
Abstract
A catheter port system technique called redistributed subclavian arterial infusion chemotherapy (RESAIC) for locally advanced breast cancer was reported and seemed to be effective for local control and as a palliative treatment. However, when the cancer spreads beyond the medial line to the contralateral chest wall, ipsilateral RESAIC would not achieve a favorable drug distribution. We report on two patients with advanced breast cancer spreading to the contralateral chest wall in whom bilateral RESAIC was attempted. In summary, when advanced breast cancer spreads to the contralateral chest wall, bilateral RESAIC may be useful for local control or palliation.
Locally advanced breast cancer is generally treated by combined modality therapies that include systemic chemotherapy (1, 2). Although arterial infusion chemotherapy is not a standard therapy, it is sometimes performed for downstaging or local control. There are some reports of arterial infusion chemotherapy and a catheter port system, which attained high local control when used as neoadjuvant chemotherapy (70–90%) (3–11).
A new catheter port system technique called redistributed subclavian arterial infusion chemotherapy (RESAIC) was reported to perform arterial infusion chemotherapy simply and continuously. This technique seemed to be effective for local control and as a palliative treatment (12, 13). RESAIC is a technique wherein the tip of the catheter port system (CPS) is placed in the subclavian artery after redistribution of the internal thoracic artery. Arterial redistribution was achieved using a mixture of N-butyl cyanoacrylate (NBCA; Braum, Melsungen, Germany) and lipiodol (LPD; Guerbet, Aulnay-sous-Bois, France). The breast cancer then became supplied mainly from the branches of the axillary and the subclavian arteries. In addition, a sphygmomanometer cuff was used during the injection of the anticancer drugs to prevent perfusion to the arms. With the RESAIC method, it is essential that distribution of the drug encompasses the entire tumor. However, in the cases when the cancer spreads beyond the medial line to the contralateral chest wall, ipsilateral RESAIC would not achieve a favorable drug distribution. We therefore report on two patients with advanced breast cancers spreading to the contralateral chest wall in whom bilateral RESAIC was attempted.
Case reports
Patient 1
A 50-year-old woman with recurrent breast cancer, who had undergone mastectomy on the left side, systemic chemotherapy, and radiotherapy 2 years ago, had severe anemia (hemoglobin 6.0 g/dl) caused by bleeding from the recurrent local lesion. Although conventional selective arterial infusion chemotherapy was performed twice at a previous institution, local tumor control had not been obtained. Pretreatment CT images revealed a very large tumor spreading from the left breast to the right chest wall (Fig. 1a) and right axillary lymph node metastasis. CT angiography showed the development of a collateral arterial blood supply from all directions (Fig. 1b). As the arteries feeding the tumor, both sides of the internal thoracic arteries, branches of the axillary arteries and the inferior epigastric arteries were assumed to be involved. Bilateral RESAIC was therefore attempted.
(a) Pretreatment CT images of patient 1 show a very large tumor spreading from the left breast to the right chest wall. (b) CT angiography revealed the feeding artery came from all directions. (c) The arteriogram of the left intrathoracic artery demonstrated the tumor stain. (d) The arteriogram of the left inferior epigastric artery demonstrated the development and the tumor stain via the left superior epigastric artery. (e) Two indwelling catheters were placed with each tip positioned immediately distal to the ipsilateral internal thoracic artery. (f, g) CT images of patient 1 obtained by the infusion of contrast material via the catheter-port system (right side, f; left side, g) demonstrated enhancement of the entire tumor, which suggested sufficient drug distribution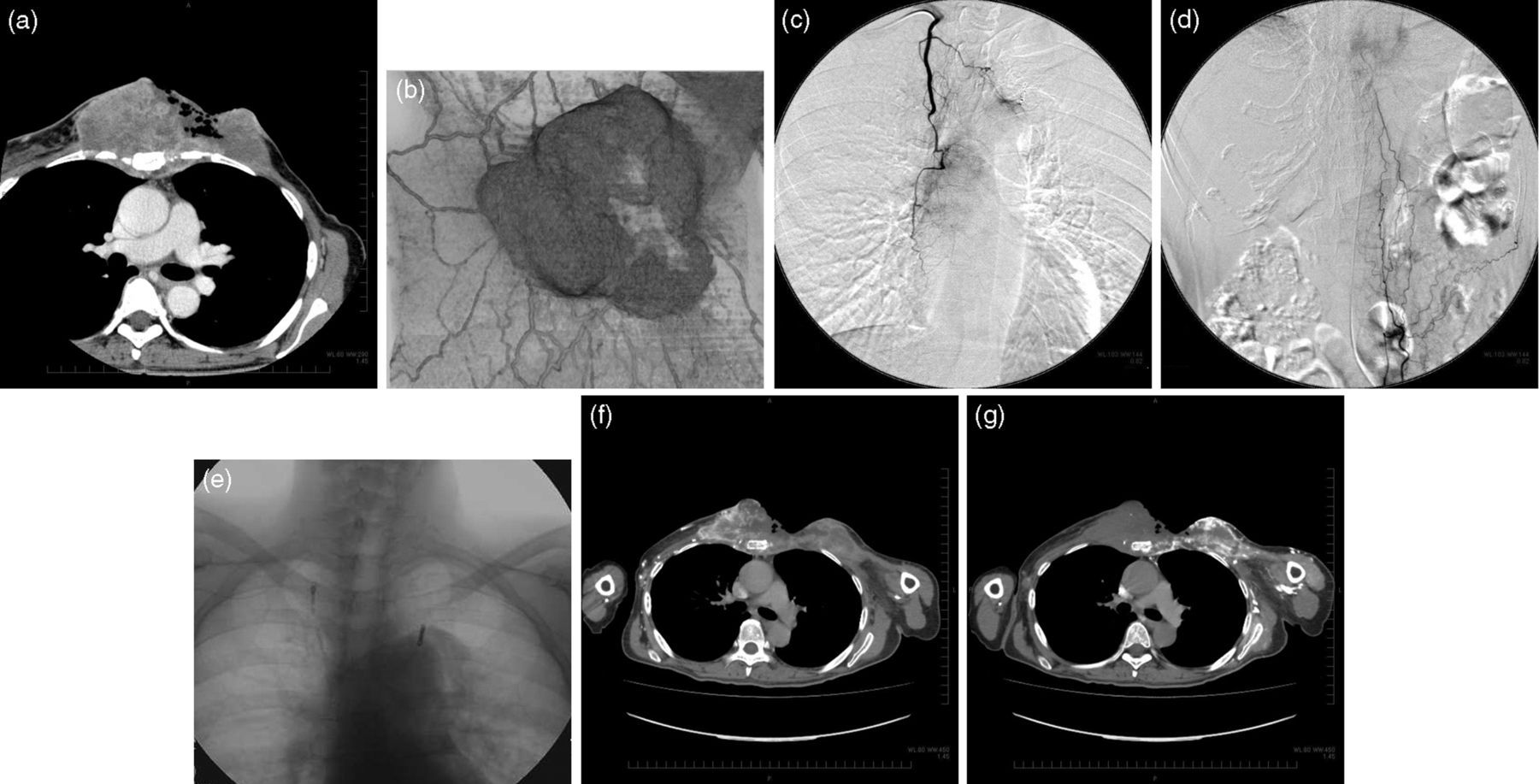
The procedure was performed under local anesthesia via the right brachial artery. Selective angiograms were obtained using a 2.2-Fr microcatheter introduced coaxially through a 4-Fr cobra-shaped, pigtail or headhunter catheter. A right internal thoracic arteriogram revealed a huge tumor in the chest wall (Fig. 1c). A left inferior epigastric arteriogram also revealed tumor stain through the left superior epigastric artery (Fig. 1d). Although the right inferior epigastric artery did not supply the lesion in the chest wall, the development of a collateral blood supply was suspected. The left internal thoracic artery had been embolized by microcoils during a previous treatment. Therefore, the right internal thoracic artery and the right and left inferior epigastric arteries were embolized by a mixture of NBCA diluted eight times with lipiodol for the arterial redistribution. The proximal portion of the right internal thoracic artery was additionally embolized using a few microcoils (Tornado, COOK, Bloomington, IN, USA) of 3–5 or 3–6 mm in diameter. Two long tapered catheters (a distal shaft measuring 3.3-Fr and 60 cm long and a proximal shaft measuring 5 Fr and 40 cm long) (Anthron-PU catheter, Toray, Japan) were placed with each tip positioned just distal to the ipsilateral internal thoracic artery via the right and left brachial arteries (Fig. 1e). The distal end of the catheter was connected to a port (Celsite port; Toray, Japan) and was implanted at the forearm. There were no significant procedure-related complications. Contrast-enhanced CT images obtained by the infusion of contrast material via the bilateral CPSs revealed sufficient drug distribution (Fig. 1f and g).
The regimen was as follows. Epirubicin (EPIR) 40 mg/body was injected at the first treatment. From second treatment onward, the treatment cycle consisted of cisplatin (CDDP) 10 mg/body and 5-FU 1000 mg/body on days 1, 8, and 15 and EPIR 30 mg/body on day 22 of treatment. The reduction in bleeding and pain was apparent a few days after the initial infusion, and arm edema improved as tumor size decreased. The patient experienced an improvement in symptoms such as pain caused by skin ulceration, bleeding, a foul odor, arm edema, and paresthesia. At 3 months after treatment, the tumor had decreased slightly in size from 22.2 cm to 19.1 cm, which represented “stable disease” according to the Response Evaluation Criteria in the Solid Tumors (RECIST) manual (14).
Patient 2
A 60-year-old woman with right-sided advanced breast cancer without any previous treatment had pain, ulcer, bleeding with severe anemia (hemoglobin 4.4 g/dl), and right-arm edema. Pretreatment CT revealed a huge tumor spreading from the right breast to the right axilla with multiple metastatic nodules beyond the medial line to the left chest wall (Fig. 2a and b). Left axillary lymph node metastasis was also observed. CT angiography showed no evidence of supply from the inferior epigastric arteries. Therefore, RESAIC of the right side and conventional selective arterial infusion chemotherapy of the left side were attempted.
(a, b) Pretreatment CT images of patient 2 show a very large tumor spreading from the right breast to the right axillary region, with multiple nodules in the left chest wall. (c, d) CT images obtained at 6 weeks after right-side RESAIC revealed a decrease in the size of the tumor in the right chest wall (c) and an increase in the size of the tumor located medially (d). (e) CT images taken 6 weeks after the bilateral RESAIC demonstrated decrease in tumor size as partial response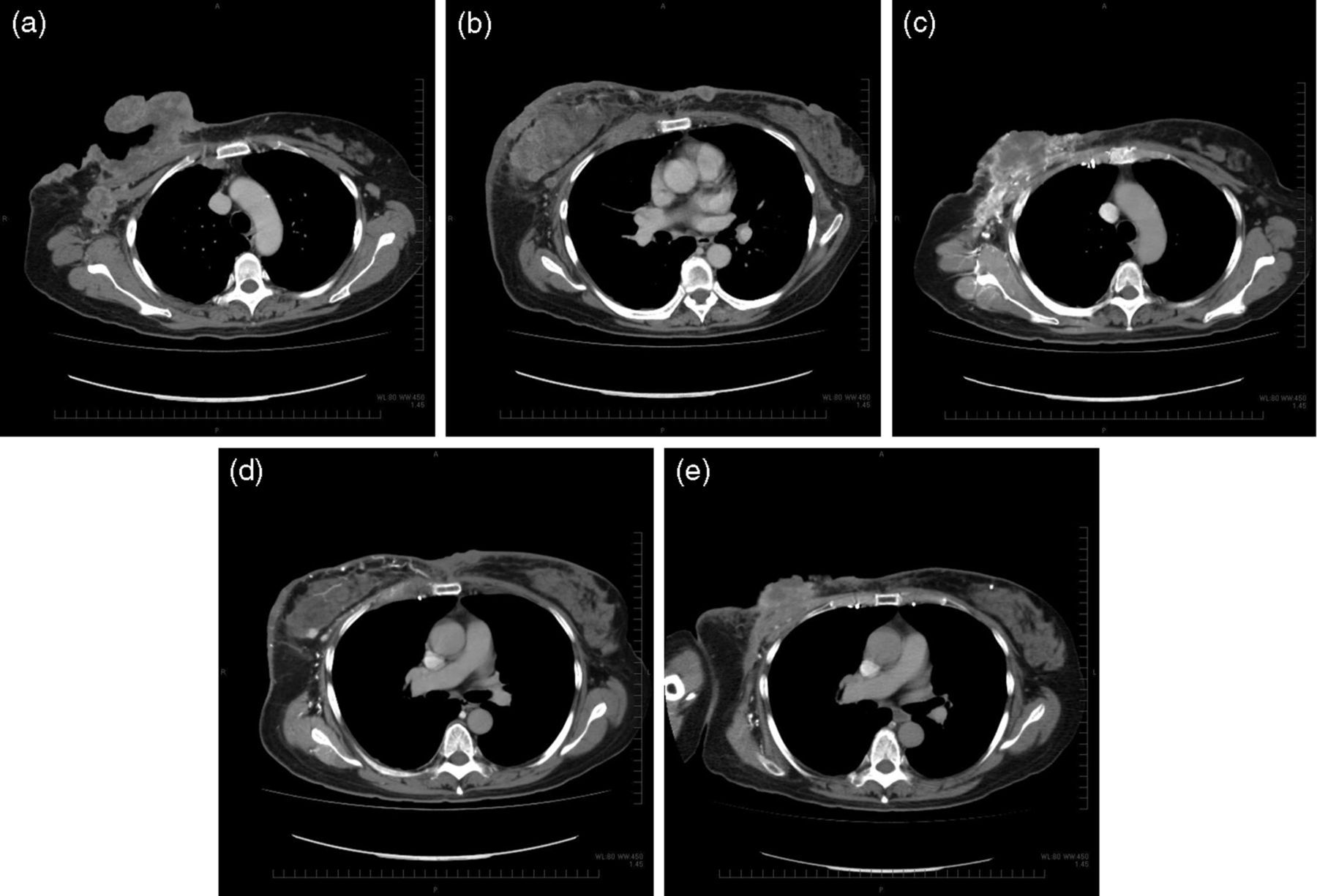
The procedure was performed under local anesthesia via the right brachial artery approach. A right internal thoracic arteriogram revealed the presence of a very large tumor in the chest wall. Thus, the right internal thoracic artery was embolized by a mixture of NBCA-LPD for the arterial redistribution. Additional embolization with microcoils was also performed. The CPS was implanted in a manner similar to that used for Patient 1. At the same time, the selective arterial infusion of EPIR 40 mg from the left internal thoracic artery was performed after a confirmatory arteriogram was obtained.
The regimen was as follows. EPIR 30 mg/body was injected at the first treatment. Subsequently, the treatment cycle consisted of CDDP 10 mg/body and 5-FU 1000 mg/body on days 1, 8, and 15 and EPIR 20 mg/body on day 22. The CT angiography from the right CPS obtained at 6 weeks after the treatment revealed a decrease in the size of the main tumor of the right breast and an increase in the size of the nodules of the medial and left chest wall without enhancement, which suggested effective drug distribution (Fig. 2c and d). The contralateral axillary lymph nodes had also increased in size. Then, we decided to perform the left RESAIC. The CPS was implanted after embolization of the left internal thoracic artery with NBCA-LPD.
The regimen for the bilateral RESAIC was as follows. EPIR 40 mg/body was injected at the first treatment. Subsequently, the treatment cycle consisted of CDDP 10 mg/body and 5-FU 1000 mg/body on days 1, 8, and 15 and EPIR 30 mg/body on day 22.
The patient also experienced an improvement in symptoms without significant procedure-related complications. At 3 months after treatment had started, tumor size had decreased from 25.8 cm to 11.8 cm, which represented “partial response” to the RECIST (Figure 2e).
Discussion
Although the RESAIC method seems to be useful for local control or palliation for locally or recurrent advanced breast cancers, favorable drug distribution is essential for treatment success. The arteries feeding the tumor are typically the internal thoracic artery, the lateral thoracic artery and the intercostal artery. Anastomoses through the penetrating branches are especially apparent in the case of a large advanced breast tumor. In addition, the artery feeding the recurrent breast cancer tends to be more complex due to vascular damage from the previous treatment.
In patient 1, the right internal thoracic artery and the left inferior epigastric artery fed the recurrent tumor in the left breast. At the same time, the right internal thoracic artery displayed an irregularity. Previous treatments such as radiation therapy and arterial infusion chemotherapy may have damaged the artery and promoted this communication. In patient 2, spread of the lesion to the contralateral side necessitated the use of a bilateral approach.
To obtain sufficient drug distribution, the artery feeding the tumor should be assessed adequately by CT angiography in all cases. The history of treatment is also of importance. In addition, the CT obtained by the infusion of contrast material via a catheter-port system during the treatment is helpful in understanding the pattern of drug distribution. Spread of the lesion to the contralateral side represents an indication for bilateral RESAIC.
An additional point to consider when attempting RESAIC is the potential for cerebral infarction in the area surrounding the vertebral arteries. Other potential complications are related to CPS issues such as occlusion, detachment and infection. The limitations of bilateral RESAIC include occlusion of the axillary artery due to tumor invasion or any vascular lesion.
In conclusion, bilateral RESAIC may be useful when advanced breast cancer spreads to the contralateral chest wall. Physicians must consider the area of the redistribution and the site of indwelling in each case to achieve sufficient drug distribution, which may provide a greater likelihood of local control or palliation for the patients with locally or recurrent advanced breast tumors who have abandoned standard therapeutic approaches.