
Abstract
Secondary shoulder surgery is frequently needed to improve shoulder contracture and movement after obstetrical brachial plexus palsy. This surgery comprises subscapularis release coupled in half the cases with tendon transfers, and is generally performed from ages three to nine years. Postoperatively, a shoulder splint is used to immobilize the shoulder in a position that maintains the released position and prevents tension on the tendon transfer, if performed. A thermoplastic splint design that is light and effective is presented.
Introduction
Children with obstetrical brachial plexus palsy may develop a shoulder internal rotation contracture related to either slow or failed restoration of external rotators. In those cases which fail to respond to physiotherapy, surgical release of the contracture is necessary, otherwise shoulder deformity will result and severely limit function. 1–5 Postoperatively, the released position needs to be maintained using a shoulder splint for four to six weeks, occasionally followed by a further period in a splint. 6 Two splinting positions are required, the first in cases where recovery of the external rotators has been poor, occurs when a subscapularis release is performed with a simultaneous latissimus dorsi transfer to reconstruct shoulder external rotation. This needs a ‘statue of liberty’ position to maintain external rotation with shoulder abduction to reduce tension on the tendon transfer. The second splinting position does not need abduction as there is no tendon transfer and is utilized in children who have adequate motor recovery of the external rotators, and who undergo a subscapularis release alone. This position is with the arm adducted and maximally externally rotated. The traditional plaster or fibreglass shoulder spica is difficult to cast, and heavy and hot to wear. 7,8 This paper presents a thermoplastic alternative.
Design
The thermoplastic shoulder spica design is the same for either situation, though the mode of application differs slightly.
It is a sheet of perforated thermoplastic material with high rigidity, low conformability/high resistance to stretch and uncoated to allow self-bonding is needed. The exact material is not essential as we have used several different manufacturers, types and thicknesses with equal success.
Measure the child and mark the sheet as shown in Figure 1. Cut the rectangular side pieces off. One of these will be rolled to form the supporting bar and the other will form the shoulder strap. This leaves the basic shape (Figure 2).
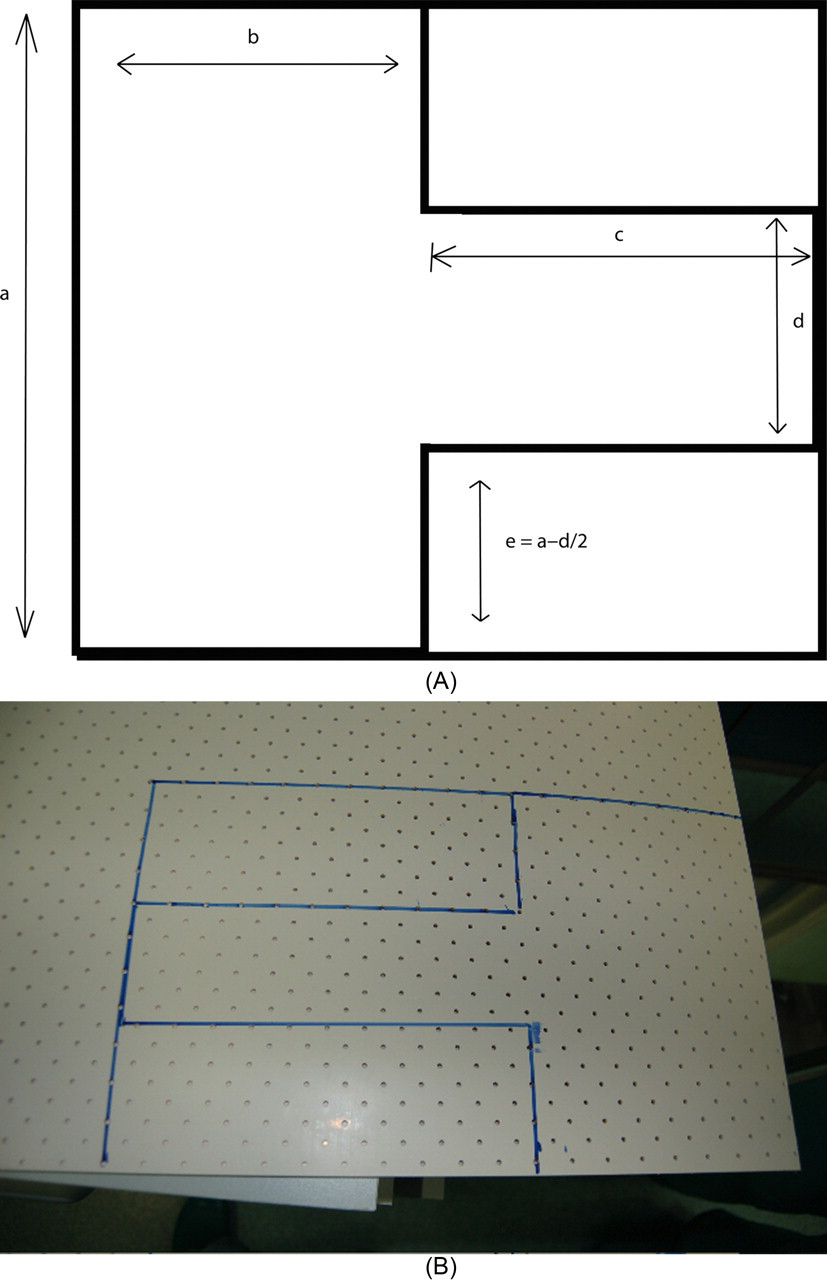
(A) Design and measurements required for the thermoplastic shoulder spica. (a) One-half circumference of chest; (b) axilla to iliac crest; (c) axilla to wrist or palm; (d) one-half circumference of the arm; (e) a − d/2. (B) Design marked on a sheet of thermoplastic
After the shape has been cut
Application
This spica is made at the end of the shoulder release procedure while the child is still anaesthetized. Wrap the torso (or at least three-fourths of it) and arm with ortho wool, with extra padding for the epicondyles and wrist. Your assistant should position the arm in abduction and external rotation with the elbow flexed to 90°and hold the hand. Warm the basic shape, then remove from the bath and place on the child. Conform the torso and the arm piece to the body and limb. Meanwhile heat the rectangular pieces. Remove these and use one to create the shoulder strap and the other as the supporting bar between elbow and torso (Figure 3). This bar should be tubed within the central segment only allowing the end pieces to lie flat on the body and arm plastic and adhere. Wrap in a couple of crepe bandages. These can be removed later and changed for Velcro fastenings or these can be fashioned at the time (Figure 4).

Supporting bar between the elbow and torso components of the ‘statue of liberty’ spica

Spica fitted with velcro straps. Note that the shoulder strap component can be left attached to the main part of the splint as in this case, but this adds unnecessary complexity
To mould the second style of spica where the arm is to be held adducted and externally rotated to the side, the same basic shape is placed on the child, but the assistant should then adduct the arm maintaining the external rotation. The supporting bar is then used as a support between the torso and distal forearm (Figures 5 and 6).

Alternative spica with the supporting bar between the torso and forearm maintaining the shoulder adducted and externally rotated

Rear view of alternative spica
Experience
Since 2002 we have used this splint in 18 cases in children from ages 2 to 14 years and weighing from 10 to 60 kg. Minor modifications are made in the clinic postoperatively to smooth corners, change fastenings and incorporate the wrist if required. There have been no splint failures. There was one rather rotund child in whom a type 2 splint rotated around the torso thus reducing the degree of external rotation. This could have been avoided by extending the length of the torso component of the splint. All the children were able to tolerate the splint for the required four- to six-week period. There were no patients whom had had prior experience of the plaster of Paris or fibreglass type of shoulder spica, but our experience of both indicated that the current design was better tolerated.
Conclusion
We present an easy design to create a thermoplastic shoulder spica in children undergoing secondary surgery for the treatment of obstetrical brachial plexus palsy.
Footnotes
Acknowledgement
Full parental consent was given for the photographs of the children.
Competing interests
None declared.
Hand Therapy has recently adopted the Vancouver style of referencing. As this is different from the referencing used in previous issues of the journal, please check the author guidelines carefully before you submit your paper. The author guidelines can be found at: