteries, and rarely fistulous terminations (3). However, there are no sufficient CT data regarding anomalies in the intrinsic coronary arterial anatomy.
Normal coronary arteries lie within the epicardial fat, but may sometimes burrow into a band of myocardial muscle, in a phenomenon named MB. MB is a benign congenital anomaly which is asymptomatic in most cases and diagnosed incidentally during CCA or CCTA (3). Systolic compression and narrowing of the tunneled segment of the coronary artery was reported in 0.5–12% of patients undergoing CCA, and angina pectoris, myocardial infarction, malignant arrhythmias, and sudden death have been reported in rare instances (18). It is most commonly localized in the middle segment of the LAD (18, 19). CCA was the standard and accepted diagnostic modality for MB, at which a typical ‘milking’ effect and a ‘step down–step up’ phenomenon induced by systolic compression of the tunneled segment are diagnostic (20). The great difference in the incidence of MB between autopsy series (15–85%) and CCA series (0.5–16%) indicates that CCA is not sensitive enough to detect MB (3, 19–21). The primary cause of this variability may be the benign nature of MB thus meaning that in many cases, the patient will never undergo CCA (20). The secondary cause may be the inadequacy of CCA to show superficial MB (20, 21). In contrast, MDCT can give information about coronary arteries and the surrounding myocardium in any plane, and clearly shows the location of the tunneled coronary artery (19, 21). The reported incidence of MB in MDCT studies is between 3.5% and 58% (22–24). The prevalence of MB in this report was 21.6% which is in accordance with the previous MDCT reports. Nearly 97% of MBs were found in the LAD artery, and the most common segment was the mid LAD (76%).
In a CCA study, it is reported that a dual LAD is seen in 1% of normal population and is classified into four groups (25). In all types, the proximal LAD (LAD proper) bifurcates into the short and long LADs. The short LAD terminates in the anterior interventricular sulcus before reaching the apex of the heart, and the long LAD re-enters the anterior interventricular sulcus at the distal part, coursing to the apex. The short and long LADs mainly supplies the septal wall and the apical wall, respectively (26). The long LAD courses on the left ventricular side of the short LAD in type 1, and on the right ventricular side of the short LAD in type 2. In type 3, the long LAD has a proximal intramyocardial course in the ventricular septum, and appears on the epicardial surface in the distal part of anterior interventricular sulcus. The distinct feature of type 4 is origination of the long LAD from the RCA (25). We have detected 29 cases of typical dual LAD type 1 with a prevalence of 1.38% that is higher than that reported in the CCA literature and to the best of our knowledge, this is the highest type 1 dual LAD prevalence rate reported with CCTA. The presence of a long and short LAD originating separately from the LMCA in two patients has not been published before in the literature, so we suggest that this anomaly be classified as a variant of the type 1 dual LAD. The radiologist who is reporting preoperative MDCT of the coronary artery should be familiar with and attentive to the presence of a dual LAD, and should forewarn the cardiac surgeon about which branch of the dual LAD is diseased in order to prevent an incorrectly placed arteriotomy (9, 26).
When a coronary artery diameter exceeds 1.5 times or more the diameter of the adjacent normal arterial segment, it is known as a focal or diffuse ectasia-aneurysm of the coronary artery (3). Coronary artery aneurysms are commonly associated with Kawasaki disease, lupus, and atherosclerotic coronary artery disease, are a component of rare inherited genetic syndromes, and also may have a rare congenital etiology (3, 27). The prevalence of aneurysmal coronary disease is 2% in this study, which is in accordance with the previous angiographic study indicating a prevalence of 2.7%, surgical study with 4.9%, autopsy study with 1.4%, and MDCT study with 2% (28–31). We found that the majority of coronary artery ectasia-aneurysms are located in the RCA, which is compatible with the literature (32). Coronary ectasia-aneurysm carries a risk for thrombosis, rupture, myocardial ischemia, and fistulous communication with neighboring structures (3). Our study group was of a certain age and not a highly selected group as the main indication of CCTA was the investigation of ischemic heart disease. Coronary ectasia-aneurysms are assumed to be a variant of occlusive coronary atherosclerosis and we could not find any strict CCTA criteria in the literature to determine the etiology of the coronary ectasia-aneurysm (29, 30). Detection of higher concomitant atherosclerosis with coronary ectasia-aneurysm in our work also supports these studies. In light of this information, we conclude that this ratio is the prevalence of coronary ectasia-aneurysm which is independent from underlying etiology, not the prevalence of real congenital coronary ectasia-aneurysm. Clinically-oriented studies and radiologic–pathologic correlation should be planned for this purpose.
Angelini (13) proposed and classified the variability of the coronary arterial tree with following definitions: normal is any morphological feature observed in more than 1% of an unselected population; a normal variant is an alternative, relatively unusual morphological feature seen in greater than 1% of the same population; and, anomaly is a morphological feature seen in less than 1% of that population. When this definition is applied to our study, the type 1 dual LAD and MB can be classified as normal variants. For MB, this conclusion comes from a statistical result and to disclose clinical importance of MB, prospective, long-term, and clinically-oriented studies are needed.
This is one of the largest MDCT studies on intrinsic coronary artery variations in the literature (1, 2, 5, 7–9, 12, 19, 22–24, 28, 33). Recently, Andreini et al. (34) and Bazzocchi et al. (35) published similar retrospective studies performed with 64-slice MDCT. The sizes of the population in these two studies (2757 patients and 3236 patients, respectively) are slightly larger than that of our study (2096 patients). However, the results of those studies are slightly different from that of our study. Regarding MB, all three studies agree that MB is a normal variant although the frequency of each report is slightly different (9.8% vs. 3.2% vs. 21.6%, respectively). On the other hand, regarding aneurysm, Andreini et al. (34) reported 1.1% and Bazzocchi et al. (35) reported 0.7%. Regarding type 1 dual LAD, Bazzocchi et al. reported 0.06%. Those different results might be due to different genetic and geographic backgrounds of the study population or due to study population number too small to estimate the actual prevalence in the general population. This study adds the results of a similar sized group and confirms that the prevalence of normal coronary variants is different among different groups.
The main limitations of this study are its retrospective design and lack of clinical and CCA correlation. However, it has been shown that there is no need to correlate CCTA with CCA because of the high sensitivity of MDCT in the visualization of normal and abnormal coronary vessels (8, 33). Although 5 years of cardiovascular radiology experience is enough for the evaluation of CCTA images, presence of only one reader is another limitation of our study.
In conclusion, CCTA is a non-invasive imaging modality to show complex coronary artery anatomy and variations of intrinsic anatomy of the coronary arteries. The incidence of coronary artery variations is high and various, and the readers should be familiar and looking for these conditions during interpretation of CCTA examinations.
Footnotes
Acknowledgments
We thank the 29 May Hospital's radiology technologists for data acquisition and Dr Fatih Kara for statistical consultation, guidance, and data analysis.