
Abstract
According to the 2004 US Renal Data System's annual report, the incidence rate of chronic renal failure in Taiwan increased from 120 to 352 per million populations between 1990 and 2003. This incidence rate is the highest in the world. The prevalence rate, which ranks number two in the world (Japan ranks number one), also increased from 384 to 1630 per million populations. Based on 2005 Taiwan national statistics, there were 52,958 end-stage renal disease (ESRD) patients receiving routine dialysis treatment. This number, which comprised less than 0.2% of the total population and consumed $2.6 billion New Taiwan dollars, was more than 6.12% of the total annual spending of national health insurance during 2005. Dialysis expenditures for patients with ESRD rank the highest among all major injuries (traumas) and diseases. This article identifies and discusses the risk factors associated with consumption of medical resources during dialysis. Instead of using reimbursement data to estimate cost, as seen in previous studies, this study uses cost data within organizations and focuses on evaluating and predicting the resource consumption pattern for dialysis patients with different risk factors. Multiple regression analysis was used to identify 23 risk factors for routine dialysis patients. Of these risk factors, six were associated with the increase of dialysis cost: age (i.e. 75 years old and older), liver function disorder, hypertension, bile-duct disorder, cancer and high blood lipids. Patients with liver function disorder incurred much higher costs for injection medication and supplies. Hypertensive patients incurred higher costs for injection medication, supplies and oral medication. Patients with bile-duct disorder incurred a significant difference in check-up costs (i.e. costs were higher for those aged 75 years and older than those who were younger than 30 years of age). Cancer patients also incurred significant differences in cost of medical supplies. Patients with high blood lipids incurred significant differences in cost of oral medication. This study identified the relationship between cost and risk factors of dialysis procedures for ESRD patients based on average variable costs for each dialysis treatment. The results show that certain risk factors (e.g. aged 75 and older, hypertension, bile-duct disease, cancer and high blood lipids) are associated with higher cost. The results from this study could enable health policy makers and the National Health Insurance Bureau to design a fairer and more convincible reimbursement system for dialysis procedures. This study also provides a better understanding of what risk factors play more influential roles in affecting ESRD patients to receive haemodialysis treatment. It will help policy makers and health-care providers in better control or even prevent the disease and manage the distribution of the treatment. In addition, with the results from the analysis of cost information, we can tell which risk factors have more impacts on the dialysis cost. It will further help us control the cost for those high-risk dialysis patients more efficiently.
Background
Chronic kidney disease patients often delay treatment due to the lack of noticeable symptoms associated with renal diseases as well as ignoring these symptoms. This usually results in decline of kidney function, which ultimately leads to end-stage renal disease (ESRD). Patients with ESRD must rely on dialysis for the remainder of their lives, unless they undergo kidney transplantation.
According to the 2004 US Renal Data System's (USRDS) annual report, the incidence rate of chronic renal failure (CRF) in Taiwan increased from 120 to 352 per million populations between 1990 and 2003. This incidence rate is the highest in the world. The prevalence rate, which ranks number two in the world (Japan ranks number one), also increased from 384 to 1630 per million populations. The rapid increase in mortality, prevalence and crude incidence rate of renal diseases places it, along with hypertension and diabetes, as one of the three most important chronic diseases in Taiwan. 1 Because renal disease damages a person's health and quality of life, it poses a great threat to people living in Taiwan.
In 2003, dialysis expenditures reached $2.38 billion, comprising 6.77% of the total annual spending of national health insurance. 2 According to the 2005 national health statistics, there were 52,958 ESRD patients (less than 0.2% of the total population in Taiwan) receiving long-term dialysis. ESRD patients spent more than $500,000 New Taiwan (NT) dollars per year. In 2005, total dialysis expenditures comprised 6.12% of the annual spending of the national health insurance and ranked the highest when compared with all major traumas and diseases. However, in the USA, dialysis costs comprised only 1.12% of total national health expenditures in 2005.
Currently, all dialysis services are reimbursed under the National Health Insurance Bureau's (NHIB) global budget system, a retrospectively floating-point system with an average of NT 0.95 dollars per point. The reimbursement rate for each service will decline by 50% if the frequency of dialysis exceeds 500. This means that providers will need to control the number of dialysis treatments they provide each year because they will be held financially responsible. In other words, as the demand for dialysis rapidly increases, health-care practitioners and health-care organizations will soon struggle to continuously offer quality services under this floating-point global budget reimbursement system. Faced with the challenge of high dialysis expenditures, the NHIB has been actively examining and evaluating the current fee-for-service reimbursement system. It has been suggested that the NHIB should replace the fee-for-service system with capitation, or per-case base reimbursement. 2 In order to alleviate financial threats and possible changes in the reimbursement system, it becomes crucial to identify risk factors associated with resource consumption by dialysis patients. Identification of the risk factors assists providers in their decision to select dialysis patients and provide services. In other words, providers will not have to favour lower risk patients over higher risk patients. The results of this study may lead to a better understanding of the real costs of dialysis service. Additionally, promotion of quality of patient care may result from a fairer and standardized reimbursement system that reflects the levels of severity and actual resources used.
Objectives
On average, dialysis comprises 6–7% of the annual total national health expenditure in Taiwan. In fact, reimbursements for dialysis are the highest when compared with other treatments. Therefore, it is imperative to reduce all costs of dialysis use. Most studies estimate the costs of providing dialysis based on reimbursement data. However, this method fails to capture real costs or resource consumption in providing dialysis services. This study attempts to analyse and predict real resource consumption for dialysis patients with different risk factors, from a real cost perspective within health-care organizations. Results from this study may reveal an association between cost and risk factors of dialysis patients. Furthermore, the results of this study may provide information to the NHIB for planning and implementing a prospective payment or capitation system in the future. Objectives of this study include the following: (1) to identify an association between risk factors of dialysis patients and consumption of medical resources; (2) to suggest a model for setting the reimbursement rate for ESRD patients with different risk levels; and (3) to explore and discuss the differences in types of resource consumption.
Literature review
The physiological functions of the kidney include routine metabolism of water, calcium and phosphate; acid-alkaline ph balance; assisting in red blood cell production; adjusting blood pressure; and hormone secretion. The onset of CRF usually produces no symptoms. However, once the disease progresses to the end stage (i.e. ESRD), kidney function drops to 20% below that of normal people and is usually irreversible. The pathology of ESRD is due to damaged nephrons within the kidney, which results in kidney atrophy and loss of excretory function. The resulting accumulated waste products affect all bodily systems. Diseases that may damage nephrons include vascular diseases, glomerular disorders and obstructive diseases. The common symptoms of ESRD include nausea, vomiting, gastrointestinal disturbances, ‘ammonia’ breath, difficult breathing, chest pain and other cardio-pulmonary symptoms due to fluid accumulation. Skin colour may also be yellow due to urine accumulation or pale due to anaemia. Abnormal metabolism of calcium and phosphate result in skeletal disorders. Dialysis becomes necessary when the glomerular filtration rate is less than 10 mL/minute. Peritoneal dialysis (PD), haemodialysis (HD) and kidney transplantation are the most common recommended treatments for ESRD. However, kidney transplantation is not very popular in Taiwan. Therefore, PD and HD are the major treatment options.
Dialysis involves the use of an ‘artificial kidney’, which is a semipermeable membrane that dialyzes and removes toxins from the blood. In addition, super (ultra) filtration is possible if extra pressure is exerted onto the artificial kidney. Normally, dialysis and ultrafiltration occur simultaneously. 3 Dialysis is usually performed three to four times per week. Each treatment lasts approximately four hours and the dialysis flow speed is 250 mL/minute for HD and 500 mL/minute for PD. An artificial loop for blood circulation is required in order to connect the artificial kidney with blood vessels for dialysis because venous blood flow cannot occur at these high rates. 3 Proper equipment and reagents, as well as frequency and length of dialysis treatment are crucial to the efficiency of dialysis.
The term ‘risk adjustment’ is defined as adjusting medical risk based on a patient's individual variances. The analysis of a patient's risk factors would enable insurance providers to estimate and prepare for a right amount to cover the medical expenses of those with insurance coverage. It is believed that risk factors affect utilization rates and total expenses of medical services. Therefore, using risk factors to properly estimate medical costs may help the NHS lower the revenue difference in insured patients, reduce financial risk for insurers to cover high-risk patients, and prevent insurers and medical providers from denying medical care to patients who are considered vulnerable or at high-risk. 4,5 Lin 6 reported that the current risk-adjusted systems for premium calculation around the world are all based on the Andersen's behavioural model for medical care utilization. 7 Andersen proposed that the demand for health services is a derivative demand from the demand for health itself. His behavioural model for access to medical services is composed of two perspectives: (1) consumption (i.e. when people pursue health); and (2) investment (i.e. when people have better health, they are more productive and have more time to participate in relaxing activities [Figure 1]).
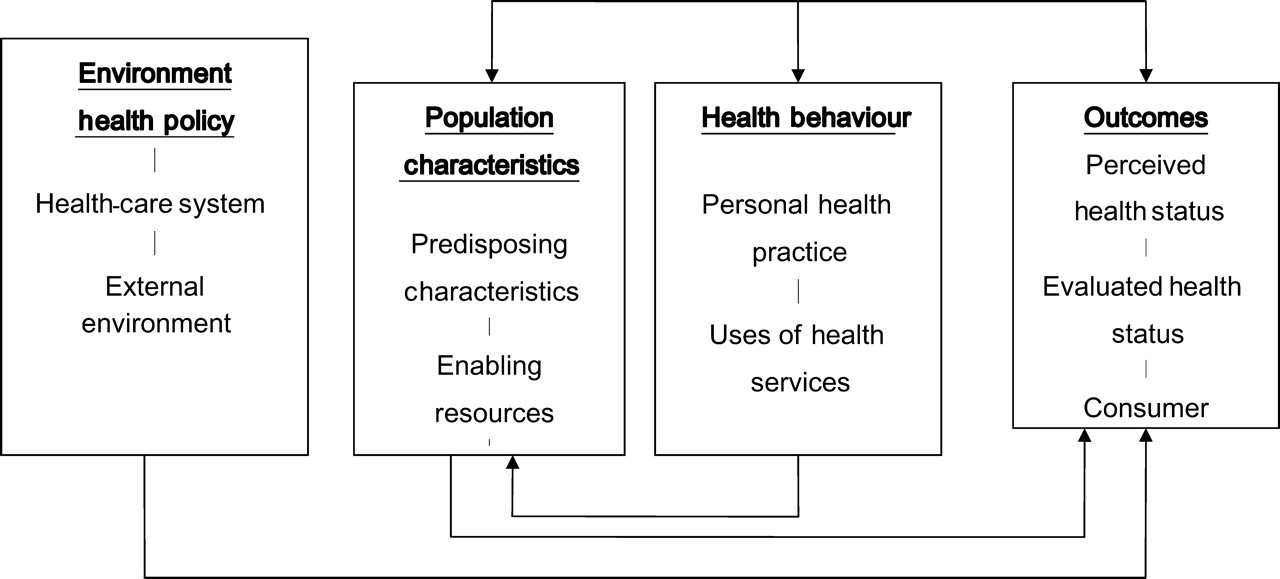
Conceptual model of Andersen's behavioural model and access to medical care (Source: Adopted and modified from Andersen RM. Revisiting the behavioural model and access to medical care: does it matter? J Health Soc Behav 1995;
Three levels of evaluation could be performed in the Andersen model, including structure, process and outcomes. At the structure level, Andersen noted that the combination of utilization pattern, organizational and financing management with predisposing, enabling and need factors, directly and indirectly affects medical service utilization. In addition, personal characteristics (e.g. predisposing factors) may be influenced by environmental factors that reduce exposure to those risk factors in the environment (e.g. physiological, social or economic interaction). The process level implies the interaction between patients and care providers, which includes utilization of medical services and customer satisfaction. The outcomes level indicates that the ultimate goal is to promote the health for individuals and the whole community.
The personal characteristics in Andersen's behavioural model include predisposing factors, enabling factors and need factors. Predisposing factors include age, gender, race, marital status, education and other demographic characteristics. Enabling factors include income, insurance coverage and medical resource availability due to location and transportation factors. Need factors include the individual's health status. Andersen's model considers the factors that have direct influence on utilization of medical care services. The need for health-care services can be either objective or subjective. Generally, objective needs are usually identified through clinical diagnoses, or measurement in disease severity, limitation in function of activity daily living and prevalence of chronic diseases, whereas subjective needs are determined by individual self-assessment of health condition.
Chang 4 used Andersen's model to analyse the predisposing, enabling and need factors of 2385 patients who continued HD treatments for over two years. The study results showed that age, gender, diabetes, cardiovascular diseases, low albumin, lower vitality and higher level of urbanization are associated with significant differences in predicting the health expenditure for the following year. Lai also identified several risk-adjusted factors for dialysis patients, including age, gender, diabetes, expense from previous health service utilization, and whether or not the patient ever had a kidney transplant. 8 Various studies regarding risk factors for dialysis patients showed that age had a huge impact on medical expenses. For examples, Chang 4 noted that female dialysis patients are more likely to use more health resources than males. Other studies showed similar results. 8–11 Likewise, Arora reported that female dialysis patients tend to have more physician visits, higher outpatient expenditures and length of stay than males. 12 In contrast, Hong 13 reported no significant difference in utilization rate or expenditure with respect to gender. In fact, most researchers report that medical expenditures are most likely to be affected by age than gender.
Most studies report diabetes as one of the most effective predictors of the cost of medical expenditures for dialysis. 10 Bruns et al. (1998) used the 1994–1995 USRDS to analyse medical expenditures for dialysis patients. The results showed that idiopathic diabetes patients had higher medical expenditures ($64,322) than patients without diabetes ($54,369). Other diseases with a significant impact on medical expenditures for dialysis patients include cerebral-vascular diseases, gastrointestinal diseases, cancers, liver disease and cardiovascular disease. 12,13 Other studies showed a rising trend in mortality, admission rate, utilization of medical services and expenditures for dialysis patients when they suffer from combined cardiovascular diseases, cerebral-vascular diseases, gastrointestinal diseases or infections. 9
Mo discussed the impacts of predisposing, enabling and need factors on medical expenditure for dialysis patients, and established a model for billing. 14 This study classified levels of medical resource utilization and provided useful suggestions for building a system to adjust risk factors. A summary of the literature review on the impacts of dialysis patient risk factors on medical expenditure is shown in Table 1.
Literature review: risk factors for dialysis patients
Research methodology
Research subjects and material
This study includes 248 dialysis patients from one district teaching hospital in southern Taiwan from 2005 to 2006. Patients who received fewer than 40 dialysis treatments, for about a three-month period, were excluded; thus, resulting in 177 actual participants.
For each dialysis patient, total cost included fixed and variable cost groups. In the fixed cost group, direct costs were equal to transferred costs (e.g. amortization/depreciation costs and cost for medical manpower). In the variable cost group, different items were consumed for each individual (e.g. costs for oral or injection medicines, medical supplies or laboratory tests). These numbers varied from case to case based on differences in risk factors and dialysis condition. Four variable costs were collected from each individual during the study period and classified as dependent variables in order to analyse the impact of risk factors on cost of dialysis. Real cost data were used for these variable costs, except for the cost for laboratory tests, which was replaced by the standard charging rate defined by the NHIB.
The risk factors in this study included demographic factors, such as age and gender, as well as common risk factors of dialysis patients discussed in the literature. We identified the most common risk factors of dialysis patients by reviewing the medical records of the 177 participants. Those risk factors found in more than three subjects were included in this study. Twenty-three risk factors were included as independent variables. These risk factors included diabetes, hypertension, cardiovascular and cerebral-vascular diseases, chronic obstructive pneumonia, stomach ulcer, liver function disorder, high lipids, high cholesterol, bile-duct diseases, anaemia, bone disease, gout, oedema, dizziness, mental disorder, cancer, urinary-tract infection, asthma, prostate gland enlargement and other demographic factors, such as age, gender and marital status.
Conceptual modelling
This study uses Andersen's ‘behavioural model of access to medical services’ as its conceptual framework. The framework is shown in Figure 2.
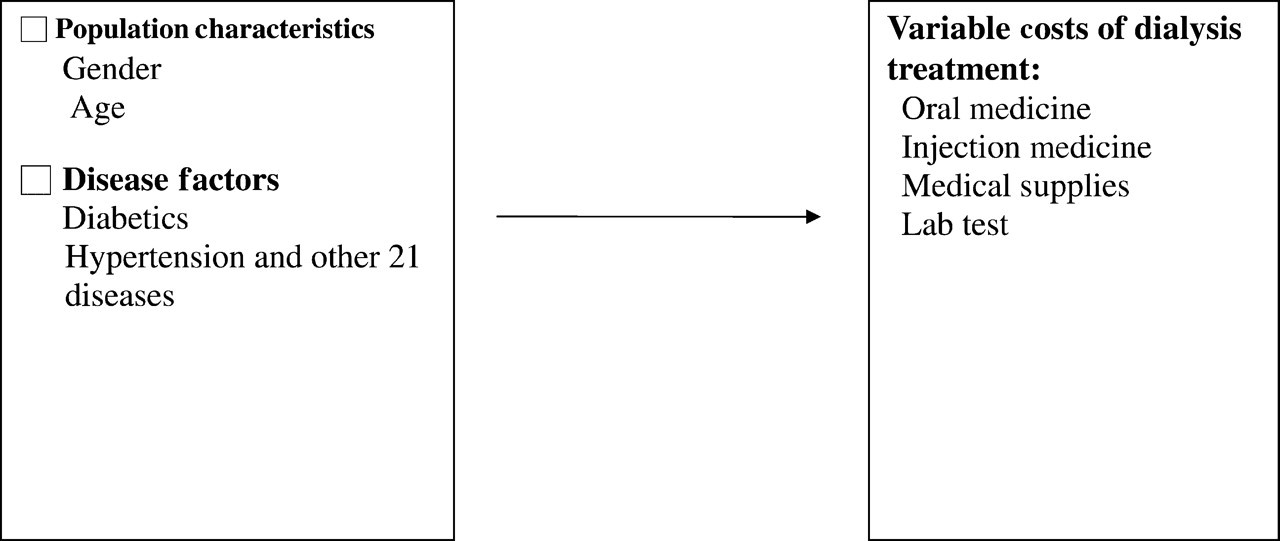
Conceptual modelling for this study – based on Andersen's behavioural model for access to medical services
Data analysis
SPSS (SPSS 10.0 for Windows) was used for data analysis. The statistical methods based on study objectives includes descriptive statistics to describe demographic and disease factors, as well as components of cost; single-variate analysis using independent t-tests, ANOVA and Pearson correlation; multivariate analysis using multiple linear regressions to determine a significant impact of all risk factors on cost, if any; and to discuss those risk factors that significantly affect types of cost among groups.
Results
Descriptive statistics
This study included 86 (48.6%) men and 91 (51.4%) women. The average age was 61.9 years. Table 2 lists the distribution of demographic and disease factors. The average variable cost, which includes costs for oral medicine, injection medicine, medical supplies and laboratory tests, was calculated by dividing the total variable cost of these items by the total dialysis number in that fiscal year (Table 3).
Distribution of population factors and disease factors of study subjects (N = 177)
Consumption of medical cost from study subjects (N = 177)
Among these variable cost items, medical supplies (NT 895.33) and injection medicine (NT 402.89) had higher average costs and variation. The average total variable cost for each dialysis was NT 1474.53 with a standard deviation of NT 214.64 (Figure 3).
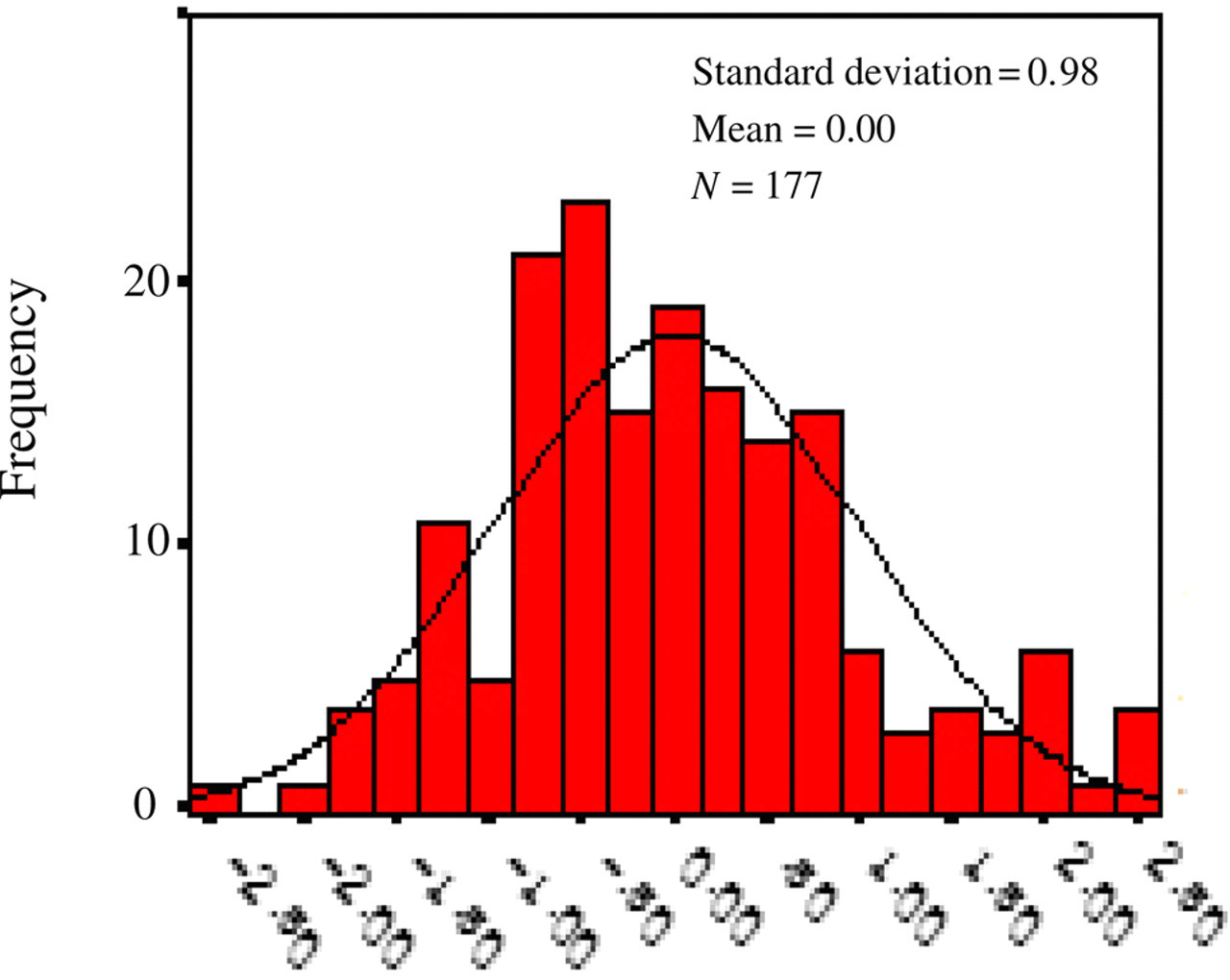
Histogram: dependent variables: total variable costs
ANOVA and Pearson correlation
The independent t-statistic was used to examine if there is a difference on variable cost of each dialysis procedure among risk factors, including demographic and disease factors. Results showed that the variable costs for each dialysis procedure received by subjects with any of these risk factors were higher than costs for those without these conditions. Subjects with the risk factors present significant difference in higher variable cost of dialysis procedure include hypertension (P = 0.000), high lipids (P = 0.01), liver function disorder (P = 0.000), high cholesterol (P = 0.036), cancer (P = 0.012) or bile-duct disease (P = 0.000). However, no significant differences were found between variable cost for the dialysis procedure and the following risk factors: gender (P = 0.565), stomach ulcer = 0.421), cardiovascular disease (P = 0.890), diabetes (P = 0.664), mental health disorder (P = 0.959), cerebral-vascular disease (P = 0.153), chronic obstructive pneumonia (P = 0.605), asthma (P = 0.960) and urinary tract infection (P = 0.050).
ANOVA analysis of variable costs for dialysis in different age groups showed significant differences (P = 0.032) in variable cost among groups. Furthermore, post hoc Scheffe's analysis showed that subjects aged 75 years and older had higher variable costs of dialysis than those younger than 30 years of age. However, Pearson correlation examined the relationship between frequency of dialysis and its variable cost and showed no significant correlation.
Multiple regression analysis
A linear regression model was established and used to examine the effects of risk factors on variable costs for dialysis patients. Risk factors (i.e. demographic and disease variables) included in the multiple regression model of the analysis were liver function disorder, hypertension, bile-duct disease, age older than 75 years, cancer and high lipids. The following regression equation was used:
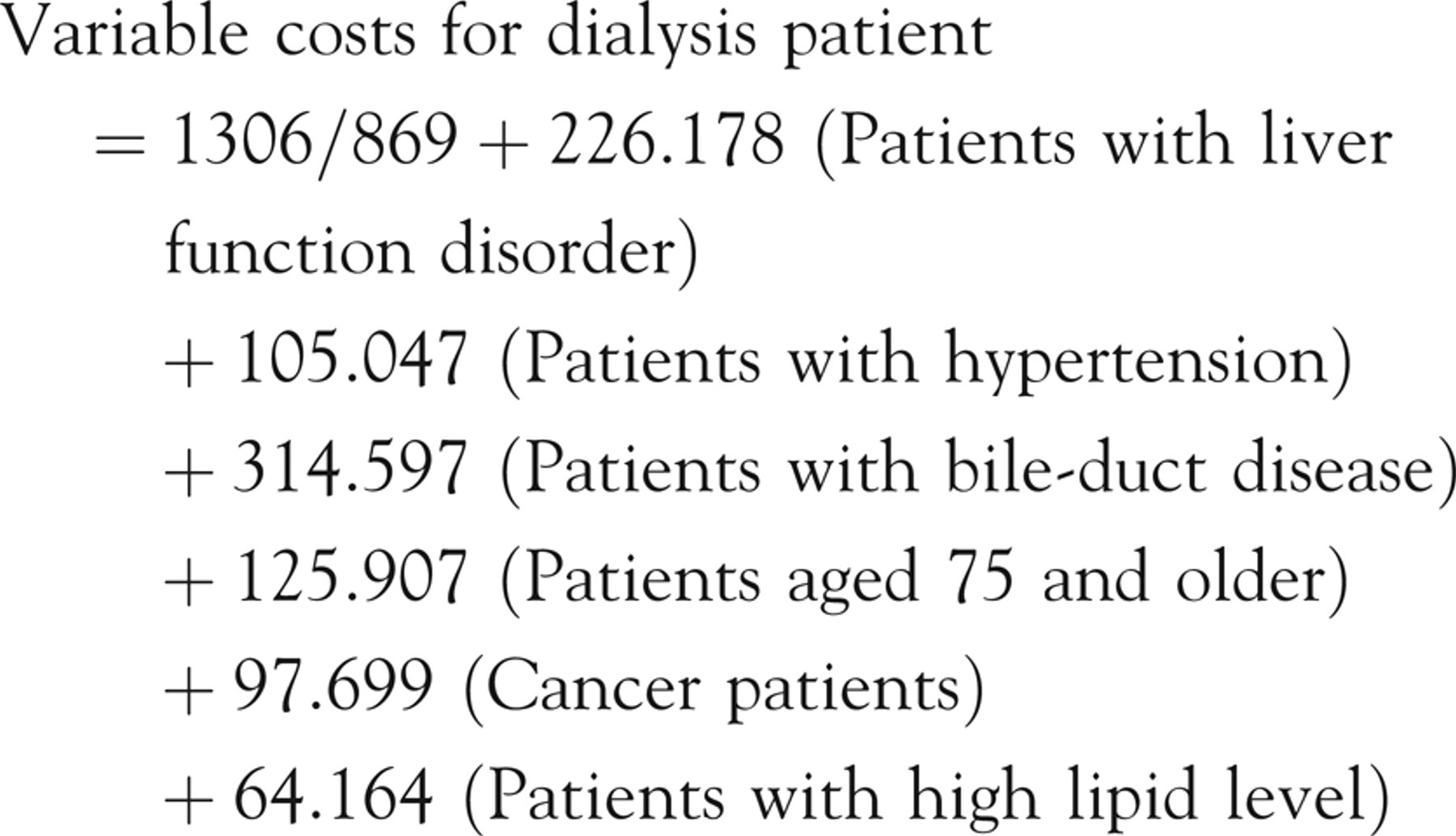
Standardized regression coefficients of risk factors and their relationship with variable costs for dialysis patients show that after controlling for other variables, risk factors such as liver function disorder, hypertension, bile duct disease, high blood lipids, cancer and age 75 years and older are significantly positively associated with variable costs for dialysis patients. Patients with these risk factors had higher average variable costs when compared with those who do not have these risk factors. Similarly, patients aged 75 years and older also had higher average variable costs than those who were less than 30 years of age.
Single variant (correlation) analysis showed that dialysis patients with high cholesterol had higher variable costs than those with normal cholesterol levels. However, when added to the multiple regression model, significant correlations were identified between high cholesterol and other disease factors, such as high blood lipid (0.163) and cancer (0.152).
In the whole diagnosis of correlation for regression model, variance inflation factor (VIF) is used to measure the impact of collinearity among the variables in a regression model. The rule of thumb of using VIF is as follows: values of VIF that exceed 10 are often regarded as indicating multicollinearity, but in weaker models values above 2.5 may be a cause for concern. In this study, there is no formal VIF value for determining the presence of multicollinearity. All VIF values are under 1.1, which is lower than the standard value of 10. The highest value of confidence interval (CI) is 4.760, which is also smaller than 30. This study uses step-wise regression analysis to help researchers include or exclude each individual variable to deal with correlation problems (see Tables 4 and 5).
Analysis of impacts of population and disease factors on dialysis cost
*t-test; **ANOVA
Regression analysis
*F-value = 14.857, which has the significance level of (0.000), D-W value is 2.096
Using the histogram of changes in variable costs on frequency and P-P graphs (see Figure 4 – Normal distribution of standardized residuals), we can test the assumption that if the value from sample is normally distributed. From the symmetrical bell-shape curve of and the straight line of standardized residuals, we can tell that the values from sample observation are very close to a normal distribution.
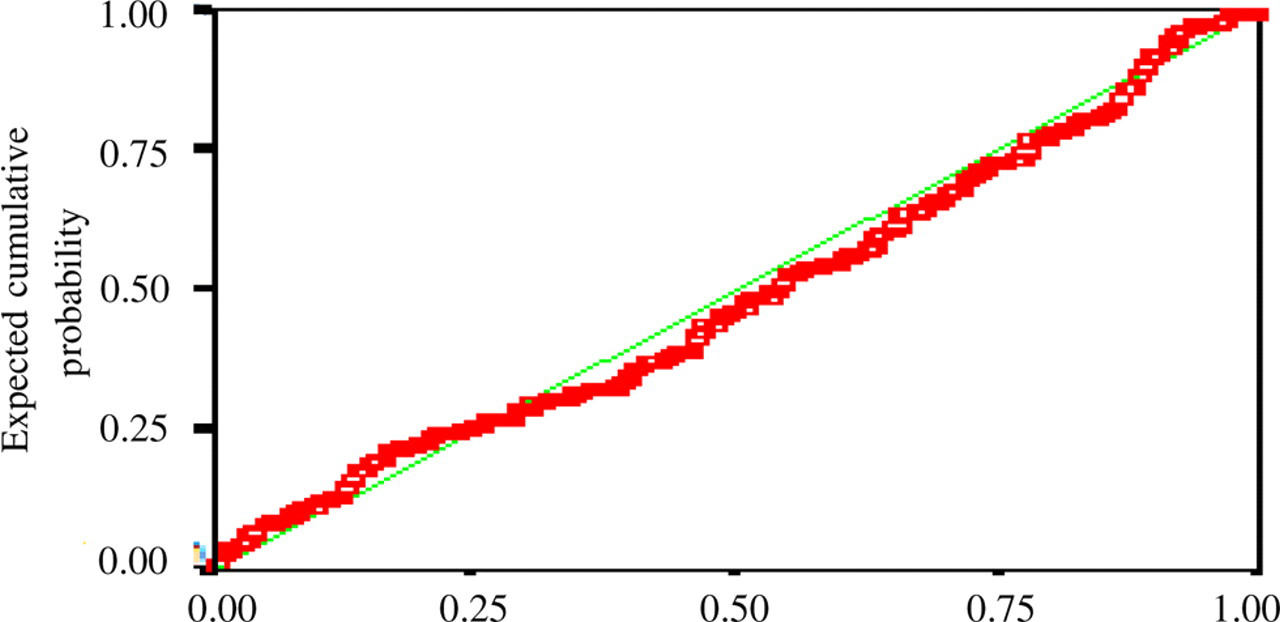
Regression analysis – normal distributional P-P graph for standardized residual error
Cost comparison of significant differences within risk factors
This section discusses six risk factors that were included in the multiple-regression model. In order to compare the four combinations of these six risk factors in the regression model on variable costs, we used independent t-tests to examine the difference in cost of individual risk factors (Table 6). One or more cost items must show a significant difference in variable cost in order to be included as one of the six disease/demographic factors in the multiple-regression model for checking the relating cost combination. For example, patients with liver function disorder had two types of cost (i.e. injection medication and medical supply), which showed substantial significant differences. Hypertensive patients also had higher costs in injection medication, medical supply and even oral medication. Patients with bile-duct disorder had higher laboratory check-up costs. Patients aged 75 years of age and older had higher cost in injection medication than those aged 30 years and younger. Cancer patients had higher cost in medical supply and patients with high blood lipids had higher oral medication cost.
Analysis of significant difference in sources of variable costs
*,**t-test
Conclusion and discussion
The purpose of this study was to identify risk factors associated with consumption of medical resources and their relationship to dialysis costs. Twenty-three common risk factors were found in dialysis patients who participated in the study. Multiple regression analysis showed significant differences in liver function disorders, hypertension, bile-duct diseases, age of 75 or older, cancer and high blood lipids. In addition, patients with these risk factors who received single dialysis had higher variable costs. However, no significant differences were found between variable cost for single dialysis and risk factors, such as gender, stomach ulcer, cardiovascular diseases, diabetes, mental disorders, neurovascular disorders, chronic obstructive pulmonary pneumonia, high cholesterol, constipation, anaemia, skeletal disorders, gout, oedema, dizziness, urinary tract infection, asthma and enlargement of prostate gland. Of the cost combinations associated with independent variables in the six regression models, one or more cost items are needed to show a significant difference. For example, liver function disorder showed statistically significant differences in costs of injection medication and medical supply. Similarly, hypertension presented significant cost differences not only in these two cost items, but also cost of oral medication.
Previous studies used the reimbursement rate (i.e. hospital charge) from the National Health Insurance to measure the consumption of medical resources, but failed to use actual costs (i.e. hospital cost) to analyse the risk factors for dialysis patients. However, the results from this study are quite different. For example, previous studies reported that diabetes and gender affect the medical cost for dialysis. This study showed no statistically significant difference in costs associated with diabetes, cardiovascular diseases, chronic obstructive pulmonary pneumonia and neural-vascular diseases. The only risk factor that was consistent with previous studies with respect to cost differences was being aged 75 years and older. For those risk factors that presented significant differences in cost for dialysis patients, some were similar to previous studies but some were identified for the first time in our study. For example, similar to Hong, 13 liver function disorders and cancer showed significant differences. In addition, this study included bile-duct diseases, high blood lipids and hypertension, which have not been reported elsewhere.
Suggestions and limitations
This study identified the relationship between cost and risk factors of dialysis procedures for ESRD patients based on average variable costs for each dialysis treatment. The results show that certain risk factors (e.g. aged 75 and older, hypertension, bile-duct disease, cancer and high blood lipids) are associated with higher costs. The main difference between this study and previous studies is the use of cost in this study is more closely related to actual resource consumption. Although it has always been an argument about whether to use the hospital cost or charge information to achieve a better performance on cost accounting function, this study suggests that cost information related to actual resource consumption should be crucial and more accurate than charge data for accounting management purposes.
In addition, the results from this study could enable health policy makers and the NHIB to design a fairer and more convincing reimbursement system for dialysis procedures. This study also provides a better understanding of what risk factors play more influential roles in affecting ESRD patients to receive haemodialysis treatment. It will help policy makers and health-care providers in better control or even prevent the disease and manage the distribution of the treatment. In addition, with the results from the analysis of cost information, we can tell which risk factors have more impact on the dialysis cost. It will further help us control the costs for those high-risk dialysis patients more efficiently.
Aside from reviewing all the benefits suggested by this study, we must also consider the possible adverse effects and limitations from it. For example, it is good to have a better understanding of the impacts on cost of dialysis treatment from different risk factors. Researchers should further examine and keep alert in the possibility of access limitation or hindrance for those patients with conditions that we discussed as risk factors in our study to receive the dialysis treatment in time. Luckily, the national health insurance in Taiwan is currently still providing universal and comprehensive care to all people in Taiwan. However, the finding of this study can still be applied in reforming a better reimbursement fee schedule for dialysis patients with different co-morbidity, but not to be used for limiting access to care. Another concern of this study is that subjects collected in this study are from a district hospital in south Taiwan from 2005 to 2006 only. Although some exclusion criteria were applied and seasonal variance were considered, the external generalization power may still be limited. It is suggested that a further study be conducted to include a wider area and different care level of subject collection, such as including subjects from nation-wide, regional hospitals and medical centres.