
Abstract
In most industries of economy, the production structures evolved into activities characterized by a high division of labour between the business partners combined with specialization, the standardization of service components and extensive networking. In the health-care sector, the first signs of a similar development are beginning to crystallize. As a consequence, networkability, the ability to link up with other players on the basis of commonly agreed standards for the joint provisioning of patient-centred and cost-efficient health services will emerge to a key concept for future health service delivery. As not only technical but mainly organizational and behavioural issues are actually determining networkability of health-care organizations, a holistic model for analysis is needed. In this paper, the main variables leading to an increase in this networkability are identified and compiled into a comprehensible procedure model for health-care practitioners.
Introduction
In the past decade the effects of globalization, differentiation and specialization of markets, and technological advance revolutionized first and foremost highly competitive sectors such as the banking or engineering sector. In order to manage the constant pressure of reducing costs, rising product quality, and shortening process and innovation cycle times, a higher specialization and standardization of service components accompanied by extensive division of labour and networking was achieved. 1–3
At present, the health-care sector has only seen the beginnings of this development. In Switzerland, like in many other industrialized countries, health care is still marked by monolithic structures with a low division of labour 4,5 and annually increasing health expenditure. 6 Reasons for this are manifold. The fact that health care differs in structure from the other sectors is − beside causes such as the ageing population or the lack of economic growth 7 − attributable to the high level of regulation which can hinder or prevent innovation, the high proportion of government investment and the associated low pressure in respect of effectiveness and efficiency, the lack of orientation towards patient benefits and the widely differing interests of the individual players. 8,9 Nevertheless, health-care organizations are nowadays under pressure from patients, insurers, government agencies and other stakeholders to restrict expenditure while improving the quality of health services. More recent developments in the Swiss health-care sector such as the introduction of diagnosis-related groups for inpatient tariffing or fixing rates for primary care treatments are a clear indication that the pressure to achieve effectiveness and efficiency is set to increase significantly. Networkability, in other words the ability to link up with other players in the health-care sector rapidly and with low set-up costs for the joint provisioning of services, will then take on greater importance.
Previous research in the area of health services research, strategic management or information systems often focused on very specific aspects of networkability such as the strategic positioning of organizations in complex value chains, 10,11 the optimization of business processes in networks, 12 cultural and behavioural considerations of networks, 13 or information technology as means for building networking platforms. 14,15
However, the intention of this contribution is to investigate the multitude of the various factors influencing networkability of health-care organizations. Since established knowledge on networkability in health care is scarce, the empirical part of the study, therefore, focuses primarily on determining the variables to be measured. Once the variables have been identified, the next objective is to reduce complexity by using factor analysis in order to obtain a comprehensible model of networkability of the health-care domain. The remaining sections of the study are devoted to the discussion and interpretation of the results. Finally, the main conclusions and an outlook on further research are presented.
Exploration of the actual understanding of networkability in health care
Data and information collection
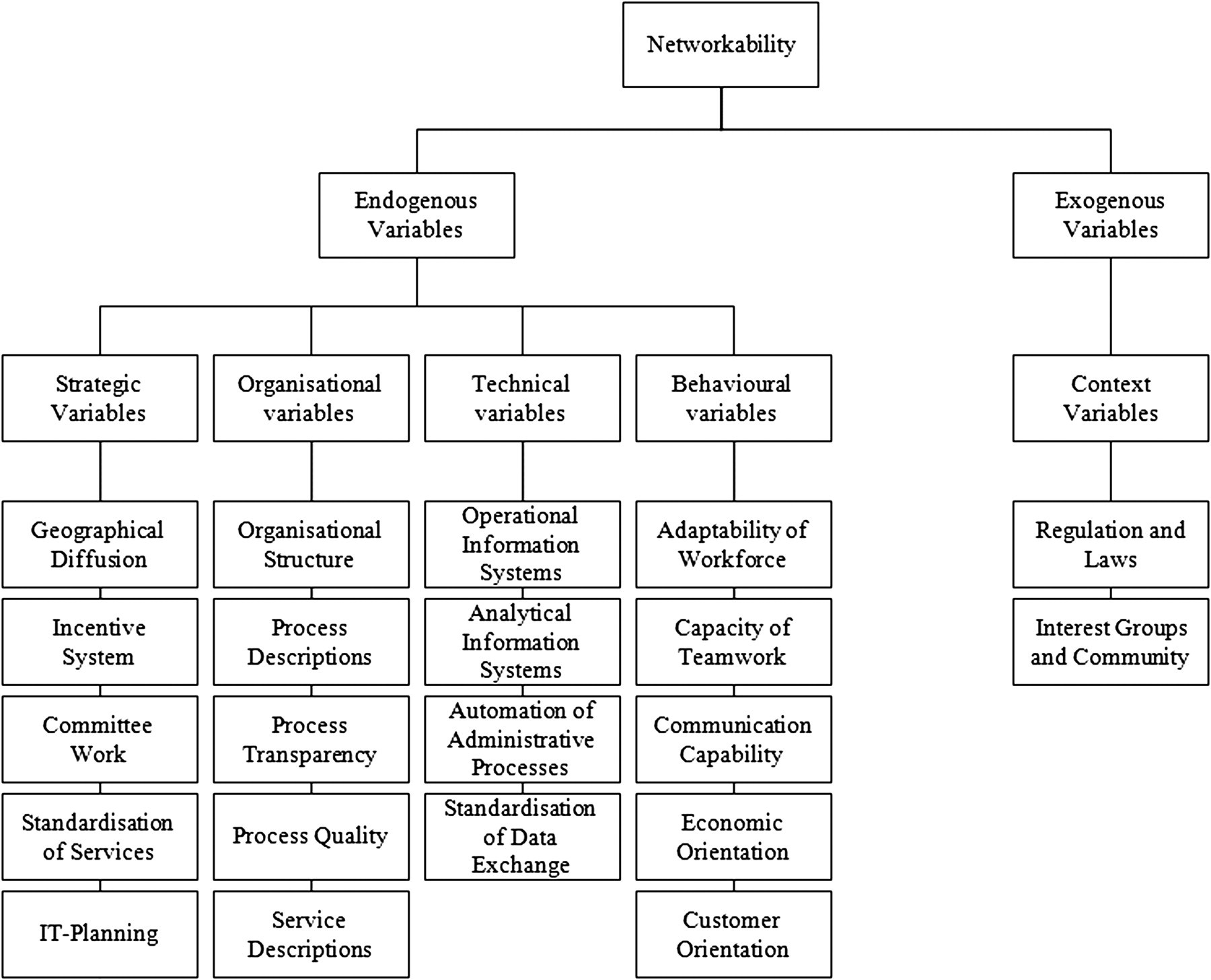
In health care, and in particular in the area of health services research, the use of focus groups is a proven qualitative research method 16–18 for the exploration of people's ‘frameworks of understanding’. 19 As in health care, the perceptions of the various actors are extremely important to the success of any change effort 20 and profound theoretical underpinnings of the concept of networkability are still missing, focus group discussions were used to obtain deeper insights into the topic. In order to get a broad distribution of opinions, three different focus groups, one for medical practitioners, one for health insurance companies and one for service providers with an average of five to 10 exponents per fraction, were set up. In the period from June 2005 to May 2006 a total of 15 sessions – five per focus group – were conducted. The results of the discussions yield to a list with more than 100 potential influencing variables. To facilitate further investigation, the identified variables were clustered first of suggestibility as seen by the exponents (endogenous or exogenous variables) and second in terms of similarity in content (strategic, organizational, technical, behavioural or context variables). Thereby, the number of potential variables was reduced to approximately one-fourth (Figure 1).
Variables influencing networkability of health-care organizations
Survey development and evaluation
A major disadvantage in using focus group discussions lies in the lack of representativeness as a result of the small number of people surveyed. In order to obtain as wide coverage as possible for validation of the identified variables, a survey was conducted across Switzerland during the period from July to September 2006. Beforehand, the draft version of the questionnaire was checked by a number of health-care experts, with a view to removing any inconsistencies and generally improving the structure. In conducting the survey, the following questions were asked:
To what extent have the identified variables an impact on the networkability of your organization? Which variables not listed in the questionnaire have also an influence on the networkability of your organization?
The questionnaire was either distributed by post or by email, addressed individually to 500 key persons of health-care organizations (doctors, hospital managers, health insurance managers, administrative personnel and service provider managers). Of the 500 questionnaires sent out, 65 valid replies were returned, giving a response rate of 13%. Thereof 45% were completed by doctors and hospital managers, 23% by health insurance managers and 12% by employees of a service provider. Another 20% came from other areas (e.g. pharmaceuticals industry, public administration). Sixty-eight percent of the respondents described themselves as working in a management position. The remaining respondents were medical specialists (9%), information science and technology (IT) professionals (11%), people working at the interface between medicine and IT (3%) or stated another function (9%).
The questionnaire contained five main blocks (according to the differentiation between strategic, organizational, technical, behavioural and context variables), and an additional one for the identification of missing influencing variables. To question the identified variables a five-point Likert scale was used, where 0 means that the variable has no influence at all, 1 that the variable is unimportant, 2 that it is moderately important, 3 that it is important and 4 that it is very important. For the final block, where the respondents were asked about the completeness of the study, a free text field was provided.
As shown in Table 1, all identified variables were confirmed by the survey since none of them was rated as insignificant for the networkability of a health-care organization. Analysing the final block, it emerged that the financing and infrastructural elements (among others for identity management and access management) should also be considered as important variables in conjunction with the networkability of the health-care organizations. However, the authors propose to subsume this within the existing variables (e.g. IT planning, automation of administrative processes).
Descriptive statistics of survey variables
SD = standard deviation; IT = information science and technology
Factor model of networkability in the health-care sector
Identification of the main factors of networkability
As the monitoring of a large number of variables, as shown in Table 1, is inept for health-care management practice, a condensation of the data is needed. In order to reduce complexity and to obtain a comprehensible model for practitioners, data were reduced by running a factor analysis. This is a multivariate technique with the primary purpose of finding the underlying structure among the variables by analysing the interrelationships (correlations) and summarizing highly interrelated variables to factors with the least possible loss of information. Thus, a factor is nothing but the linear combination of the original variables observed. To quantify the degree of intercorrelations among the variables and the appropriateness of factor analysis the Kaiser–Meyer–Olkin measure of sampling adequacy is used. This index ranges from 0 to 1, reaching 1 when each variable is perfectly predicted without error by the other variables. Values above 0.5 indicate appropriateness. For the used data-set a measure of 0.814 was calculated.
As shown in Table 2, the factor analysis yielded five main factors that account for almost 66% of the total variance explained by the original variables.
Variance explained
To understand the nature of a particular factor, the correlation between the original variables and the factors has to be analysed more precisely. In order to achieve a simpler and pragmatically more meaningful factor solution, the initial factor matrix was rotated. The resulting factor loadings of all variables on each factor are shown in Table 3.
Rotated factor matrix
IT = information science and technology
Interpretation of the results
Factor 1: corporate performance management
One key for successfully developing the networkability of a health-care organization is corporate performance management, explaining 23% of the total variance of the original variables. As health-care organizations are facing dramatic changes in technology, demographics, labour markets, compensation and benefit structures, and malpractice claims the pressure to evaluate service delivery in order to improve patient outcomes is increasing. 21 According to Jackson and Lapsley 22 nearly all public sector organizations use some kind of performance measurement technique. Notably, key performance indicators are used by 77%, the Balanced Scorecard approach by 23% of health-care organizations. Regardless of which technique is applied by an enterprise, the corporate performance management should always consider both technical aspects (analytical information systems, automation of administrative processes), organizational aspects (process quality, process and service descriptions, process transparency) and strategic aspects (interdisciplinary committee work, incentive system and IT planning).
Factor 2: human resources development
The second factor, labelled human resources development, explains almost 14% of the total variance of the original variables. Although most literature in organizational transformation implicitly follows the assumption that human resources are just another type of input, like financial or physical resources, people working in health-care organizations have to be regarded as strategic actors who can act individually or collectively to modify the governments’ projects, such as trying to impede budget cuts, which they present as a strategy to protect the quality of services, or blocking a more equal deployment of resources, which becomes an obstacle to achieving a more equitable access to care. 23 Therefore, special attention has to be given to behavioural aspects (adaptability, capacity for teamwork, communication capability, economic orientation and customer orientation of workforce) when enhancing networkability.
Factor 3: enterprise application integration
Explaining 10% of the total variance of the original variables, the third factor labelled enterprise application integration (EAI) addresses a pure technical perspective of networkability. Main influencing variables of EAI are operational information systems and the actual level of standardization of data exchange. To date, the integration of heterogeneous information systems is a problematic endeavour for health-care organizations, as it is associated with high operational costs and risks. Thus, compared with the use of EAI in other sectors, its adoption in the health-care sector is rather slow. 24
Factor 4: market and service orientation
Another important factor for networkability represents the market and service orientation of a health-care organization, accounting for almost 10% of the total variance of the original variables. Since markets can be considered as locations where buyers and sellers enter into exchanges of similar products and services, 25 product differentiation and geographical diffusion play a major role to augment market share (and the status position within a network). For systematic analysis of a health-care organization's networkability it is therefore useful to take up both an inside-out perspective (what services can be delivered) and an outside-in perspective (what services are needed). On the one hand, product differentiation is influenced by the level of service standardization, that is how much an organization provides or consumers demand off-the-shelf service. On the other hand, it is influenced by the geographical diffusion of the organization, that is how wide the organization's services are spread. The geographical diffusion on its part is directly influenced by the organizational structure of the organization (number of clinics, departments, etc.) and indirectly by density of population.
Factor 5: compliance and public relations
The last factor, labelled compliance and public relations, explains another 10% of the total variance of the original variables. As the health-care sector, more than other industries, is affected by regulatory settings, compliance must be addressed at any rate when networkability is developed. In addition, as a result of the increasing competition in the health-care market, the importance of public relations will increase and therefore should also be considered.
Recommendations for management practice
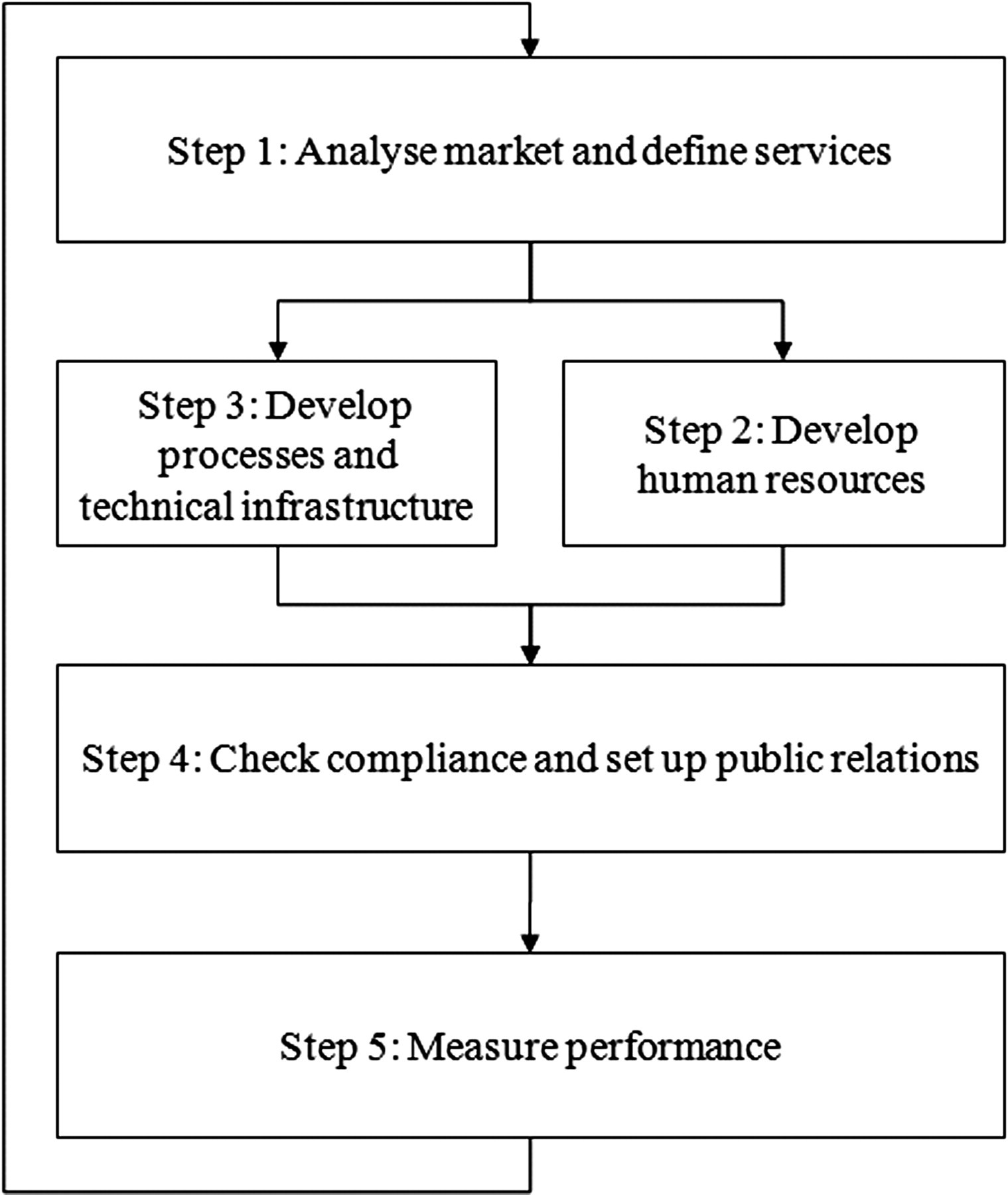
As the intention of this paper is to provide a comprehensible procedure model for health-care practitioners, the developed factor model is consolidated to a step-by-step description of the generic work practices to be effected in order to increase networkability (Figure 2).
Procedure model for enhancing networkability in management practice
Step 1: analyse market and define services
One key for success is a thorough analysis of the market in order to understand evolving opportunities and threats as they relate to the strengths and weaknesses of the health-care organization. Hence, before restructuring health service delivery, the current market size, potential growth rate, profitability, cost structure as well as the key success factors have to be explored. This allows the sophisticated definition of additional health services to be rendered and the identification of those services better are yielded to specialized partners.
Step 2: develop processes and technical infrastructure
When the systematic market analysis is conducted and the portfolio of health services is defined, it is important to examine the processes and infrastructure that support the rendition of the services. This is addressed by an ongoing process known as business/IT alignment. 26 The objective of business/IT alignment is to establish a trusted relationship between the business and IT that allows for an innovation-driven climate in which information and communication technology becomes a strategic enabler for tangible (e.g. reducing process cycle-times and costs of administrative processes) and intangible (e.g. improving quality of care) benefits.
Step 3: develop human resources
However, a holistic improvement of the networkability not only requires the adaptation of processes and infrastructure (‘hard change’) but also to review the corporate culture to become more patient-centric (‘soft change’). As the effectiveness and efficiency of a health-care organization strongly depends on the ability of the human resources, 23 the development of the health workforce is therefore extraordinarily important when networkability is developed. A high degree of flexibility, openness and agility of the workforce is needed. However, this cannot be developed in the short run. Thus, activities and instruments that further the required change have to be planned, implemented and communicated already at an early stage.
Step 4: check compliance and set up public relations
After the successful development of soft and hard change initiatives, it is also crucial to check compliance of its implementation. As an increased networkability is always in the line with a stronger embedding of the network a health-care organization is working with, it is necessary to deliberately define governance policies (e.g. what happens in case of a breach of contract on the part of a networking partner). In addition, it is also increasingly important to better involve the different stakeholders within the own organization. For this, a sophisticated relationship management is needed.
Step 5: measure performance
Finally, the outcome of the implemented changes has to be measured. 27 This is used to evaluate (how well is the health-care organization performing?), control (are the networking partners and the own workforce doing the right things?), motivate (which networking partners should be motivated to do the things right?), budget (on what services should be spend more money?), promote (which stakeholders should be convinced to join?), celebrate (what are the most successful networking partners?), learn (why is service delivery not working?) and improve (what exactly should be done to improve service delivery?). In doing so, an iterative cycle for an ongoing improvement of networkability of health-care organizations is established.
Conclusion and outlook
As modern health systems become more complicated and more people need coordinated care, networkability becomes a crucial concept for the delivery of good quality and affordable health services. In the context of health services research, however, little has been done so far to sharpen the understanding of this particular issue. As existent investigations in other fields of research, like strategic management or information systems, often focus on very specific aspects of their research discipline, only limited conclusions can be drawn for the health-care sector. For this purpose, a total of 21 influencing variables that led to an increase in networkability were identified with the help of focus group discussions and evaluated by means of a survey. In addition, factor analysis was applied to obtain a more meaningful model for health-care practitioners. In turn, the obtained factors provided the basis for a step-by-step description of the work practices for enhancing networkability.
Building on the results presented in this paper, future work should be directed at the practical application of the recommendations to get the basis for further empirical validation. Moreover, additional models and methods for each recommended step have to be identified, adapted or developed in order to provide better guidance for health-care practitioners in day-to-day business.