
Abstract
Background
Although CT is the modality of choice for morphological lung imaging, an increasing proportion of chest imaging is performed by MRI due to the utilization of whole-body MRI. Therefore, the diagnostic performance of MRI in reliably detecting pulmonary lesions should be established.
Purpose
To investigate the detection rate of pulmonary lesions by MRI that can be expected in a clinical setting and to assess the accuracy of lesion measurement by MRI compared to CT.
Material and Methods
Twenty-eight patients (median age 66 years) with indication for CT imaging due to suspected thoracic malignancy were prospectively included. Chest MRI performed on the same day as CT, comprised unenhanced TrueFisp, ecg-gated T2-weighted HASTE, T1-weighted VIBE, and contrast-enhanced T1-weighted, fat-saturated VIBE sequences. MR sequences were evaluated for lesion detection by two readers independently and measurement of lesion size was performed. MR findings were correlated with CT.
Results
One hundred and eight pulmonary lesions (20 thoracic malignancies, 88 lung nodules) were detected by CT in 26 patients. Lesions were ruled out in two patients. All thoracic malignancies were identified by MRI with strong correlation (r = 0.97−0.99; P < 0.01) in lesion size measurement compared to CT. Unenhanced, T1-weighted VIBE correctly classified 94% of thoracic malignancies into T-stages. Contrast-enhanced, T1-weighted VIBE performed best in identifying 36% of lung nodules, 40% were detected combining unenhanced and contrast-enhanced T1-weighted VIBE. Detection rate increased to 65% for the combined sequences regarding lesions ≥5 mm. Lesion size measurement by all MR sequences strongly correlated with CT (r = 0.96−0.97; P = 0.01).
Conclusion
MRI is as accurate as CT in detection and size measurement of primary thoracic malignancies >1 cm in diameter. If a lung lesion is detected by MRI, it is a reliable finding and its measurement is accurate. CT remains superior in detecting small lung nodules (<6 mm). Detection rate of MRI for small lesions is improved using a multi-sequence protocol including contrast administration.
Morphological imaging of the lung is the domain of computed tomography (CT), which is the method of choice in clinical routine. CT allows for visualization of anatomical details of lung parenchyma and detection of small pulmonary lesions. It is therefore suited for imaging of lung diseases like fibrosis or emphysema and for staging purposes in oncologic imaging. Magnetic resonance imaging (MRI) of the chest has evolved as an important method for functional imaging, e.g. assessing lung perfusion and ventilation (1). However, MRI has also been reported to be superior to CT in selected morphological aspects like differentiating atelectasis from tumor in the feeding bronchus such as bronchial carcinoma (2, 3).
Therefore, it is important to assess the overall diagnostic performance of MRI in detection and characterization of lung pathology in a routine clinical setting. There are various studies in the literature focusing on the detection of lung lesions by using different MRI sequences at 1.5 or 3 Tesla field strength. These articles reported differing detection rates depending on the lesions investigated, for example a range of 35–84% for lesions smaller than 5 mm (4–12).
In the context of these diverging results, the purpose of this study was to assess the accuracy of lesion detection by MRI compared to CT that can be realistically expected in the clinical routine. We further examined lesion size measurement using various MRI sequences to evaluate its reliability for lesion characterization and T-staging.
Material and Methods
The prospective study design was approved by the local ethical committee and all patients gave informed consent.
Patients
We prospectively included 28 patients (median age 66 years, 16 men, 12 women) with suspected thoracic malignancy and clinical indication of diagnostic CT imaging of the chest. Exclusion criteria were contraindications to CT or MR imaging such as contrast allergy, renal function impairment or insufficiency (estimated glomerular filtration rate <40 mL/min), and medical implants such as cardiac pacemaker. Patients underwent CT and MRI of the chest on the same day. CT served as the reference standard for lung lesion detection by MRI. Findings were compared to surgery or lung biopsy if performed.
CT
Scanning was performed on a 64-slice CT scanner (Somatom Definition, Siemens, Forchheim, Germany). The scan area was planned on the scout scan ranging from the apex of the lungs to the upper abdomen. Sixty mL of contrast material (Iopromide 370 mg/mL, Ultravist, Bayer HealthCare, Berlin, Germany) was injected using a power injector (Stellant, Medrad, INC., Warrendale, PA, USA) via a 20-gauge cubital venous access at a flow rate of 3 mL/s. Scan start was timed by bolus tracking using a region of interest (ROI) placed in the ascending aorta and a scan delay of 4 s after reaching a contrast enhancement threshold of 60 Hounsfield units (HU). Scan parameters were as follows: 64 × 0.6 mm collimation, 15 mm table feed per rotation, initial value of 320 milliampere second for automatic tube current modulation (reference mAs), 120 KV tube voltage. Image reconstruction using a field of view adjusted to the outer margins of the chest was performed in axial orientation with 3 mm slice thickness (ST), 2 mm increments, and a medium (B30f) as well as hard (B70f) convolution kernel.
MRI
Image acquisition was performed on a 1.5 Tesla MR scanner (Avanto, Siemens, Erlangen, Germany) equipped with a 45 mT/m gradient system (slew rate 200 T/m/s) using a standard phased-array surface coil with 6 elements for signal reception. The scan protocol comprised unenhanced sequences, single-shot TrueFisp (fast imaging with steady state precession), ecg-gated T2-weighted HASTE (Half Fourier Acquisition Single shot Turbo spin Echo [TSE]), T1-weighted VIBE (Volumetric Interpolated Breath hold [bh] Examination), and a contrast-enhanced (venous phase) T1-weighted, fat saturated VIBE (Table 1). Contrast material, 0.1 mmol/kg gadopentetate-dimeglumine (Magnevist, Bayer HealthCare, Berlin, Germany), was administered at a flow rate of 3 mL/s using a power injector (Spectris Solaris, Medrad, INC., Warrendale, PA, USA) via the cubital access established for CT.
MR sequence parameters. All sequences were solely acquired in axial orientation to allow for a short examination protocol, familiar image interpretation and for correlation with CT. Number of excitations = 1, parallel imaging factor = 2 for all sequences
Image evaluation
Image data were analyzed by two experienced radiologists (5 and 12 years of experience in chest radiology) independently of each other on diagnostic workstations (Centricity Radiology RA1000, GE Healthcare, Milwaukee, WI, USA).
Lesion detection
First, each MRI sequence was evaluated for detection of lung lesions in random order and at standardized window settings (TrueFisp 231, 552; T2 HASTE 392, 866; native VIBE 131, 253; contrast-enhanced VIBE 173, 336 [center, width]). If disagreement occurred, the negative result, e.g. that a lesion was not detected, was chosen. This careful approach was deliberately chosen to meet the probability of missing a lesion and to have a high threshold in detecting true lesions instead of artifacts.
Lesion measurement
For any detected lesion, the location was noted and the longest diameter measured. Lesion measurement was done in consensus using the digital calliper of the diagnostic workstation.
Comparison to CT
Once the MRI reading was completed CT data were evaluated for lung lesions by both observers in consensus. Each lesion was recorded with its location and the longest diameter was measured at standard lung window settings (center –498, width 1465).
Finally, results of MRI lung lesion detection were compared one-to-one to the CT data. CT images were displayed on one screen and MRI images on the second screen of a dual-monitor diagnostic workstation. For each MRI sequence, it was recorded if a lung lesion was identified in concordance to CT. In case a lesion was not initially detected by MRI during the reading, it was noted if it could be retrospectively identified. In case of lung cancer, the T-stage of the lesion for CT and each MRI sequence was classified solely based on lesion size according to the seventh edition of the TNM classification of lung cancer (13).
Statistical analysis
Data are presented in absolute and relative numbers with standard deviation and range. The diagnostic accuracy of MRI was expressed as proportion of lesions detected by MRI in comparison to lesions identified by CT. Specificity and sensitivity have not been calculated since the high ratio of lesion positive patients compared to patients without lesions would render these parameters artificially high. A relation between values was assessed by Pearson's correlation coefficient. An error probability of P < 0.05 was considered to be statistically significant. Bland-Altman plots were calculated to analyze agreement of measurements between CT and MRI (14). Statistics including t-test were calculated using commercially available software (PASW Statistics 18.0, SPSS Inc., Chicago, IL, USA).
Results
A total of 108 lung lesions were detected by CT in 26 of 28 patients of the study group, in detail 20 primary thoracic malignancies and 88 lung nodules. Lung lesions were ruled out by CT in two patients. Primary malignancies (lung cancer = 17; primitive neuroectodermal tumor = 1, angiosarcoma = 1, thymic cancer = 1) were proven by either surgery (n = 19) or lung biopsy (n = 1). Lung metastasis secondary to renal (n = 3) or rectal (n = 1) cancer were observed in four patients. In one patient, a lung lesion was a manifestation of tuberculosis proven by histopathology based on the surgical specimen. In a further patient, a solitary lung nodule was monitored over a 36-month period without change in size and therefore was considered as a granuloma.
Primary thoracic malignancies
Lesion detection
All primary thoracic malignancies were correctly detected by MRI.
There was no difference of performance between the MR sequences (TrueFisp, T2-weighted HASTE, T1-weighted non-enhanced and T1-weighted, fat-saturated contrast-enhanced VIBE) and a 100% accuracy was measured for each sequence.
Accuracy of measurements
The mean lesion size measured by CT was 55 ± 20 mm ranging from 21–106 mm. The correlation (Pearson's) between measurement of longest diameter by CT compared with each MR sequence was strong (r = 0.97–0.99) and significant (P < 0.01) for all four MR sequences (Table 2, Fig. 1). The mean difference in the lesion measurement of lung cancer compared to CT was 3 ± 5 mm for TrueFisp, 3 ± 4 mm for T2-weighted HASTE (T2w-HASTE), 1 ± 3 mm for unenhanced T1-weighted VIBE (T1w-VIBE), and 2 ± 4 mm for contrast-enhanced, fat-saturated T1-weighted VIBE (ce-T1w-VIBE) sequence (Fig. 1).
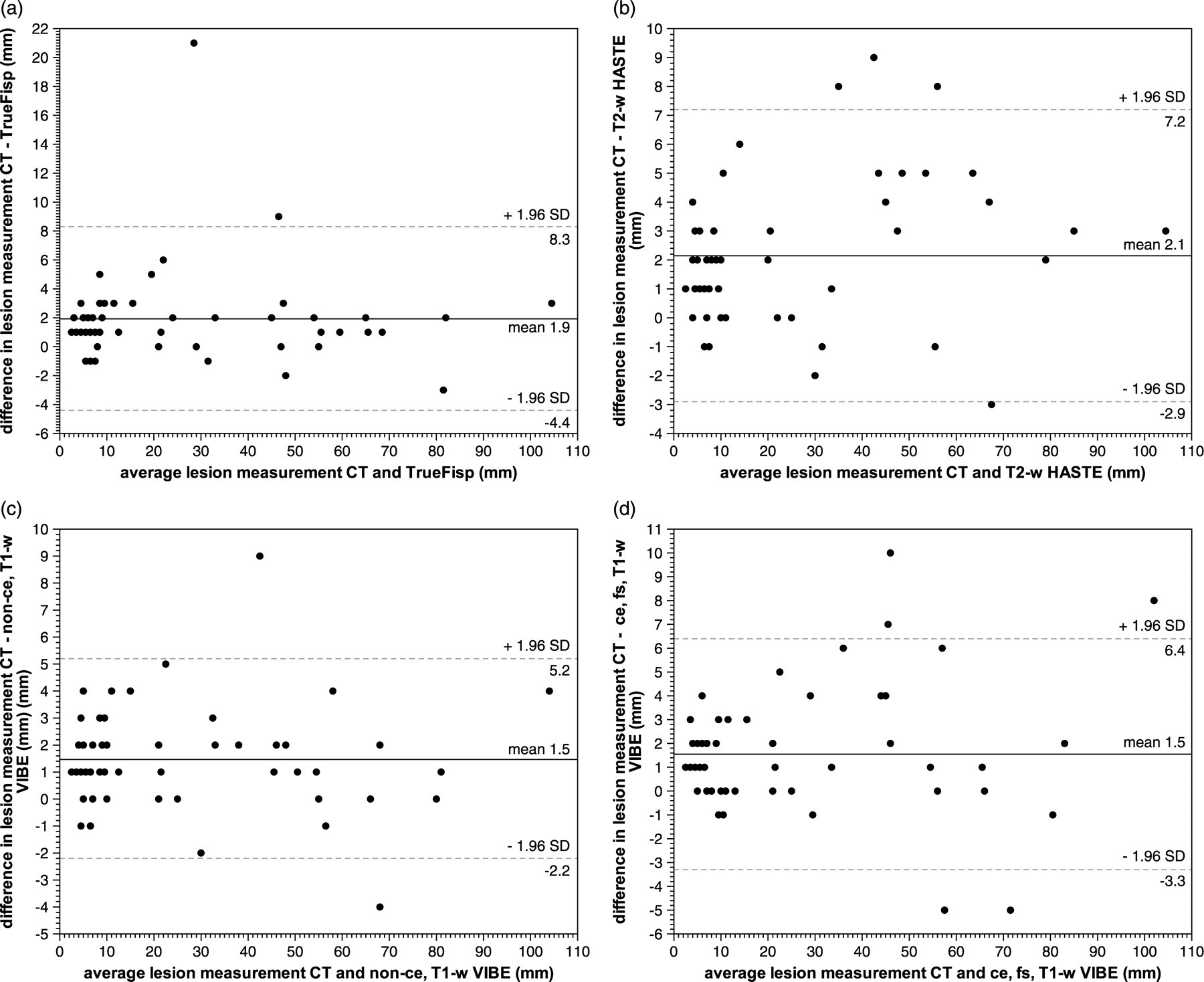
Bland-Altman plot of difference and average of nodule and tumor measurements by CT and (a) True Fisp, (b) T2-w HASTE, (c) T1w-VIBE, and (d) ce-T1w-VIBE MR sequences
Correlation of MRI tumor measurement with CT and accuracy of T-stage designation solely based on size for each MRI sequence
*Significant on the level of P = 0.01 (Pearson's correlation)
T-stage designation of lung cancer solely based on lesion measurement by CT revealed two cases that were classified as T1b, six as T2a, eight as T2b, and one case as T3. T1w-VIBE sequence performed best in T-staging if compared to CT with 94% accuracy. TrueFisp, T2w-HASTE, and ce-T1w-VIBE reached 82% accuracy, respectively (Table 2). Only one case was incorrectly classified by T1w-VIBE sequence into a higher T category, CT measured 29 mm (T1b) in contrast to T1w-VIBE with 31 mm (T2a).
Lung nodules other than primary thoracic malignancies
Lesion detection
A mean of 4 ± 5 lesions (range 1–18) per patient were detected by CT in 20 patients. The mean lesion size measured by CT was 6 ± 5 mm (range 2–25 mm). Accuracy for lung nodule detection was best with 40% combining T1w-VIBE and ce-T1w-VIBE sequences, no other combination of two or more sequences yielded better results. Accuracy for each sequence is given by Table 3. If lung nodules ≥5 mm were regarded, the accuracy increased to 60% for ce-T1w-VIBE sequence alone and to 65% for the combination of T1w-VIBE and ce-T1w-VIBE (Table 3). Overall 53 of 88 (60%) lung nodules were not detected by MRI initially, while 17 of these 53 initially undetected nodules were identified in retrospect. Including lesions retrospectively detected, accuracy increased to 59% (Table 4). No false-positive detection by MRI occurred. MRI was concordant with CT in ruling out any pulmonary lesion in two patients.
Detection rates of lung nodules for each sequence with mean size of detected vs. undetected lesions as well as mean difference and correlation of MRI measurements compared to CT
*Significant difference between detected and undetected lesions (P < 0.001, t-test)
†Significant on the level of P = 0.01 (Pearson's correlation)
Overall detection rate of lung nodules (if any MR sequence detected lesion) classified by lesions size according to the Fleischner society (19)
The mean lesion diameter of initially undetected nodules (including retrospectively detected) was significantly lower (P < 0.001) with 5 ± 3 mm compared to detected lesions with 9 ± 5 mm. The size of nodules retrospectively detected in correlation with CT was 6 ± 5 mm compared to 4 ± 2 mm of nodules that were not detected at all by MRI. Sixty-six percent (35/53) of the missed lung nodules were smaller than 5 mm, 10/53 measured 5 mm, and 6/53 had a diameter between 6 and 10 mm. One large pulmonary lesion with 25 mm in diameter identified as endobronchial mucus plug by CT was missed by MRI due to low signal intensity. The largest undetected solid lesion was 11 mm in diameter. Eleven lesions smaller than 5 mm, three measuring 5 mm, and two nodules between 6 and 10 mm were retrospectively identified in correlation with CT (Fig. 2, Table 4).
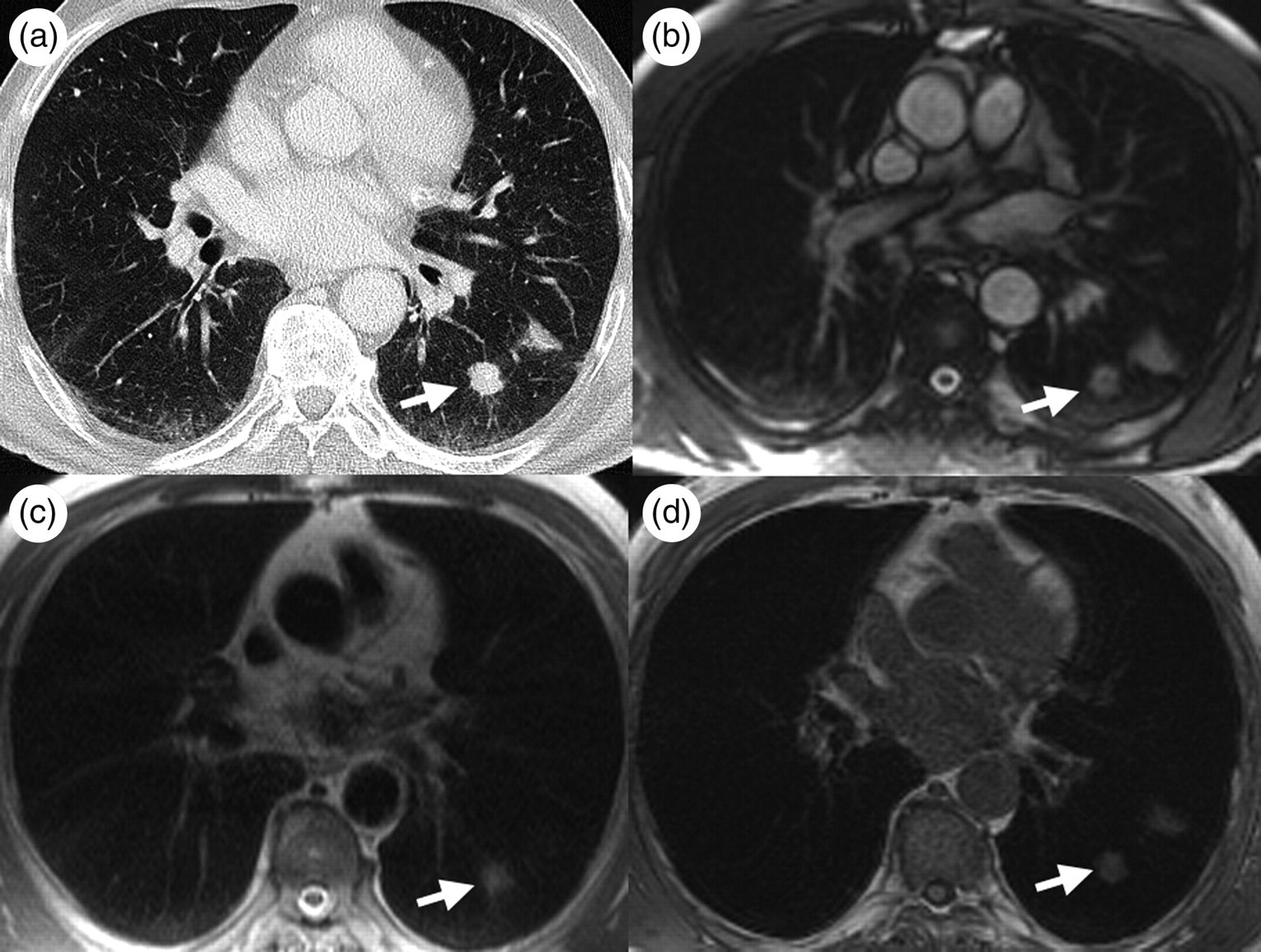
A 67-year-old patient with pulmonary and pleural metastatic disease, secondary to renal cell carcinoma, proven by thoracic surgery. CT (a) shows a solid pulmonary nodule (arrow) neighbored by a structure adjacent to the pleural fissure. Note that both, the pulmonary (arrow) and pleural lesion, are well identified on True Fisp (b) and T1w-VIBE sequences (d), whereas only the pulmonary lesion is conspicuous on ecg-gated T2w-HASTE (c)
Accuracy of measurement
There was a strong and significant (p = 0.01) correlation ranging from r = 0.96−0.97 between lung nodule size measured by CT and by TrueFisp, T2-weighted HASTE, T1w-VIBE, and ce-T1w-VIBE sequences. Bland-Altman plots show the comparison between each sequence and measurements performed on CT (Fig. 1).
Discussion
In this study we could demonstrate that MRI can be used for detection of primary thoracic malignancies with reliable measurement of the lesion size for clinical T-staging (Figs. 2 and 3). All tumors were detected by any of the four sequences which achieved a high T-staging accuracy. Correlation of lesion measurement was strong (r = 0.97–0.99 for primary thoracic tumors and r = 0.95–0.97 for nodules) and significant (P = 0.01) for all sequences.
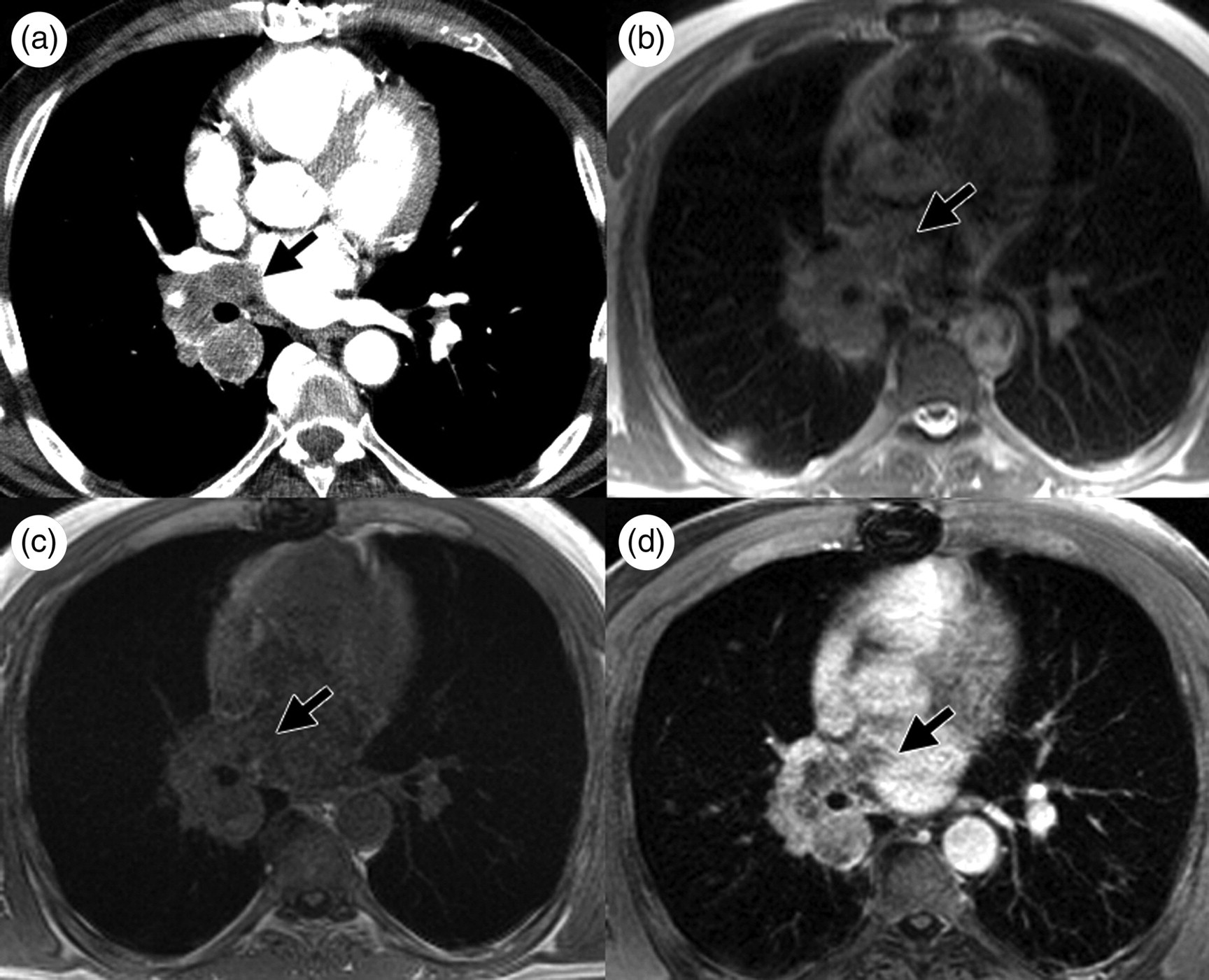
A 66-year-old patient with a central carcinoma invading the right pulmonary veins and left atrium as shown by CT (a). The tumor itself can be identified by T1w-VIBE (c) and T2w-HASTE (b) but the invasion into cardiac structures (arrow) is difficult to assess. Ce-T1w-VIBE (d) accurately delineates the tumor margin in comparison to CT
Lung nodule detection for lesions ≥5 mm was 59% for ce-T1w-VIBE sequence and 65% for the combination of T1w-VIBE and ce-T1w-VIBE. Overall detection rate of all lesions with a mean size of 6 mm (2–25 mm) was as low as 40% for the combination of T1w-VIBE and ce-T1w-VIBE. Combination of these two sequences proved to have the best accuracy compared to a single sequence or any combined protocol of three or four sequences.
However, 60% of lung nodules were initially missed by MR while there were no false-positive findings. The mean lesion size of initially missed nodules (5 mm) and retrospectively identified lesions (6 mm) differed significantly from detected nodules with 9 mm. A proportion of 19% of initially undetected lesions was identified retrospectively in direct correlation with the CT (Fig. 4). Therefore, the presented study data seem to support a size of 6 mm as an adequate threshold for secure lesion detection by MRI.
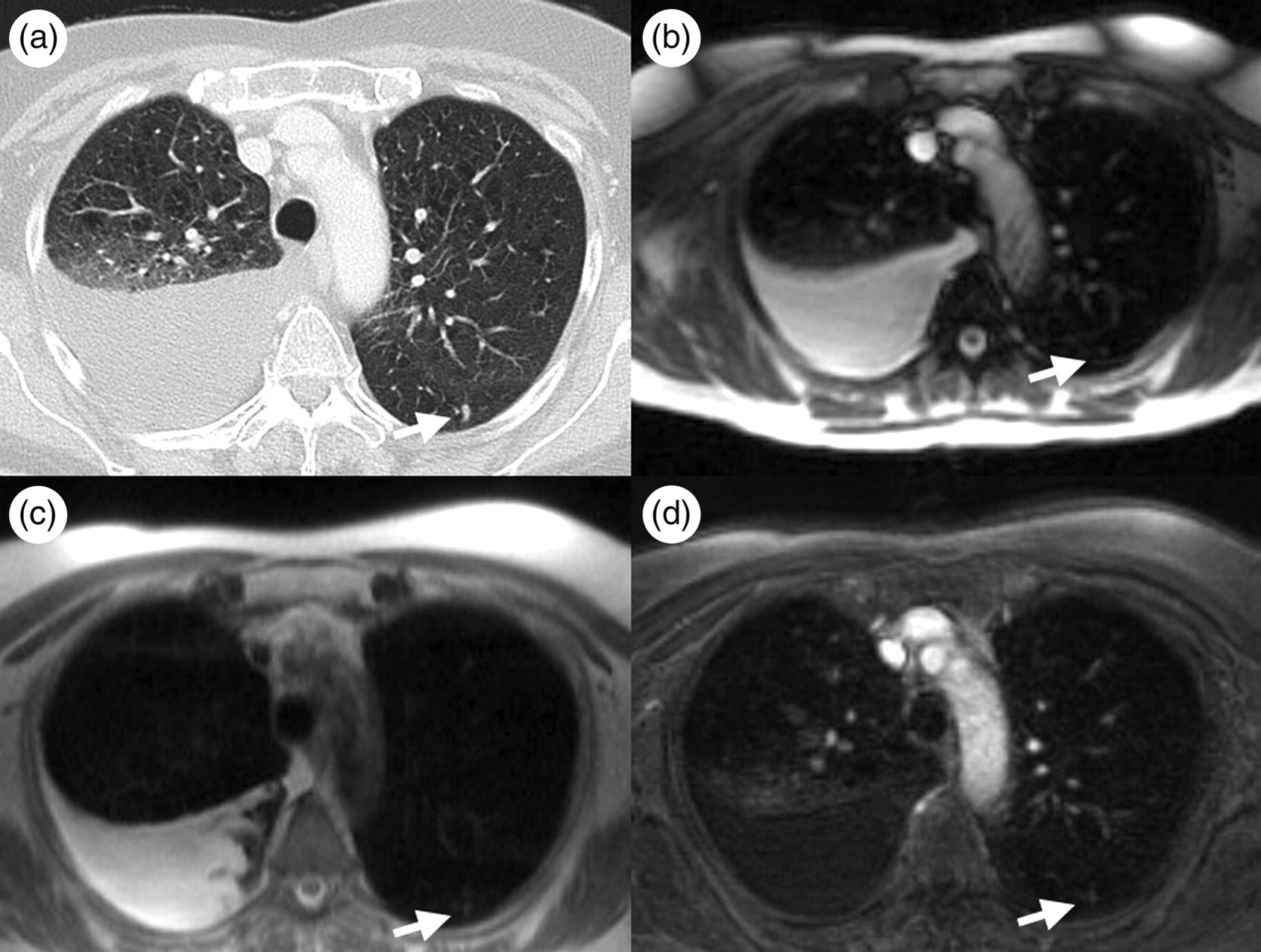
A 69-year-old patient with primary lung carcinoma located in the right lower lobe and consecutive right sided pleural effusion. CT (a) detected a small, 4 mm pulmonary nodule in the apical segment of the left lower lobe (arrow). This pulmonary lesion was retrospectively identified in correlation to the CT; it is faintly visible on TrueFisp (b), T2w-HASTE (c), and ce-T1w-VIBE sequences (d)
Hence, lesion size is one crucial parameter defining detectability and is essential for comparing studies which address this topic.
In a study performed by Both et al., T1w-VIBE detected 80% (12/15) of lesions ranging from 3–21 mm in size, while T2w-HASTE detected 60% (9/15) (2). The minimum detectable lesion size was 4 mm for T1w-VIBE and 5 mm for T2-weighted HASTE. The difference in the detection rate could be explained by the proportion of smallest lung lesions in our study, 42% were ≤4 mm and 27% between 4–6 mm in size. However, a study by Schroeder et al. investigating a T2w-HASTE sequence with comparable sequence parameters and a high rate of small pulmonary lesion per patient, achieved a detection rate of 73% for lesions <3 mm, 84% for 3–5 mm lesions, 96% for 5–10 mm lesions, and 100% for lesions larger than 10 mm (9). Another study by Vogt et al. using a T2w-HASTE sequence on a 1.5 Tesla system reported a sensitivity of 95% for lesions between 5–10 mm (10). Kersjes et al. reached a detection rate of 36% for lesions smaller than 5 mm using a T2-weighted TSE sequence on a 1.5 Tesla scanner in 1997 (5) but MR technology, with regard to gradient characteristics and receiver-coil channels, has improved since then. These varying detections rates in small pulmonary lesions may be explained by the histological character of the lesions. Schroeder et al. investigated a study population with 1102 lesions in 30 patients with pulmonary metastasizing malignancies (9). Aside from lesion size, signal intensity (contrast-to-noise ratio) is another factor defining detectability. It may be speculated that pulmonary metastasis would present with different, probably higher signal intensity, due to the more solid nature than for instance a small granuloma (15). Theoretically, a concurrent chemotherapy would further increase signal intensity on T2-weighted sequences as a result of cytotoxic edema. A recent study by Yi et al. at 3 Tesla found relatively low detection rates of 35% for T1-weighted and 36% for T2-weighted sequences for lesions between 3–5 mm, which is comparable to this study's detection rate of 35.3% for combined results of unenhanced and contrast-enhanced T1-VIBE (12). The differences in the reported studies at 1.5 and 3 Tesla scanners may be explained by different patient populations but demand for a reasonable appreciation of expectable detection rates in the clinical context. The approach of this study, to classify a lesion as undetected if one of the two observers did not identify the lesion, is lowering the detection rate but may be closer to a clinical setting by reflecting the lower but more realistic end of the achievable accuracy. In contrary to the cited literature there were no false-positive findings in this study. As a consequence, detection of a pulmonary lesion by MRI using a cautious approach is a reliable finding. Conversely, MRI to date cannot securely rule out lung lesions smaller than 6 mm. However, a phantom study by Biederer et al. has shown that MR sequences, especially 3D gradient-recalled echo sequences such as the VIBE sequence, have the potential to detect small pulmonary nodules (< 5 mm) with a high sensitivity and specificity (93% and 86%, respectively) (16).
The more MRI of the chest becomes clinically applicable, for instance in whole body MRI, the more it is important to know which sequences to implement for chest imaging and whether contrast administration is necessary (17, 18).
The management of a pulmonary lesion incidentally detected by MRI is dependent on the lesion size according to a statement of the Fleischner society (19). In order to appropriately manage a lesion, it is necessary to assess the accuracy of lesion size measurement by MRI. Reasons for imprecise measurement may be due to regions of low signal intensity in partially solid lesions mimicking a smaller lesion as well as low spatial resolution. As a result, a MRI protocol for patients with suspected pulmonary malignancies should comprise at least one unenhanced and one contrast-enhanced sequence, such as T1w-VIBE and ce-T1w-VIBE.
This study has several limitations. The study utilized CT as the standard of reference instead of histopathology. However, CT is a widely accepted method to detect lung lesions and a one-to-one comparison of MRI with histopathology would be difficult due to changes in volume and orientation induced by specimen fixation postoperatively. Additionally, a consensus reading for lesion measurement may be criticized since it does not assess agreement between multiple readers, but this study was focused on variability introduced by the MR sequences and a consensus reading may be found in most of the clinical settings, e.g. resident and attending constellation.
To allow for better comparison with CT, only axial MR image acquisition was performed. Maybe a second acquisition orientation would have been helpful to increase the sensitivity of MRI. Additionally, the patient population was small and a great proportion of patients with pulmonary malignancies or metastasis was present, which implies a high probability of further pulmonary lesions. In order to determine the role of MRI in securely excluding pulmonary lesions a study in a non-selected patient population would be needed. Furthermore, we did not implement DCE-MRI measurements in this study that might improve diagnostic accuracy. However, this issue should be investigated in future studies.
In conclusion, MRI of the chest is as reliable as CT in detection and size depending clinical T-staging of primary thoracic malignancies (e.g. bronchial carcinoma).
Detection of a lung nodule by MRI is a reliable finding, while measurement of lesion size shows good agreement with CT. However, detection rates of lung nodules are low compared to CT. Detection of small lung nodules (<6 mm) by MRI is not reliable in a routine clinical setting. Therefore, MRI is not sufficient in securely excluding lung nodules in a non-selected patient population where these nodules might have a clinical impact.