
Abstract
In recent decades, advances in nanotechnology engineering have given rise to the rapid development of many novel applications in the biomedical field. However, studies into the health and safety of these nanomaterials are still lacking. The main concerns are the adverse effects to health caused by acute or chronic exposure to nanoparticles (NPs), especially in the workplace environment. The lung is one of the main routes of entry for NPs into the body and, hence, a likely site for accumulation of NPs. Once NPs enter the interstitial air spaces and are quickly taken up by alveolar cells, they are likely to induce toxic effects. In this review, we highlight the different aspects of lung toxicity resulting from NP exposure, such as generation of oxidative stress, DNA damage and inflammation leading to fibrosis and pneumoconiosis, and the underlying mechanisms causing pulmonary toxicity.
Introduction
The study of nanotechnology has emerged in the last few decades due to advances in the field of engineering, which have facilitated rapid and mass production of engineered nanomaterials. These particles, defined as having at least one dimension in the nanoscale, are so small that they can easily enter or diffuse through pores of membranes. They also possess characteristics much different from their bulk counterparts. Nanomaterials form the foundation for the development of ground-breaking nanomedical devices applied in drug delivery and biomarker discovery, as well as in molecular diagnostics. 1 Even now, various nanomaterials are increasingly incorporated into many consumer items, such as clothing and plastic wares, 1,2 thus increasing the risk of human contact and exposure to nanomaterials, not just in the industrial work places, but also in the home environment.
The future prospects for nanotechnology are bright and promising. While the attention of current researchers has been toward enhancing the applications of this novel technology, comparatively less research has been performed to assess the potential deleterious health effects of these unique materials. The sheer diversity of size, shape, structure and elemental constituents, including surface modifications of engineered nanoparticles (NPs), makes their evaluation tedious and challenging. Adding to the confusion, older literature would use the term ultrafine particles (UFPs) to define both engineered NPs as well as ‘unintentionally generated NP’, including combustion-derived products such as carbon black. With such a blanket term used, it would give misleading reports if toxicity were to be due to engineered NPs where properties are better established than the accidental NPs generated (of which components are an unknown mixture).
There are three main routes of entry of the NPs into the human body. First, NPs are inhaled into the body from atmospheric air via the upper respiratory tract. Exposure to metal NPs like iron, nickel and titanium oxide NPs (TiO2NPs), as well as the carbon-based NPs in the work place environment has become a common event. 3,4 Oral ingestion and entry via the dermal route, either by injection into the dermal layer or absorption through the pores of the skin, are mainly mediated by exposure from therapeutic or cosmetic applications. 5 We have opted to focus on the respiratory route, which is the most important consideration for study of atmospheric exposure to NPs. The lungs would be the first line of contact for particles that gained entry into the body and hence the most likely organ for accumulation and long-term exposure. In one inhalation study, the lung showed the highest bioavailability of gold nanoparticles (AuNPs) within five days of NP exposure and significant accumulation over 15 days exposure. 6 The data from another report also highlighted that aggregates of silver NPs (AgNPs) could be retained in the lung for seven days, while the non-aggregated ones can easily translocate to other organs. 7 These studies remain even more important as more NPs are increasingly being manufactured, leading to increased occupational exposure and release into the atmospheric environment. 8
In this review, we will examine the issue of lung injury and diseases induced by nanotoxicity, with a distinct focus on metal-based engineered NPs. At times, we will refer to early studies on UFP pollutants because they are the foundation for much of the present research into the pulmonary toxicity of NPs. As the field continues to develop and mature, it may not be long before safety evaluation of engineered NPs becomes a prerequisite before use in biomedical applications. 9–11
Intrinsic toxicity of NPs
It has been known for some time that NPs are not innocuous but may harbor harmful effects. The ‘NP hypothesis’ first originated from information available on particulate matter (PM), especially work on PM with less than 10 μm diameter (PM10), which formed the basis for extensive studies into nanotoxicology. 12 The hypothesis suggests that NPs are the main drivers of proinflammatory effects in cases of PM toxicity because they are the main particulate type found in PM mixtures, thus implying that NPs may possess some intrinsic toxicity. What are the properties of NPs that would give rise to toxic effects? One would be the small size of NPs as it would give rise to a high surface area per unit mass, and from what we know about particle toxicology, this is often correlated with higher reactivity. 12 In addition, the larger surface area also leads to an increased possibility for the formation of free radicals (i.e. superoxide anions or hydroxyl radicals), which consequently drive oxidative stress, especially for metal-based NPs. Thus, this forms the underlying mechanism responsible for inflammatory responses to NP exposure. 13 Certain NPs such as heavy metal cadmium quantum dots and AgNPs are also known to induce oxidative stress and are highly toxic. 14,15 However, not all cases of oxidative stressed are caused by direct effects of NPs. Metal contaminants on the cell surface have also been shown to be the main causative agents that generate free radicals. 16 While size does play a big part in particle toxicity, the shape of the NP as well as the surface modifications may also affect their uptake and toxic potential. 17,18
Another effect of the large surface area per unit mass of the NP is that it may be responsible for the adsorption of various organic compounds from ambient air and this phenomenon enhances biological interactions within the organism. 19 It has been shown by a number of epidemiological studies that airborne PM from combustion sources like motor vehicles or industrial exhausts contributes to respiratory and cardiovascular morbidity and mortality. 20–22 A specific toxicological role has been observed for particles with diameter <0.1 μm (UFPs in particular), which are generated in incomplete fuel combustion. UFPs have been found to induce inflammatory and prothrombotic responses, promote atherosclerosis, thrombogenesis and may be the cause of other cardiovascular events. 23 Besides affecting lung physiology, these particulates have also been shown to affect the autonomic nervous system or, in other cases, act directly on cells in various organs and may possess mutagenic potential. 24,25
The lung as a route of entry
The human lung is a vulnerable organ for NP invasion as there is approximately 2300 km of airways and 300 million alveoli, giving rise to a large surface area, which is in contact with the environmental atmosphere and the ultrafine particulate pollutants present in it. 2 Even though nasal cilia and mechanical actions, such as coughing, could trap and expel larger size particles from the airways, they may not be so effective in getting rid of NPs. The small size of NPs allows them to easily penetrate into the deep air spaces of the alveoli (Figure 1) and be readily taken up by lung epithelial cells and fibroblasts (Figure 2).
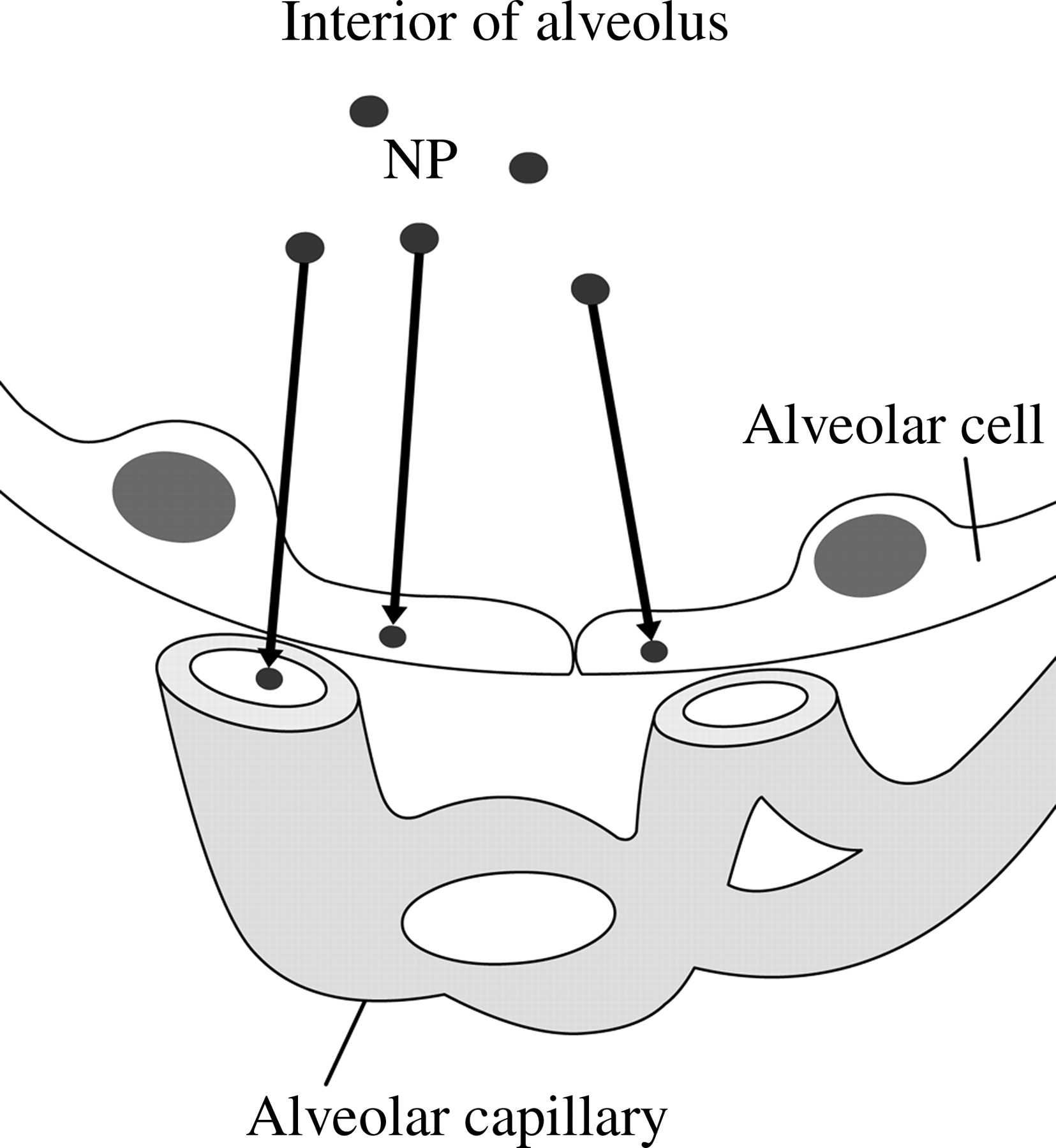
Entry of NPs into alveolar cells and the pulmonary circulation. NP, nanoparticle
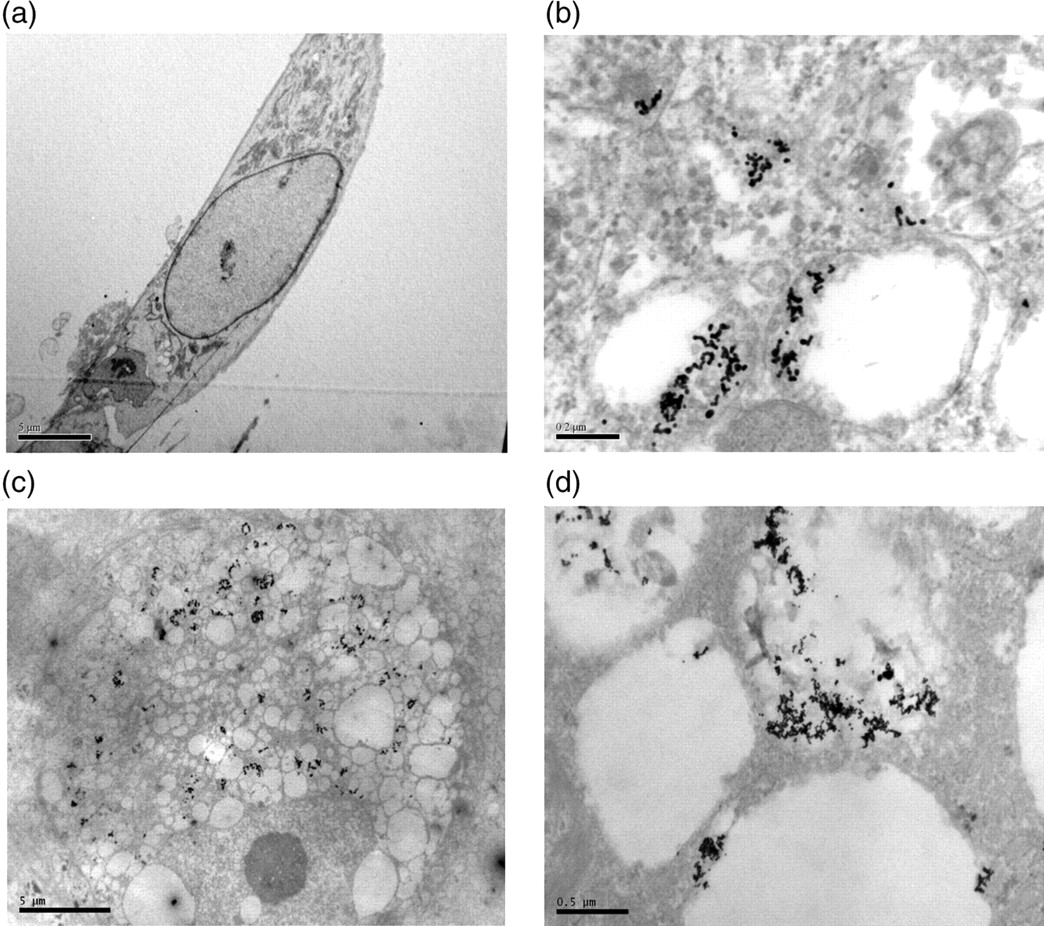
TEM of MRC-5 human lung fibroblast and primary human SAECs treated with AuNPs. MRC lung fibroblasts and SAECs were routinely cultured in four-chambered coverglass (Lab-tek Chambered Coverglass System, Nalge Nunc International, Rochester, NY, USA) at a density of 7000 cells/well and exposed to 1 nmol/L AuNPs (20 nm in diameter) for 72 h. Post-treatment, cells were fixed in 3% glutaldehyde, osmicated with 1% osmium tetroxide, dehydrated and embedded in araldite. Ultrathin sections were cut and viewed in an Olympus EM208S TEM after double staining with uranyl acetate and lead citrate. (a) Low magnification image of an MRC-5 fibroblast. Scale bar = 5 μm. (b) Higher magnification with arrows pointing to AuNP clusters in cellular vacuoles present in the cytoplasm of the fibroblasts. Scale bar = 0.2 μm. (c) Low magnification image of an SAEC. Scale bar = 5 μm. (d) AuNP clusters are also similarly deposited in the vacuoles present in the cytoplasm of the SAEC. Scale bar = 0.5 μm. TEM, transmission electron microscopy; SAEC, small airways epithelial cell; AuNP, gold nanoparticle
There is only a single-cell layer that separates inhaled air from the blood capillaries, which makes for a poor barrier against the entry of NPs from the alveolar lumen into the blood circulation (Figure 1). UFPs from combustion engines are not taken up by macrophages in the lungs and instead translocate to other organs beyond the lungs as evidenced by controlled clinical and animal studies. 4,26 NPs have been reported to cross the alveolar–capillary barrier (with the aid of caveolae) into the circulatory system. 27 Some research groups have found that AuNPs and carbon-based NPs could potentially overcome the blood–brain barrier and translocate to the brain by the uptake of these NPs through the olfactory bulb. 6,28 Because much of the concern regarding exposure to NP toxicity in the workplace comes from either accidental or indirect release of NP as aerosols into the atmosphere during the manufacturing process, the respiratory system invariably becomes the first line of contact and main route of entry of atmospheric NPs into the body.
Translocation and deposition of NPs in the body
Once the respiratory system is exposed to UFPs, translocation to other organs is rapid and the particles may appear in the liver, heart and nervous system in a matter of hours. 28–30 The main mechanisms of NP deposition in the lungs are impaction (PM >100 μm), sedimentation (particles in the range of 0.1 and 50 μm) and diffusion (UFPs). 31 Whether UFPs accumulate in the nasal cavity, conducting airways, and the alveoli by diffusional displacement are dependent on the size of the particles. Larger particles (with diameter greater than 1 μm) deposited on the epithelial surface may, however, be cleared by bodily responses, such as coughing, or by mucociliary transport, and/or phagocytosis by alveolar macrophages. 32–34 Conversely, UFPs seem to penetrate cellular membranes rapidly. 28,33,34 Besides, there have been in vitro studies showing that UFPs induce oxidative stress and mitochondrial damage via penetration into the epithelial cells, and that UFPs are more potent than PM2.5 and PM10. 35
The lung is not just an entry point for NPs, but as a result of the close connection with the circulatory system, NPs in the lungs have the potential to translocate to other organs quite readily. Exposure of rats to AuNPs showed that inhaled NPs accumulate significantly in the lungs and are detected in other organs a few weeks later. 6 In another in vivo study, AuNPs injected intravenously into rats were found to accumulate in the liver and kidneys up to one month postinjection, implying that these organs may be reservoirs for NP deposition and that there could be an inhibition of natural excretion of NP from the body. 36 Therefore, it would seem that the smaller the size of the NPs, the wider will be the biodistribution in the body, and the longer the biopersistence (which reduces clearance from the body), the greater will be the impact on toxicity in cells, tissues and organ systems. To understand the effect of NPs in the lung, we will next consider the mechanisms associated with NP toxicity at the cellular level.
Underlying cellular mechanisms of NP-induced toxicity
Ineffective clearance of NPs
The epithelial cells in the respiratory tract are covered and protected by a thin liquid layer called the epithelial lining fluid, which is composed of various neutralizing agents. 37 The main component is surfactant whose main function is to displace PM <6 μm in order to facilitate mucociliary clearance. 34 Proteins in the surfactant play a role in opsonization as well as in the clearance of PM by macrophages. 37 Furthermore, UFPs are physically aggregated into agglomerates, thus making them easy targets of phagocytosis by the macrophages, in particular the alveolar macrophages, on the epithelial surfaces of the alveoli. 33,34 Their primary role is to engulf and process particles that are not cleared by mucociliary action and coughing. 38,39 However, depending on the level of agglomeration of NPs, macrophages may not be efficient in clearing them, resulting in granulomatous lesions. 35 Also, when alveolar macrophages are activated following PM phagocytosis, substantial amounts of oxygen radicals, proteolytic enzymes, proinflammatory mediators and growth-regulating proteins are released, which may lead to both acute and chronic lung inflammation. 40,41 These mediators may also stimulate epithelial and endothelial cells and promote leukocyte recruitment into the lungs. 42 Furthermore, studies have elicited that lung epithelial cells, when exposed to PM, produce a spectrum of proinflammatory mediators that attract leukocytes and upregulate adhesion molecules on their cell surface so as to recruit leukocytes into the air spaces. 43–46
Surface functionalization on NPs is also another factor that affects uptake, penetration and clearance. While there is no unique functionalization that is specific for lung epithelium, it is possible to develop specific targets for one cell type, for example, nanodrugs that target cancer cells. 47,48 Just as size of the NPs determines the depth of penetration into lungs, surface modifications can also affect cellular targeting of NPs. This brings us to the question as to how ‘sticky’ are NPs to their target sites and their rate of clearance from the body. However, few research studies have attempted to address this issue. A study by Kim et al. 49 showed that AgNPs preferentially accumulate in the liver and kidneys. NP accumulation in the kidneys is gender specific, with a two-fold higher amount of AuNPs accumulating in female than in male mice. Choi et al. 50 have observed that quantum dots less than 5 nm in size could be completely excreted from the kidneys.
Oxidative stress
Exposure to NPs and PMs are known to cause an increase in reactive oxygen species (ROS), which could lead to oxidative stress. ROS generation by NPs could be due to three factors as outlined by Knaapen et al.: 51 (i) active redox cycling on the surface of NPs, particularly the metal-based NPs; 52,53 (ii) oxidative groups functionalized on NPs; and (iii) particle–cell interactions, especially in the lungs where there is a rich pool of ROS producers like the inflammatory phagocytes, neutrophils and macrophages. Overproduction of ROS activates a series of cytokine cascades, which include an upregulation of interleukins (IL), kinases and tumor necrosis factor (TNF-α) proinflammatory signaling processes as a counter reaction to oxidative stress 45 (Figure 3). Studies on TiO2NPs and C60 fullerenes have shown that these NPs induce elevation of proinflammatory enzymes, such as IL-1, TNF-α, IL-6, macrophage inhibitory protein and monocyte chemotactic protein in rodent lungs. 54,55 When receptor tyrosine kinases, mitogen-activated protein kinases and transcriptional factors, such as nuclear factor-κB and signal transducer and activator of transcription 1, are activated, the genes involved in inflammation and fibrosis are transcribed and expressed. 56,57 Stimulation of IL-1β and TNF-α heightens the expression of profibrotic proteins. More specifically, the latter is known to upregulate the production of transforming growth factor (TGF)-β1, which potentiates collagen deposition by fibroblasts, 58 while the former is associated with the expression of platelet-derived growth factor (PDGF)-AA and its receptor, PDGF receptor-α, which increases proliferation of myofibroblasts, promoting the formation of immature collagenous tissue within the lung. 57
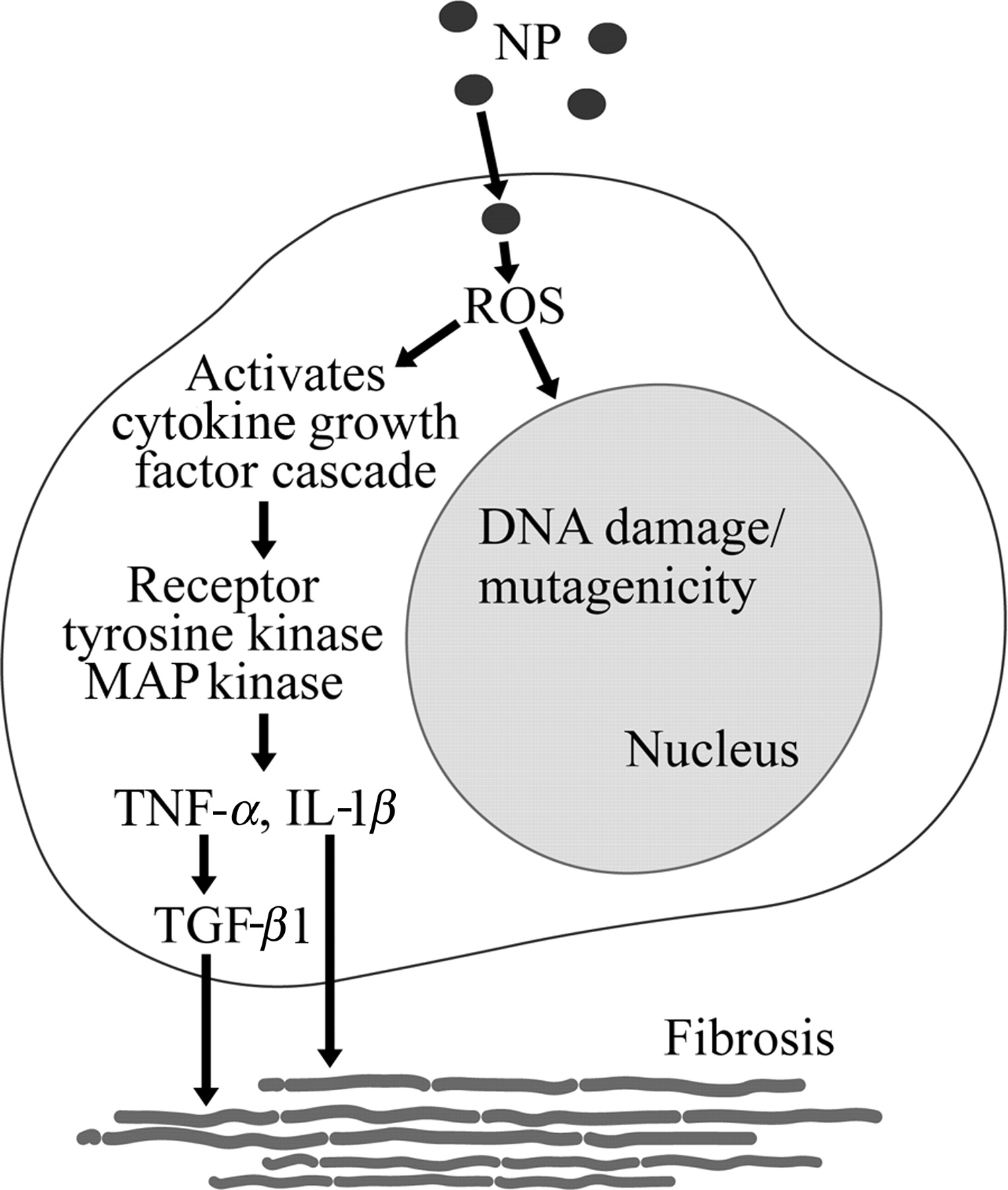
Possible mechanistic pathway for pulmonary toxicity induced by exposure to NPs. Exposure to NPs may lead to oxidative stress due to increased production of ROS and downstream signaling responses that promote fibrosis and produce genotoxicity. NP, nanoparticle; ROS, reactive oxygen species
Genotoxicity
NanoGenotoxicology is yet another new term that was coined to represent the growing trend of research into NP-induced genotoxicity and carcinogenesis (an excellent review on the genotoxicity of nanomaterials is given by Singh et al. 59 ). Although there are still no conclusive links with NP-induced genotoxicity and lung cancer from past epidemiological studies and in vivo rodent experiments, some researchers have pointed out that long-term inflammation and oxidative stress present in tissue environment eventually induces DNA damage in cells and tissues. 59 This is of particular concern, especially if the NPs continue to generate an oxidative environment in the cell that causes gene mutations/deletions. This can lead to larger-scale mutagenesis (Figure 3) and carcinogenicity, and subsequently development of tumors and cancer. 51 Already, more evidence has emerged regarding the DNA damaging properties of certain classes of NPs, particularly the metal-based NPs like AgNPs, AuNPs and TiO2NPs. 60–63 One proposed mode of action for NP genotoxicity is the ability of signaling peptides functionalized on NPs such as carbon nanotubes (CNTs) that enable them to enter the nucleus via nuclear pores. 64 It is yet to be shown that such CNTs are able to cause genotoxicity, but it is believed that there is a greater potential of damage when NPs are able to get in close proximity to DNA. There are also other different mechanisms that may be specific to the elemental composition and shape of NPs, which could lead to DNA damage such as single-strand breaks, double-strand breaks, DNA deletions and genomic instability in the form of increase in 8-hydroxy-2′-deoxyguanosine levels. 65,66 While some researchers have found that exposure to TiO2NPs in rats could cause formation of lung granulomas, 54 others have cautioned that appearance of granulomas does not necessarily mean that the tissue is cancerous as most tissues probably remain benign. 67 As most reports regarding NP toxicity were observed from experiments involving ultraviolet or irradiation exposure, the clinical relevance of these mechanistic experiments are questioned. 68 Nevertheless, a recent study has shown that TiO2NPs may be able to switch on regressive cancer cells. In vivo preimplantation of TiO2NP, followed by co-culturing of a regressive cancer cell line over the implantation site, was observed to induce tumorigenic characteristics such as an upregulation of TGF-β and prostaglandin E2. 69 According to Mroz et al. 70 cells with long-term exposure to NPs, like nanoparticulates in PM10, displayed genome instability under comet assay analysis, altered cell cycle kinetics in flow cytometry and induced protein expression of p53 and DNA repair-related proteins, similar to that observed in irradiated cells. Hence, they postulate that these NPs could activate signaling pathways similar to ionizing radiation, resulting in carcinogenesis as a consequence of errors in DNA replication. DNA repair in ionizing radiation requires activation of ataxia telangiectasia mutated protein, which is a serine/threonine-specific kinase, and subsequently, the ubiquitylation signaling cascade and sumoylation pathway. A postulated mechanism for the repair of damaged DNA from exposure to NPs based on the ionizing radiation model is shown in Figure 4. However, as cancer is a multifactorial disease, there may not be only one defining cause for an individual to develop neoplasm. Instead, it may be more pertinent to place the risk factor from NP exposure alongside other risk factors for cancer as well.
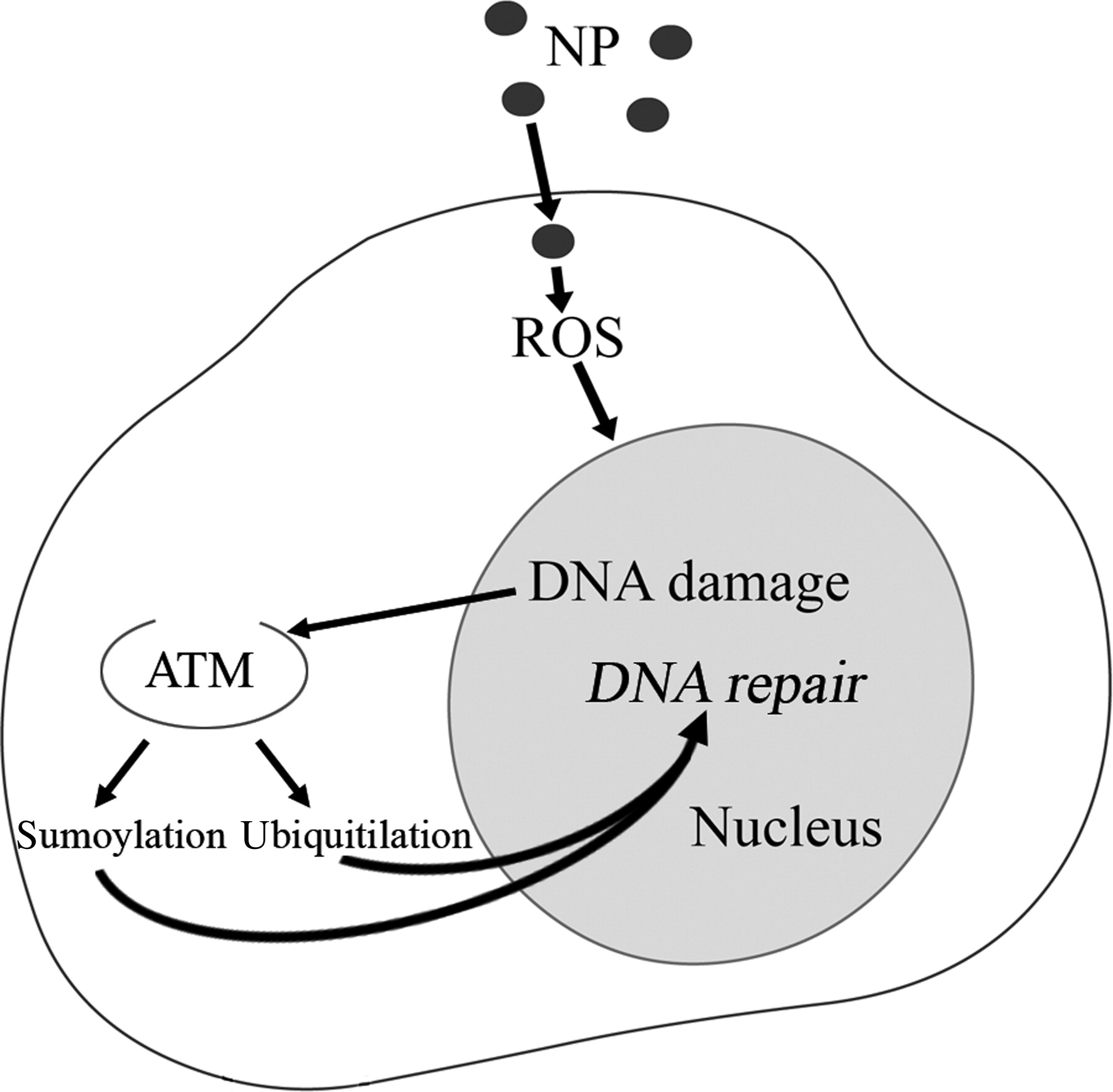
Postulated mechanism for the repair of damaged DNA on exposure to NP based on the ionizing radiation model. NP, nanoparticle; ATM, ataxia telangiectasia mutated
Inflammation of lung tissues induced by NPs
Among all the adverse effects caused by NPs, inflammation (a biological reaction of tissues to harmful stimuli) appears to be the most common factor. In fact, different types of NPs can induce diverse inflammatory responses in the lung. For instance, the toxicity of single-wall CNTs in inducing epithelioid granulomas and interstitial inflammation in mice lungs seven and 90 days after intratracheal instillation has been reported to be higher as compared with other NPs, like carbon black and quartz particles. 71 Oxidative stress is most likely the major underlying mechanism driving inflammation responses by NPs, which lead to the activation of different transcription factors with subsequent enhanced synthesis of proinflammatory proteins. TiO2NPs are able to induce pulmonary neutrophilia mediated via increased production of neutrophil-attracting chemokines CXCL1, TNF-α and IL-8, 72,73 together with a surge in counts of eosinophils and lymphocytes in the bronchoalveolar lavage fluid. 74 CNTs and NPs are also believed to cause adverse effects through inflammation and induction of proinflammatory molecules. 75 However, it must be noted that some researchers have found metal contaminants (such as iron and nickel) in the nanotube production process to be the main causative agent of oxidative stress. 16,76 Pulmonary inflammation may also result in changes in membrane permeability, which in turn can result in particle distribution extending beyond the lung and indirectly affecting cardiovascular performance. 24,77 Moreover, NPs have the potential to enter the brain 28 and blood circulation, 78 and subsequently other major organs, inciting inflammation in these places. Needless to say, inflammation arising as a result of NP exposure could lead to pulmonary diseases or exacerbation of existing lung disorders.
Lung disorders that may arise from NP exposure
Pulmonary fibrosis
Pulmonary fibrosis occurs as a result of increased tissue reactivity leading to the formation and accumulation of fibrous connective tissue. Fibrosis can take many forms, varying from severe forms that cause distortion of lung architecture, inducing bronchiectasis and chronic respiratory infection, to milder forms, which comprise of restrictive ventilatory defects causing hypoxemia, cor pulmonale and pulmonary hypertension. 79,80 The first step in pulmonary fibrosis is inflammatory response when immune cells comprising macrophages and neutrophils are excessively activated. These immune cells release toxic mediators, which result in the loss of epithelial integrity and promotion of tissue injury. When this happens, the cell normally employs a repair mechanism wherein mesenchymal cells are activated. These mesenchymal cells have a three-fold role, which includes extracellular matrix deposition, re-epithelialization and restoration of normal lung architecture. However, certain patients show an abnormality in tissue remodeling and excessive matrix deposition, which leads to progressive scarring and fibrosis. 80 Recently, some researchers have also observed the presence of multiwalled CNTs (MWCNTs) in the subpleural region in lungs of mice giving rise to fibrosis and scarring. 81 This has become a matter of grave concern as non-clearance and persistence of MWCNTs could cause inflammation in the sensitive mesothelium, leading to mesothelioma formation. Another study also suggests that pulmonary fibrosis induced by MWCNTs may be exacerbated in people with existing lung inflammation. 82 As aptly put by Byrne and Baugh, 13 the irregularity in tissue remodeling and fibrosis, with reference to particle inhalation, may be due to an exaggerated inflammatory response that is driven by inability to clear toxic particles from the lungs via the usual protective mechanisms. This whole cascade may be initiated by interactions of alveolar macrophages with lung epithelial cells, or even directly by interstitial fibroblasts. 13
The extent of fibrotic response may also determine the severity of loss of tissue function. Generally fibrosis occurs in the following sequence: 83 (a) organization of the immature fibrinous tissue with the formation of new blood vessels and increased blood supply; (b) proliferation of myofibroblasts; (c) increased deposition of extracellular matrix; and finally (d) scar formation. Under conditions of normal lung function, immature intralumenal collagenous tissue may be eliminated by the fibrinolytic system with concomitant apoptosis of myofibroblasts, thus favoring re-epithelialization. 84 Depending on the degree of injury to the alveoli, removing the continual exposure to NPs may allow re-epithelialization. In chronic cases of injury, however, lung function may be lost.
Pneumoconiosis
Pneumoconiosis, an occupational lung disease, is clinicopathologically classified into two categories, fibrotic and non-fibrotic. While the fibrotic process involves focal nodular or diffuse fibrosis, non-fibrotic lesions involve particle-laden macrophages, with minimal or no fibrosis. 85 The former comprises silicosis, coal worker's pneumoconiosis, asbestosis and berylliosis, which are caused by sustained inhalation of silica particles, washed coal particles, asbestos fibers and beryllium particles, respectively. 13 Non-fibrotic lesions cover siderosis, stannosis and baritosis that are caused by particles of iron oxide, tin oxide and barium sulfate, respectively. Among these pulmonary lesions, silicosis, coal worker's pneumoconiosis and asbestosis dominate the clinical cases. 85 Over the last three decades, death rates due to asbestosis have increased tremendously, overwhelming the decrease in death rates due to the other two types of pneumoconiosis. 86 Here it is to be noted that these clinical conditions are influenced by a multitude of particle types, varying in size and concentration. These particulate clouds are mineral and combustion-derived, and are found most commonly in developing nations. NPs are the most toxic of the particles found in particulate clouds and are the most significant contributors to fibrogenicity. 87 It is hypothesized that NPs could also behave like asbestos in vivo since some NPs, particularly the carbon rods, have similar shape, size and properties. A study showed evidence of asbestos-like pathogenic behavior of MWCNTs in mice, inducing inflammation and formation of graulomas. 88 Although there have not been any confirmed reported clinical cases of engineered NP-induced pulmonary fibrosis, it should be remembered that the rapidly increasing exposure levels may cause serious issues, considering the extent to which NPs are integrated into technology. 71
Exacerbation of asthma
Asthma is a disease whereby inflammation of the airways induces lung hypersensitivity, and hence asthmatic individuals are more likely to be vulnerable to NP-induced lung toxicity. Many early studies have shown that deposition of fine particles are most enhanced in the lungs of patients with chronic obstructive lung disease, including asthma. 89,90 Since inhaled UFPs have higher deposition efficiency in the pulmonary region, more UFPs are retained in the lung with each breath in comparison with larger particles. 89,91,92 In cases of asthmatic patients, airway obstruction causes air trapping and thus an increase in alveolar volume, causing a net increase in UFP deposition through diffusion, although impairment of alveolar ventilation may prove inhibitory. Since alveolar volume increases during exercise, the deposition in healthy individuals is also higher during exercise than while at rest. However, this increase is not significant in asthmatic patients, perhaps because the increased alveolar volume and airway turbulence is innately present. 93 Dead space ventilation increases the minute respiration of patients with obstructive lung disease. 94 This phenomenon along with hyperinflation, which is seen even in mild cases of asthma, is speculated to increase the diffusional deposition of UFPs in the distal airways and alveoli. The increase in particle number in the lung has been reported to be 74% in asthmatic patients compared with healthy subjects. 93 Therefore, it would appear that greater NP deposition in the lung would exacerbate airway inflammation in susceptible individuals.
Another concern would be how the use of steroids in asthmatic individuals would affect NP lung toxicity. Steroids, such as the various forms of corticosteroids, are used in the treatment of asthma as it helps to control and reduce inflammation in the airways by inhibiting cyclooxygenases and production of superoxides. 95,96 How effective steroids are in counteracting NP toxicity is still not known. Our preliminary study has shown that dexamethasone did not affect the viability of NP-treated lung epithelial cells in vitro (Figure 5). Even so, there are proponents for the novel use of platinum NPs as an antioxidant treatment for pulmonary inflammation. 97 Moreover, fullerenes (C60 NPs) have also been reported to exert anti-inflammatory properties. 98
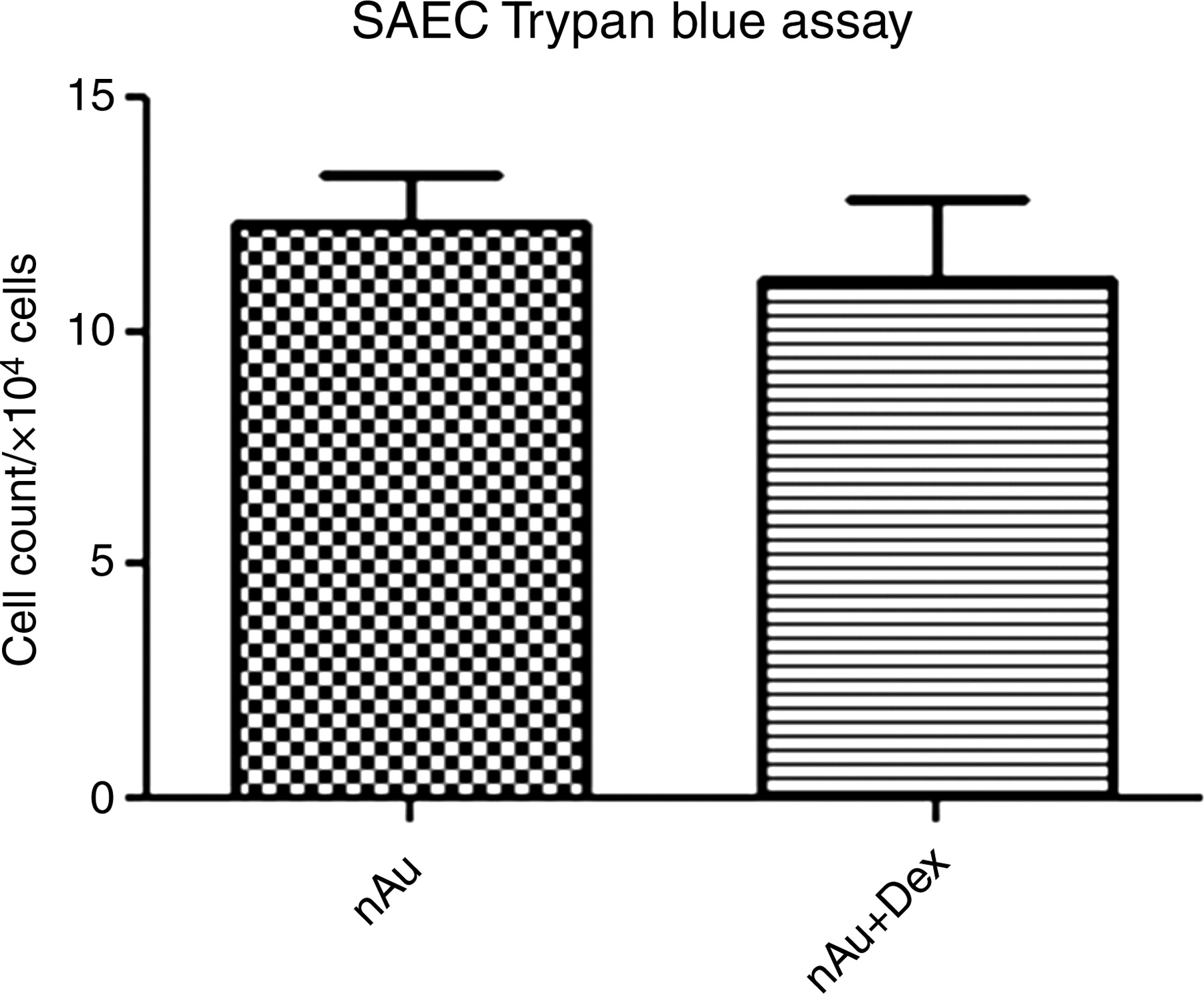
Effect of dexamethasone on AuNP-treated SAECs. SAECs were treated with either 1 nmol/L AuNPs alone or combined with 100 nmol/L dexamethasone for 72 h. Post-treatment, cells were trypsinized, resuspended in culture and cell viability was determined by staining with 0.4% Trypan blue solution (Sigma-Aldrich, St Louis, MO, USA) before counting in a hemocytometer. There was no significant difference in cell viability between the two groups of treated SAECs (P > 0.05). Experiments were carried out in triplicates. SAEC, small airways epithelial cell; AuNP, gold nanoparticle
Conclusion
It is still early days in the study of NP-induced pulmonary toxicity and there is a diversity of factors that need to be taken into consideration before we can truly understand the impact of NP exposure on human health. Even in studies of nanotoxicology, many have called for greater caution in making conclusions about the relevance of any toxicological study on NPs. A recent clinical case study of workers developing pulmonary disease from NP exposure had received criticism from field experts for presumptuous conclusions drawn outside of the study's limitations. 99,100 In the meantime, the cautionary procedure would be to handle the use of engineered NPs with discretion and with appropriate workplace and safety protocols.
Footnotes
ACKNOWLEDGEMENTS
We thank Song-Lin Bay, Chun-Peng Low and Yee-Gek Chan for technical assistance. The work was supported by the Singapore Ministry of Education Academic Research Fund Tier 2 via Grant MOE2008-T2-1-046 and the National University of Singapore (NUS) Environmental Research Institute (NERI) via Grant R706000002646.