
Abstract
Introduction
Ulnar neuropathy at the elbow (UNE) causes sensory and motor dysfunction of the ulnar nerve and can lead to permanent loss of hand function. Hand therapists frequently encounter this pathology and are required to be cognisant of symptoms, diagnosis, therapeutic and surgical management. A detailed understanding of the anatomical structures will give the therapist greater expertise in managing this pathology.
Methods
A single case cadaveric study was undertaken to investigate known sites of ulnar nerve compression and observe the mechanisms by which compression occurs. A literature review reports on knowledge relating to the pathology, diagnosis, therapeutic and surgical management of UNE.
Results
Anatomic structures compressing the ulnar nerve are the Arcade of Struthers, the medial intermuscular septum, the cubital tunnel and the deep flexor aponeurosis. UNE is attributable to mechanical compression from fibrous and bony structures at these sites and to traction on the ulnar nerve from elbow flexion. Provocative tests are a useful tool in the diagnosis of UNE but should be used cautiously due to limitations in statistical accuracy. Conservative treatment approaches of splintage, ergonomic adaptations, education and neural mobilizations lack high-quality evidence but may have benefit primarily for early or mild to moderate disease. There is some evidence in support of conservative management in longer standing disease.
Discussion
Therapists play an important role in the diagnosis and management of UNE and should have a sound understanding of the relevant anatomy, pathology, diagnosis and treatment. Conservative treatment may be efficacious for UNE but lacks evidence from randomized, controlled trials. Further research is needed to verify current precepts and traditional approaches.
Introduction
Nerve compression syndromes of the upper limb are commonly encountered by hand therapists. Ulnar neuropathy at the elbow (UNE), often referred to as cubital tunnel syndrome, is the second most common compressive neuropathy in the upper limb after carpal tunnel syndrome. 1–3 The ulnar nerve is at risk from compression in four distinct anatomical regions of the medial elbow; the Arcade of Struthers, the medial intermuscular septum, the cubital tunnel and the deep flexor aponeurosis. 2–6 These structures form confining spaces through which the ulnar nerve must pass and create the potential for mechanical pressure on the nerve. Compression may also be caused by local soft tissue lesions or inflammatory pathologies. Although UNE is primarily recognized as a compressive or entrapment pathology, it is also considered that traction placed on the ulnar nerve from sustained or repetitive extreme elbow flexion plays an important part in the aetiology of this condition. 2,7,8 The term UNE is used by many authors in preference to cubital tunnel syndrome to encompass the compressive structures distinct from the cubital tunnel, other causes of compression and the pathological contribution of neural tension. 1,2,9,10
A person presenting with UNE may describe pain at the medial elbow and forearm, weakness in grip and pinch strength and paraesthesias in the sensory distribution of the ulnar nerve and if untreated can lead to permanent neural damage and a devastating loss of hand function. 2,11,12 Diagnosis is based on clinical signs and symptoms along with the provocative tests of Tinel's sign, the elbow flexion test and the pressure test. 10,13,14 Electromyography and sonography are used to confirm the diagnosis of UNE and identify the exact locale of compression. 15–17 The hand therapist may need to assess the degree of ulnar nerve degradation through muscle and sensory testing. Conservative approaches to managing UNE include splintage, education, ergonomic adaptations and neural mobilizations. If symptoms fail to resolve sufficiently with therapeutic management, surgical options including simple decompression, subcutaneous or muscular transposition or medial epicondylectomy will need to be considered. 16,17
This paper aims firstly to present the findings from a single case cadaveric study to discuss the anatomy of UNE. This study was undertaken to examine the ulnar nerve and identify the well-known sites of compression at the elbow. These anatomic structures are described with regard to their consistency with the literature and the mechanisms by which ulnar nerve compression occurs at these sites. Secondly the findings of a literature review will be presented in order to discuss and synthesize knowledge on the pathology, diagnosis and management of UNE.
Method
A literature search was undertaken to identify studies related to the anatomy, pathology and treatment of ulnar compressive neuropathy. Databases searched were EbscoHost Health Databases (excluding Medline), Medline via Ovid, and Proquest Dissertations and Theses. Terms searched included; ulnar nerve, anatomy, compressive neuropathy, cubital tunnel syndrome, excursion and elongation, nerve glides, neurodynamic mobilization, physiotherapy, occupational therapy, splinting, education, provocative testing and surgery.
The abstracts were reviewed for each subsection with regard to the methodology and clinical relevance of the studies. In respect to anatomy, cadaveric case studies were selected on the basis of relevance, well-described procedures and where possible those with specimen numbers greater than 10. Inclusion criteria for studies pertaining to diagnosis were primary research investigating the statistical accuracy of diagnostic tests. In relation to conservative management emphasis was placed on accessing high-quality studies from randomized controlled trials. Due to the lack of research however, it was not possible to exclude case series, experimental designs lacking proper controls or randomization and studies with low participant numbers.
A single case cadaveric dissection of a left upper limb was completed at the School of Medicine, University of Auckland, as part of the requirements for the Clinical Anatomy paper of the Post graduate Diploma in Health Science, AUT University Auckland, New Zealand. The ulnar nerve was dissected from the mid-dorsal humerus into the palm of the hand on a left upper limb prosection. The reported sites of compression were located in a proximal to distal manner and carefully dissected to reveal the anatomy at each locale. The arrangement of anatomical structures and their potential for compression of the ulnar nerve was investigated by observation and palpation and with reference to the literature. The effect of elbow and forearm joint motion on the ulnar nerve was also observed. A photographic and written record was taken throughout the dissection to compare and contrast findings with those reported in other cadaveric investigations.
Results
Literature review
There were 37 articles included in the final review. In relation to the anatomy of the ulnar nerve, nine cadaveric or biomechanical studies and two review articles were finally selected. Cohort, experimental and review articles totalling nine were selected to discuss diagnosis, pathology and provocative testing. There were no randomized controlled studies relating to splinting, ergonomic adaptations, education or neural mobilization. On the basis of the criteria already described three articles on splinting were finally selected, one pertaining to education and five to neural mobilization. There were 10 narrative or systematic review articles selected due to clinical relevance and summation of knowledge.
Anatomy
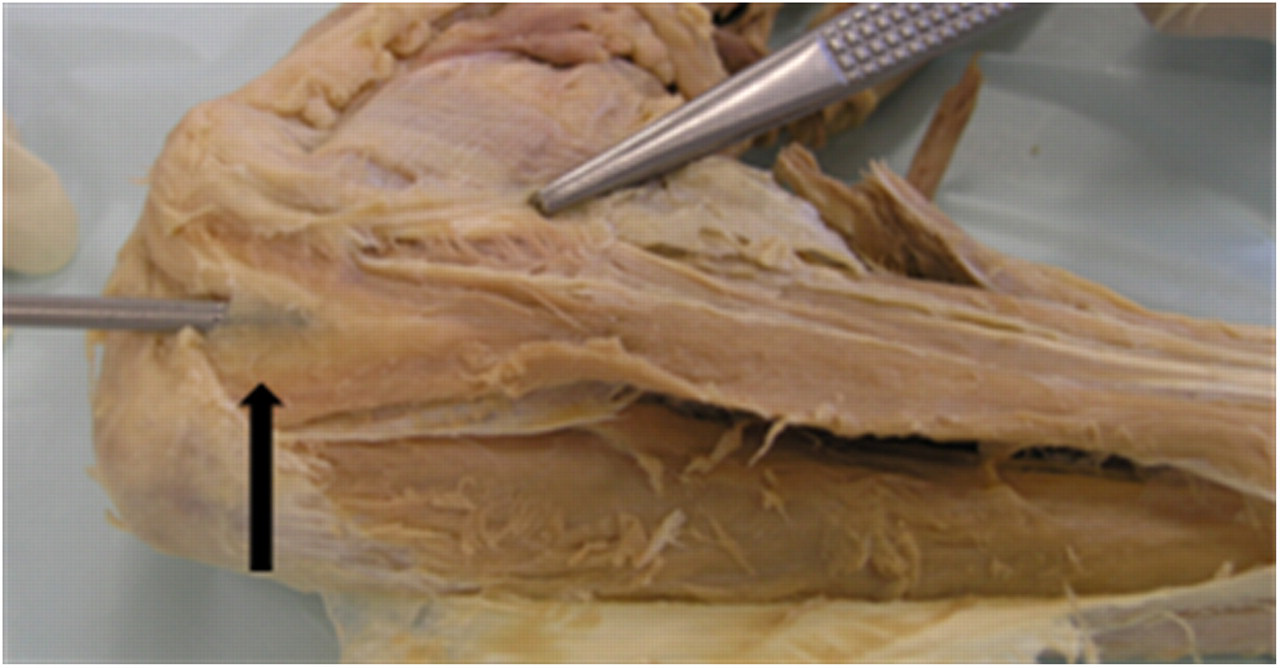
There are four sites in the medial elbow where compression of the ulnar nerve is known to occur, namely the Arcade of Struthers, the medial intermuscular septum, the cubital tunnel and the deep flexor aponeurosis. 2,3 The most proximal structure is the Arcade of Struthers (Figure 1), which was found to be consistent with descriptions as that of a deep fascial band connecting the medial head of triceps to the medial intermuscular septum. 12,18 The ulnar nerve exits beneath the Arcade of Struthers via a V-shaped opening and is recognized as a confined space that has potential for compression of the ulnar nerve. 4,12,18 The medial intermuscular septum was then identified spanning the Arcade of Struthers and the medial epicondyle, and dividing the anterior and posterior compartments of the arm (Figures 2 and 3). This structure can be problematic for compression or friction particularly at its distal edge where the fibrous septum attaches to the medial epicondyle. If the ulnar nerve subluxes over the medial epicondyle during elbow flexion, the nerve can become entrapped between the skin and this taut fibrous structure. 4,19
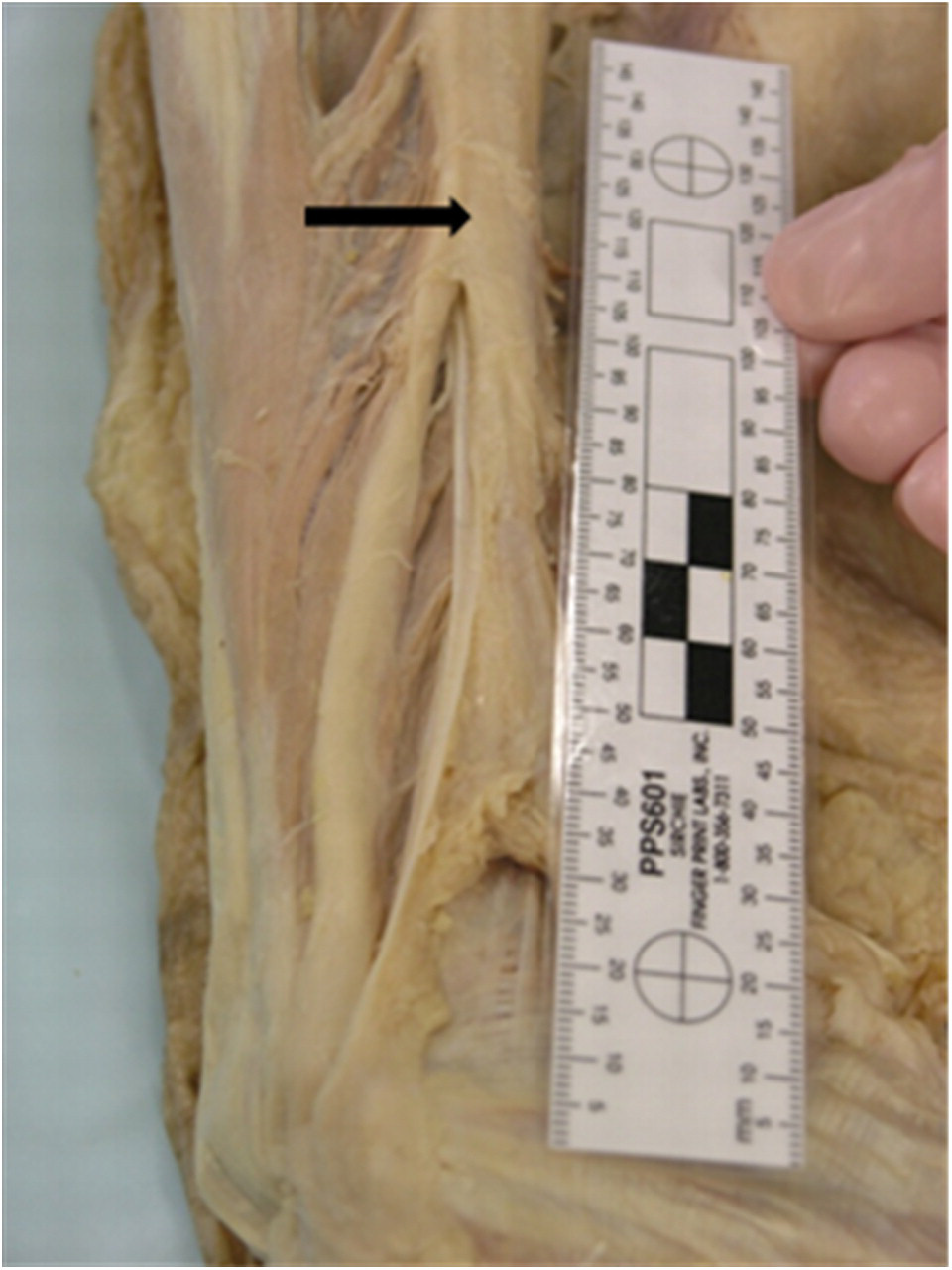
Arcade of Struthers

Medial intermuscular septum. The distal edge can be seen in close proximity to the ulnar nerve

Medial intermuscular septum
The cubital tunnel is formed by osseous and fibrous structures in the medial elbow through which the ulnar nerve must pass. The roof is described as being formed by a retinaculum spanning the medial epicondyle and the olecranon and the aponeurosis between the two heads of flexor carpi ulnaris (FCU). 3,19–21 The floor and medial borders are formed by the medial collateral ligament and epicondylar groove, respectively. The retinaculum proper was absent in the current study and the tunnel was formed by the more distal FCU aponeurosis, which was clearly identified (Figure 4).
Flexor carpi ulnaris aponeurosis
The absence of a retinaculum was reported by O'Driscoll et al., 19 in 30% of specimens and was described as causing subluxation of the nerve during elbow flexion due to its lack of restraining function. In the current study however, subluxation may have been prevented due to the depth of the epicondylar groove and by tethering of the nerve to the floor of the tunnel via a subneural fascia (Figure 5).

Subneural fascia at cubital tunnel
Compression on the ulnar nerve in the elbow is most notably associated with elbow flexion of greater than 90° whereby the retinaculum is stretched, the space within the tunnel reduces and the ulnar nerve is forced against bone and taut ligamentous structures (Figure 6). 7,21 Pressures within the tunnel in excess of 200 mmHg have been recorded with full elbow flexion; and can increase further with maximal contraction of FCU. 7,22 Additionally the cubital tunnel is superficial and prone to external forces such as injury and leaning on one's elbow.

Elbow in >90° flexion showing ulnar nerve forced against medial epicondyle
The most distal compressive structure is the deep flexor aponeurosis. This was identified and seen to serve the function of a septum separating the fibres of FCU and flexor digitorum superficialis, and arising from the muscle belly of flexor digitorum profundus. This aponeurosis forms a distal elliptical tunnel up to 10 cm from the medial epicondyle, which can compress the ulnar nerve at pressures greater than those in the cubital tunnel proper, and failure to release this structure may result in persistent ulnar nerve symptoms following surgery. 3,5,6,20
Discussion
Pathology
UNE is a compression neuropathy that causes medial elbow pain and paraesthesias in the ring and little fingers and may be reported by patients as occurring only at night or with certain activities such as wearing a sling, driving, computer use or throwing sports. 2,11,15,23–25 These symptoms are induced by mechanical pressure on the ulnar nerve due to anatomically compressive structures in the distal arm, medial elbow and proximal forearm. Neural compression may also result from external pressure such as leaning on one's elbow or due to soft tissue masses within the cubital tunnel including ganglia, lipomas, cysts, tophaceous gout or thickened synovium. 2 Added to compression is the aetiological factor of nerve traction whereby the nerve is placed on stretch in full elbow flexion with this effect increasing even further if postures of shoulder abduction and wrist extension are added. 8,21,23,26 The neural response to compression or stretch is that of inflammation, ischaemia and a subsequent loss of axonal transport. 2,27,28 Thickening of the perineurium and endothelium also occurs and can result in an enlarged nerve proximal to the site of compression. 24 Change in sensation is generally the first symptom to be noticed, which is thought to be due to the sensory fibres being more superficial in the ulnar nerve at the elbow than motor fibres, however if compression and repetitive traction are sustained over time loss of innervation to muscles will occur. 15,24,29 This repetitive trauma to the nerve results in a gradual degeneration of normal nerve physiology, and in its most advanced form can result in complete denervation of the muscles supplied by the ulnar nerve and development of a classic claw deformity. 2,15
Diagnosis
The diagnosis of UNE is based on findings from presenting symptoms, examination, use of provocative tests and electromyography. Initially, clinical findings of localized pain or tenderness at the medial elbow, night-time paraesthesias, aggravation of symptoms with elbow flexion and motor or sensory changes of the ulnar nerve in the absence of previous injury should alert the clinician to the presence of UNE. 11,29 An array of tests has been described for determining the locality, motor and sensory differentiation and severity of ulnar neuropathy in the upper limb. The most widely used provocative tests for determining the presence of UNE are Tinel's sign, the elbow flexion test, the pressure test and the combined pressure and flexion test, and several studies have examined their accuracy. 10,13,14 In addition, the clinician may conduct tests that determine the degree of sensory and motor degeneration of the ulnar nerve. These will include sensory testing with Semmes–Weinstein monofilaments, manual muscle testing and a number of motor tests including Froment's and Wartenburg's signs, pinch and grip strength, and the crossed finger test. 2,11,15,29 Electromyography and to a lesser extent magnetic resolution imaging have been traditionally used by physicians to confirm the diagnosis of UNE. 15–17,30 Recent work by Beekman et al. 30 has suggested that high-resolution sonography is an accurate and lower cost addition to the tests available to accurately determine the presence of UNE.
Provocative tests are widely advocated in the diagnosis of ulnar neuropathy but have been criticized for their lack of sensitivity, specificity and predictive value. 10,29 Tinel's test and the elbow flexion test are the most commonly described tests; Tinel's test constitutes manual percussion of the ulnar nerve and the flexion test is when the elbow is held flexed for 60 seconds; both are considered positive if paraesthesias are provoked or worsened. 13,29 The flexion test is often combined with the pressure test where external pressure is applied by the examiner just proximal to the cubital tunnel. 13,29 Novak et al. 13 reported a sensitivity and specificity of 98 and 95%, respectively, for the combined pressure test and 70 and 98% for Tinel's test. Beekman et al. 10 re-evaluated the accuracy of these tests in a much larger population (n = 192) comparing findings against electromyography and sonography reporting much lower sensitivity and specificity at values of 62 and 53% for Tinel's and 61 and 40% for the flexion compression test, respectively. Further evidence disputing the accuracy of these tests was reported by Rayan et al., 14 who found that the flexion test was positive in up to 13% of non-symptomatic individuals.
Despite criticisms, these provocative tests remain useful tools for the therapist in the initial diagnosis and exclusion of other pathologies. They should be interpreted with considerable caution and with reference to clinical findings and the results of electromyography and sonography if available. The therapist must always be alert to the fact that a positive finding from a provocative test may not represent a true pathology and further examination should always ensue.
Conservative management
Non-surgical approaches are considered to be an essential component of managing UNE and are frequently successful at alleviating symptoms and preventing disease progression. 2,11,15,31 Conservative management aims to reduce inflammation of the nerve, restore vascularity and normal axonal transport by relieving compression within the cubital tunnel and the traction associated with extreme elbow flexion. 16 Strategies that can prevent provocation of neural symptoms include education; avoidance of repetitive or sustained elbow flexion; ergonomic adaptations; avoiding external compression; splinting and neural mobilizations. 2,15,32–35
Splinting
Splinting the elbow in extension at night is considered to be a standard component of conservative management with authors consistently reporting improvements following a period of splintage. 11,36 The premise of extension splinting is that compressive forces to the ulnar nerve are alleviated and nerve repair is promoted. 2 This is based on cadaveric and in vivo studies that have demonstrated highest pressures within the cubital tunnel when the elbow is flexed greater than 90° 20,22 and lowest pressures between 40° and 50° elbow flexion. 7 Extension of the elbow also reduces strain and elongation of the ulnar nerve. Wright et al. 8 demonstrated that elbow flexion, wrist extension and radial deviation causes the greatest degree of strain to the ulnar nerve and that elbow flexion alone can increase tension by 29%. Splinting therefore aims to avoid the positions of greatest nerve traction again promoting nerve repair and reducing symptoms of pain and transient sensory loss.
A number of studies have shown positive effects following a period of night extension splintage. 34–36 The elbows in these studies were variously splinted at 15°–45° flexion during the night time for periods of up to six months. Overall the greatest improvements were seen in patients with less severe disease pathology with Dellon, Hament and Gittelshon's study 36 showing complete resolution in 42% of patients with intermittent paraesthesias and Hong et al., 35 reporting an improvement in all patients with mild or moderate disease. Improvements however have been reported in longer standing disease and in those with permanent sensory changes and in the case of Seror, 34 in three patients where surgery had previously failed. These findings contend with literature stating that splinting is not recommended for other than mild or recent onset of symptoms. 2,15 Optimal angles for splinting the elbow have not been conclusively found, however most authors recommend between 35° and 70° consistent with findings of lower cubital tunnel pressures in these angles. 7,11,15,20,22 Splinting is generally advocated for the elbow alone however some authors recommend including the wrist in flexion to relax FCU and further reduce tension on the nerve, in cases where symptoms are more severe. 11,31 Similarly, in more severe cases, splinting during the day has been advocated for short periods in an attempt to unload the ulnar nerve and promote nerve recovery. 2,11 Detrimental effects of splinting are primarily reported as discomfort of wearing a splint, disturbed sleep, risks of additional pressure at the medial elbow and interruption to daily activities if splint wearing is required during the day. 2,11,35
Despite lack of randomized trials and definitive guidelines regarding duration, type of splint and optimal position, extension splinting remains widely used in clinical practice due to convincing evidence from pathophysiological studies, case series and comparative studies. The key findings are that splinting can be effective in improving but not necessarily eliminating neural symptoms in many cases and that several months of consistent splinting may be necessary for improvements to occur. Findings that splinting can be effective even in more severe disease suggests that the premise of using conservative management in only mild or moderate disease may not be justified.
Ergonomic adaptations
Ergonomic adaptations and advice on resting positions have been recommended for alleviating static and dynamic forces to the ulnar nerve. Many occupations and activities have been associated with elbow ulnar neuropathy including musicians, sports involving throwing or batting a ball, factory workers, activities that involve digging or hammering and repetitive computer use. 2,23,25 Such repetitive stress to the ulnar nerve can cause microtrauma leading to an ongoing inflammatory response, transient ischaemia and fibrosis of the ulnar nerve. 2,23,33 No studies to date have studied the effect of any one or more ergonomic changes on UNE in isolation. Many authors recommend an evaluation of aggravating work and lifestyle factors and subsequent task adaptation or use of adaptive equipment to alleviate stress to the ulnar nerve. 2,11,15,36 Examples of such adaptations include placing a pillow beneath the elbow when seated, avoiding sitting with the arms crossed, use of a bookstand or telephone headset and adjusting the computer workstation to allow for greater elbow extension. 2,9,36
Education
Education is seen to be a significant part of management for UNE and is woven into most non-surgical approaches however authors often fail to acknowledge the value of instruction or evaluate it as a standalone treatment. Only one study by Nakamichi et al., 9 has examined patient education in isolation. These authors conducted a case series on 77 patients whereby education on the disease pathophysiology, advice on modifying activities, and changing sleeping and aggravating postures of the upper limb was the only intervention provided. An education leaflet was supplied and regular follow-up given for up to one year. Overall, excellent or good outcomes were recorded in 66% of cases and as with splinting, improvements seen most markedly in less severe cases. Improvement was still recorded in patients with advanced disease however, further adding to evidence that conservative measure can be effective in longer standing disease if treatment persists over many months. It is unfortunate that Nakamichi et al. 9 did not include a control group to identify if the effects seen were indeed due to education or some other variable such as the natural course of the disease. Beekman et al., 24 compared outcomes of patients undergoing either surgery or education. They reported less favourable results in the education group with only 35% having improved or resolved by six months compared with 61% in the surgical group. The groups however, were not homogenous in nature with the conservative group having less severe symptoms; also, the quality of the education was questionable as it consisted of very simple instructions at a medical appointment on what postures to avoid and there was no follow-up to ensure understanding or compliance as with the Nakamichi et al., 9 study. Considering the limitations of the education intervention it is positive that 35% of patients had improved and it would have been interesting to know whether a more intensive and targeted education programme could have resulted in better outcomes for more patients.
Other studies 32,33 have included patient education as part of usual care but have not examined it as a standalone intervention, perhaps believing that education is a generic strategy that should accompany more directed interventions. Oskay et al. 33 and Coppieters et al. 32 both included education in their studies on neural mobilization and in fact Oskay et al., 33 placed particular importance on the role of education. As neither of the studies included a control group to compare outcomes it is possible that the improvement in their patients may have been due as much or in some part to the education they received as to the neural mobilization treatment.
Insufficient evidence therefore exists to conclude that education alone will resolve UNE; however, it stands to reason that if patients are adequately educated and can subsequently modify activities to alleviate the stresses to the ulnar nerve that improvements should be expected. Further studies should evaluate the effect of this low-cost intervention on UNE but education programmes must be well designed and based on sound health education principles.
Neural mobilization
Neural mobilizations have been advocated for the treatment of Cubital Tunnel Syndrome; 27,28,32,33 however considerable debate continues to exist regarding the mechanism of action, application and efficacy of this treatment approach. 11,37 The nervous system is designed for mobility and nerves have the ability to elongate, tension and glide both within the nerve bed and alongside adjacent tissue in response to joint motion. 26,38 The ulnar nerve has to accommodate for motion in all joints of the upper limb with particular demand at the elbow joint. Several authors have demonstrated that up to 22 mm of ulnar nerve gliding at the elbow is necessary to accommodate normal elbow movement and that up to 29% elongation of the nerve also occurs with elbow flexion. 8,27,38 Following trauma or sustained force to a nerve, inflammation, reduced vascularity and absence of lymphatic drainage can result in the formation of fibrotic tissue and a subsequent loss of excursion between the mesoneurium and adjacent tissues and within the nerve itself. 32,33 This loss of normal neural glide may inhibit the nerves ability to adapt to the demands of motion and consequently even normal daily activities may cause further nerve damage. 32,33
Neural mobilization techniques claim to restore normal nerve physiology through increasing vascularity to the nerve thereby promoting dispersal of local inflammation and limiting the formation of fibrotic scar tissue. Additionally, nerve glides may reverse central nervous system changes and the sensitization that can occur with nerve injuries. 28,32,33 Early approaches to neural mobilizations focused on progressive elongation of the nerve bed and although care was taken to avoid overstretch, nerve glides have been criticized for exacerbating symptoms. 11 More recently, Coppieters and Butler 27,32 introduced a less aggressive approach of nerve ‘slides’ where alternating movements load the nerve at one joint and unload it at an adjacent joint thereby ‘sliding’ the nerve with minimal tension on the entire length of the nerve. 27,32 Evidence for this theory has been put forward by the same authors who found that twice the amount of ulnar nerve excursion occurred in the elbow when using slides as opposed to tensioning techniques used to mobilize the nerve. 27 Two studies have examined the efficacy of this approach with UNE; Oskay et al. 33 reporting on a case series of seven patients and Coppieters et al., 27 in a single case study. With both these studies nerve slides were performed in the clinic by the treating therapist and by the patients as part of a home programme in addition to education and muscle strengthening. All patients in the studies showed improved symptoms after 4–6 weeks which was maintained at 10–12 month follow-up. It is difficult to be able to attribute the effect seen solely to neural mobilizing due to the lack of a control group and as the improvements may have occurred due to normal healing or to the patients self-correction of aggravating postures as a response to the education they received. There is a clear need for this approach to be tested in more rigorous trials with larger sample sizes and randomization.
Surgical management
Findings from studies show that the ulnar nerve can be subject to anatomical compression at any of four sites in the medial elbow region with the cubital tunnel being the most common locale. In cases where conservative treatment has failed to improve symptoms or for the more severe spectrum of disease severity surgery may be required to relieve compression and traction of the ulnar nerve and restore normal neural physiology. 2,11,36 The most widely used surgical approaches for management of UNE are decompression, transposition of the ulnar nerve and medial epicondylectomy. Decompression techniques aim to release restrictive structures and are said to constitute less trauma to the nerve itself as there is no disturbing of the nerve bed or the fascia attaching the nerve to the cubital tunnel floor. 16 There is an inherent risk of nerve instability and subluxation following decompression particularly if the nerve has been released at more than one site; additionally decompression does not relieve the traction associated with UNE. 2,16,38 Removal of the medial epicondyle claims to preserve the vascularity of the ulnar nerve while removing the source of compression with less dissection and trauma to the nerve. 16 Transposing the nerve anterior to the medial epicondyle is performed to both decompress restrictive structures and relieve nerve traction while allowing for full exploration and resection of problematic structures. There appears to be a consensus that evidence is lacking to demonstrate the superiority of one surgical technique over another, although there is a trend towards favouring transposition of the nerve over decompression due to the ability of this technique to relieve tension on the nerve. 11,16,17
Outcomes following surgery are unpredictable and vary mostly according to the preoperative disease severity. Yamamoto et al. 17 showed that motor loss, muscle atrophy, advanced sensory loss, age greater than 60 years and disease duration of greater than three years were factors predictive of worse outcomes following surgery. Beekman et al., 24 used sonography to examine the diameter of the ulnar nerve pre- and post-operatively and determined that a thickened nerve was associated with the poorest outcomes. Conversely they determined that a motor conduction slowing and block on electromyography were prognostic of a better outcome possibly due to the reversibility of demyelination. Ultimately, the decision to perform surgery must be based on knowledge of the restraining structures, previous response to conservative treatment and the progression of the disease itself. 2,11,16 Due to the findings that outcomes are much worse for patients with advanced UNE it is imperative that the therapist closely monitors the response to conservative treatment and frequently measures motor and sensory function of the ulnar nerve. If there is any evidence of muscle weakness or other than transient sensory loss a surgical opinion should be sought immediately.
Conclusion
UNE is a common condition resulting in pain and dysfunction of the ulnar nerve attributable to mechanical pressure and traction. This paper has given an overview of the anatomy, pathology, diagnosis and management of UNE. Anatomical structures that can compress the ulnar nerve are the Arcade of Struthers, the medial intermuscular septum, the cubital tunnel and the deep flexor aponeurosis. Compression may also be caused by pathologies such as tumours, cysts or tophaceous gout. Elbow flexion places the ulnar nerve on stretch and is believed to contribute to UNE. A plethora of tests are used to diagnose UNE and the clinician must be aware of their purpose and limitations. Although the provocative tests of Tinel's sign and the elbow flexion test are widely used, their statistical accuracy has been questioned and should only be used in conjunction with clinical signs and symptoms and electromyography. With the advance of high-resolution imaging, sonography has given clinicians another tool to assist in diagnosis.
Conservative approaches including education, ergonomic adaptation and splintage are widely used in clinical practice but lack high-quality research to support their efficacy. It is asserted that these strategies are mostly effective in the earlier stages of disease pathology and prior to the onset of permanent parasthesias or motor denervation. Some evidence suggests however, that conservative management may have a role in longer standing disease if sufficient tension and compression can be taken off the nerve over a period of several months. Evidence is emerging for the use of novel neural mobilization techniques and should be considered by the clinician when treating UNE. Sound clinical reasoning and knowledge of neuropathy must be applied to avoid provocation of symptoms or further degradation of the nerve. Further studies of these treatments, which include controls and randomization, would greatly assist therapists to select the most efficacious treatments.
Surgical intervention is generally considered necessary in cases where conservative management has failed to resolve symptoms or in the presence of other than transient paraesthesias. The recovery of normal nerve function in the presence of motor loss is uncertain for either conservative or surgical intervention. For the majority of patients with UNE however, a positive outcome can be expected if the pathology is managed in a timely and considered manner by both surgeon and therapist.
Footnotes
Acknowledgements
Many thanks to the Department of Anatomy with Radiology at the School of Medicine, University of Auckland for access to the anatomical and technical resources.