
Abstract
OptionE incorporates nurse-led HIV clinics, review of blood results by doctors, patient contact by email and the option of home delivery of medication. Patient questionnaires showed increased satisfaction associated with fewer, shorter clinic visits. A retrospective case note review suggested clinical outcomes are as good as standard care.
Introduction
The number of individuals accessing HIV care in the UK is rising, and reached 47,500 in 2005, up to 13% in 2004. 1 To cope with increasing workload, the Victoria Clinic for HIV and Sexual Health introduced OptionE in 2004. Patients have blood taken at a nurse-led review clinic. Results are checked by a doctor or supplementary prescriber and the patient notified by email. If necessary, information is sent via web links or attachments, or the patient is advised to attend the clinic. Patients can also choose face-to-face consultations at any time. Medications are collected from the clinic or delivered to any UK address. Home delivery saves money because value added tax is not paid.
Patients are suitable for OptionE if they have adjusted psychologically to their HIV diagnosis and are stable on or off antiretroviral therapy, with no unresolved medical issues and reliable access to a confidential email account. At the time of writing, 268 of our HIV cohort of 801 adults are enrolled on OptionE.
Methods
Case note review
A retrospective case note review was performed of the first 100 patients joining OptionE. Demographics were compared with our whole HIV cohort. The rates of hepatitis B and C testing were compared over the same time period with the first 100 patients who joined OptionE the following year. Virological failure and adherence assessments were recorded. Qualitative data are presented as numbers with percentages. Between cohort comparisons were tested using chi-squared statistics, and where applicable Yates’ correction was applied.
Patient questionnaires pre-OptionE and on OptionE
At registration and one year later, OptionE patients completed a questionnaire about their clinical care. The two responses were compared. Differences in quantitative data are presented as mean difference with 95% confidence interval (95% CI). For responses to a Likert scale, kappa statistics were calculated. A weighted kappa was used so responses close on a Likert scale (e.g. 1–2) were given greater weight than those further apart (e.g. 1–3). Perfect agreement is indicated by weighted kappa of 1 while 0 indicates no agreement.
Data analyses were carried out using SAS version 9.1 (SAS Institute Inc., Cary, NC, USA). All P values are two-tailed.
Results
Case note review
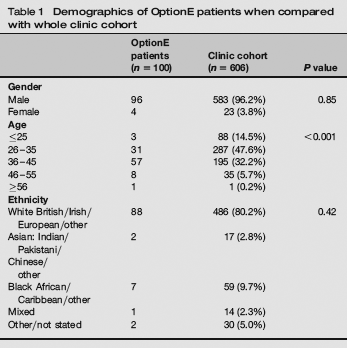
The first 100 patients who registered with OptionE did not differ from the general HIV cohort in gender or ethnicity (Table 1) but were significantly older (P < 0.001). Seventy-three were on antiretroviral treatment. Home delivery of medications was chosen by 59% (43/73).
Demographics of OptionE patients when compared with whole clinic cohort
After 12 months, 84/100 patients continued on OptionE. Five had left London. Eleven reverted to doctors’ appointments for reasons including mental health issues (2), no email access (1), acute hepatitis C (2), finding OptionE confusing (1) and preferring face-to-face consultations (3).
In those completing one-year follow-up, post-exposure prophylaxis and sexual health were discussed with 95% (80/84). Hepatitis B immunity was assessed in 99% (83/84) and hepatitis C screened in 98% (82/84). This was significantly better than the comparison group in whom 47% were tested for hepatitis B and 53% for hepatitis C (P < 0.001).
No patients on antiretroviral therapy experienced virological failure. All had a recorded adherence assessment.
Patient questionnaires
Initial questionnaires were available for 136/162 patients who had joined OptionE by May 2006 (84% response rate). In June 2007, 121/136 continued on OptionE, and 92 repeated the questionnaire (76% response rate).
Patients made a mean of 3.1 fewer clinic visits in 12 months (95% CI: 2.0–4.2). Reported time in the clinic per visit was reduced by a mean of 11 min (95% CI: 5.4–16.4).
Patients overall reported increased satisfaction for obtaining test results and medication, and said it was easier to access appointments (Table 2). The level of agreement between responses pre-OptionE and on OptionE was low (as indicated by kappa statistics), suggesting that a significant shift had occurred.
From routine clinic care to OptionE: change in patient satisfaction scores
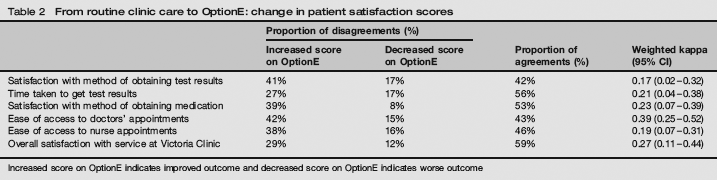
Increased score on OptionE indicates improved outcome and decreased score on OptionE indicates worse outcome
Discussion
OptionE incorporates nurse-led clinics and doctor–patient communication by email. Our study suggests the quality of care is at least equivalent to standard clinics. OptionE improves patient choice, and levels of satisfaction increased. The number and length of clinic visits reduced, and this appeared to improve appointment availability, which would benefit the clinic's whole HIV cohort. However, this model is not suitable for everyone, and our study did not investigate those who were offered OptionE but declined.
The improvements in the health of people with HIV mean many have busy working lives. This model delivers an effective, patient-centred approach without compromising care.