
Abstract
Fine-needle aspiration (FNA) cytology has an established role in the investigation of lymphadenopathy in HIV-infected patients. However, changes in the spectrum of disease have been observed since the introduction of highly active antiretroviral therapy (HAART). The aim of the study was to establish whether FNA cytology remains a useful investigative tool in the post-HAART era and to determine whether the cytology results reflect the changing patterns of disease. Retrospective search of the cytopathology database at University College London Hospitals identified 73 FNA cytology procedures performed in 62 patients between January 1998 and December 2006. FNA cytology showed significant disease in 90% of adequate samples. The most common diagnoses were persistent generalized lymphadenopathy (PGL, 50%), infection (22%) and malignancy (18%). Diagnoses could not be made in 31 % of patients because of inadequate sampling. An open lymph node biopsy was subsequently performed in 27% of patients. FNA cytology remains an important initial investigation in the post-HAART era, particularly in the diagnosis of PGL, infection and malignancy. Difficulties in diagnosis of Castleman disease and Hodgkin's lymphoma by FNA cytology are recognized.
Keywords
Introduction
Fine-needle aspiration (FNA) cytology is an important diagnostic tool in the investigation of HIV-infected patients with lymphadenopathy. It is a simple, cost-effective, low risk procedure that provides rapid diagnosis. Previous reports show that FNA cytology has an established role in the diagnosis of infection, malignancy and persistent generalized lymphadenopathy (PGL) in HIV-infected patients.1–8
Since the introduction of highly active antiretroviral therapy (HAART) in mid/late-1996, there have been significant changes in the patterns of HIV-associated diseases in populations able to access this therapy.9,10 Of note, the incidence of opportunistic infections has decreased significantly and the decline in Kaposi's sarcoma has been marked. In contrast, a more modest effect on the incidence of AIDS-related malignancy has been observed 11 and the spectrum of HIV-associated malignancy is expanding.12–14
We previously reported our experience of FNA cytology in a cohort of HIV-infected patients over an eight-year period (1989-97), before HAART was universally available. 15 This series showed a high diagnostic yield from FNA cytology and our results were comparable with other contemporaneous series.2–4 We undertook the current study in order to determine whether the changing epidemiology of HIV disease in the era of HAART has affected the diagnostic yield of FNA cytology and also to establish whether FNA cytology continues to have a diagnostic role.
Materials and Methods
The study was undertaken at University College London Hospitals (UCLH) and involved the diagnostic cytopathology service and both the inpatient HIV unit (Patrick Manson Unit and T8) and the outpatient service (Bloomsbury Clinic, Mortimer Market Centre). The UCLH electronic cytopathology database was searched retrospectively for results of FNA cytology procedures performed on HIV-infected patients between January 1998 and December 2006. Results from FNA cytology and other investigations, in patients who subsequently underwent surgical lymph node and other diagnostic biopsy, were also recorded. For each patient, demographic information, HIV risk factor, mode of presentation, CD4 count and HIV viral load were obtained from case-note review and computer records.
FNA cytology was performed in both the outpatient clinic and the inpatient unit using a 23G or 25G needle (capillary method). FNA cytology material was spread directly onto glass slides, initially air-dried and subsequently acetone-fixed. Additional investigations including microbiology, culture and sensitivity, cytochemistry (Ziehl-Neelsen and Grocott) and molecular techniques (polymerase chain reaction) were used where appropriate.
Results
In total, 73 FNA cytology procedures were performed on lymph nodes of 62 HIV-infected patients; nine patients had more than one FNA. Patients’ median age was 38 years (range 23-63); 52 patients were men and 44 were white. Risk factors for HIV acquisition included men who have sex with men (39 patients), heterosexual sex (18 patients), injecting drug use (three patients) and unknown (two patients). The median CD4 count was 260 cells/ μL (inter quartile range [IQR] = 140-440; normal range = 350-1500), and median HIV viral load was 98,000 copies/mL (range from <50 to >500 000). Thirty-eight percent and 31% of FNA cytology procedures were performed in patients who had CD4 counts <200 cells/ μL and a past AIDS-defining illness, respectively. The site of FNA cytology was cervical/supraclavicular (29), axillary (17), inguinal (15) and other (12).
Diagnostic yield from FNA cytology is shown in Table 1. The most common diagnosis was PGL followed by infection and malignancy. Patients with a diagnosis of infection had the lowest median CD4 count (160 cells/ μL [IQR 50-340]) and those with a diagnosis of PGL had the highest median CD4 count (400 cells/ μL [IQR 280-440]).
Diagnosis obtained from 73 fine-needle aspiration (FNA) cytologies of lymph nodes in 62 HIV-infected patients
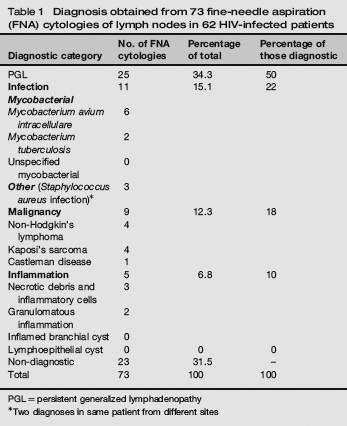
PGL= persistent generalized lymphadenopathy
Two diagnoses in same patient from different sites
Twenty-seven (37%) FNA cytology procedures were performed on patients receiving HAART (Table 2). Among these patients median CD4 count was 290 cells/ μL (IQR 140-470). Fourteen FNA cytology procedures were performed on patients with undetectable HIV viral loads. In the remaining 13 patients, median viral load was 10,200 copies/mL (IQR=847-80,000). Malignancy was more frequently identified among patients receiving HAART when compared with those who were not (26.3% versus 18%).
Diagnosis of 27 fine-needle aspiration (FNA) cytologies from patients receiving highly active antiretroviral therapy
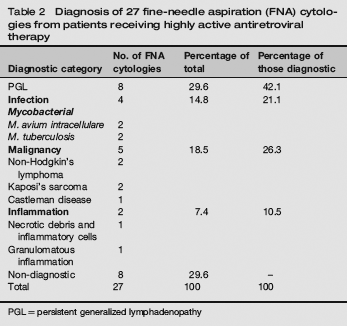
PGL = persistent generalized lymphadenopathy
Open lymph node surgical biopsy was subsequently performed in 20 (27%) patients. The purpose was to confirm a FNA cytology result, to exclude dual pathology or to obtain a diagnosis in reported ‘suspicious’ or technically inadequate FNA samples. Histology of biopsied lymph nodes confirmed the results of cytological diagnosis in seven samples, was discrepant in two and was diagnostic in 11 of the 12 patients with inadequate FNA cytology specimens. Results from open lymph node biopsy are shown in Table 3.
Diagnosis from 20 lymph node biopsies performed in
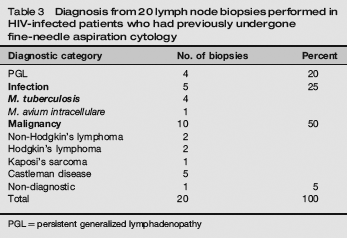
PGL = persistent generalized lymphadenopathy
Of the 23 (31.5%) patients with FNA cytology specimens that were inadequate for cytological assessment, 12 had subsequent lymph node biopsy (see above), nine had no further investigations as lymphadenopathy spontaneously resolved, two had a repeat FNA cytology procedure and two had mycobacterial infection diagnosed from microbiological assessment of the FNA cytology specimen. Three patients with an FNA cytology sample considered as technically inadequate for diagnosis had a diagnosis of malignancy made by subsequent investigation (Table 4).
Comparison of diagnoses from 73 fine-needle aspiration (FNA) cytologies of lymph nodes obtained from 62 HIV-infected patients in present series and from 65 FNA cytologies obtained from 52 HIV-infected patients in the previous series from University College London Hospitals
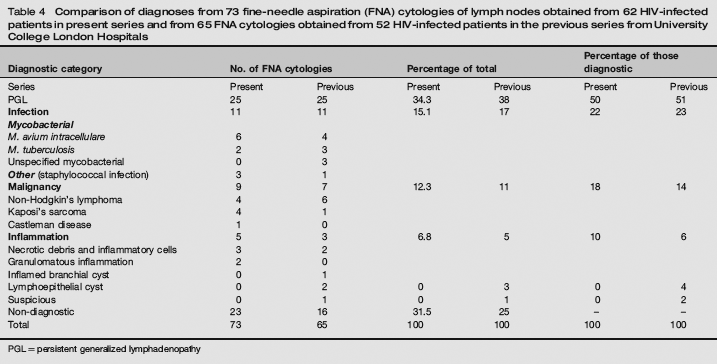
PGL = persistent generalized lymphadenopathy
Seven diagnoses of Castleman disease were made. Of these, six have had ‘inadequate’ FNA cytology; a diagnosis of recurrent Castleman disease was made clinically in one and on open lymph node biopsy in five patients. One case of Castleman disease was diagnosed by FNA cytology. However, this patient had had previously diagnosed Castleman disease with recurrence of symptoms and lymphadenopathy.
Discussion
In this study, the diagnostic yield from FNA cytology of lymph nodes was high, 68.5%. These results are comparable with those from the previous series from this centre (75%) 15 and from other similar studies.1–6 The most common diagnoses were PGL, infection and malignancy. Results in 50% of diagnostic FNA samples provided reassurance of a benign process PGL, obviating the need for further investigation or treatment. Treatment was initiated in cases of specific infection and further investigation, usually open lymph node biopsy, was subsequently performed in patients with ‘inadequate’ and malignant FNA cytology result.
A comparison of the present series with previous published series all of which were undertaken in the pre-HAART era shows a marked decline in the diagnosis of Kaposi's sarcoma (Table 4). In the era of HAART, PGL and mycobacterial infection remain the most common diagnoses made by FNA of HIV-infected patients with lymphadenopathy. The demographics of the patients in both series from this treatment centre are similar, however, in the present study there is an observed difference in the level of immunosuppression (median CD4=260 cells/ μL, compared with 70 cells/ μL, in the previous study.) Fewer FNA tests were performed on patients with CD4 <200 (38% in the present study, versus 61%) and fewer FNA tests were performed on patients with prior AIDS-defining illness (31%, versus 55% in the previous study). Despite these differences, the overall patterns of disease identified by FNA cytology remain similar. Both tuberculosis and PGL can occur at any point in the spectrum of HIV-induced immune dysfunction 16 although infection is usually associated with lower CD4 counts. 10 Mycobacterial infection was the most commonly diagnosed infection in both the previous and current series from this centre.
In contrast with the previous series from this centre no false-positive results and no lymphoepithelial parotid cysts were diagnosed by FNA cytology. Parotid enlargement occurred in ≤ 5% of HIV-infected patients before the availability of HAART. 17 One study reported resolution of lymphoepithelial cysts in patients receiving HAART. 18 There are no data on the changing incidence of lymphoepithelial cysts in the era of HAART; however, wider recognition of this benign condition and its resolution with HAART, suggests that FNA cytology may be required less frequently. However, lymphomatous transformation is a recognized pitfall and, early investigation and treatment are indicated if the lymphoepithelial cyst persists or progresses. 19
It is important to recognize the limitations of this study. First, it ascertained information retrospectively, second, it reflects practice in one specialist HIV treatment centre in central London and thus findings may not be directly extrapolated to other treatment centres, either in UK, or elsewhere, reflecting the geographically variable demographics of HIV-infected patients accessing care and the locale-dependant availability of HAART. Although comparisons have been made between pre- and post-HAART groups in the present study the numbers receiving HAART were small and half of the patients in receipt of HAART did not have undetectable HIV viral loads; a finding that infers poor treatment adherence.
In the present series results from 31.5% of FNA cytologies were ‘inadequate’, thus precluding a diagnosis. Among the HIV-uninfected general population an ‘inadequate’ rate from FNA cytology of 5-15% has been reported. 20 The main explanation for the observed higher rate of ‘inadequate’ FNA cytologies among HIV-infected patients in the present series is sampling error. The success rate of FNA cytology is sampler dependent20,21 and multiple samplers were involved in this large tertiary centre. Technical difficulties related to the size and position of the sampled node have also been described. 22 In the present study, 16% of patients did not have lymphadeno-pathy as a major presenting feature; all of these individuals had ‘inadequate’ FNA cytology. These patients had relatively small lymph nodes making cytological sampling more difficult. Sampling from inguinal lymph nodes had been shown to have the lowest diagnostic yield and, if other sites are accessible, should be avoided. 23 Although modification of FNA cytology procedures in HIV-infected patients was previously suggested as a reason for higher rates of ‘inadequate’ samples, 15 it appears more likely that the spectrum of lymph node pathology has changed in the era of HAART.
PGL involves a spectrum of cytological diagnoses, with disease evolution from early florid follicular hyperplasia to late marked lymphocyte depletion. A paucity of cells on FNA cytology in the latter may be reported as ‘inadequate’. A florid persistent lymph node hyperplasia may appear ‘suspicious’, mimicking a low-grade lymphoma. However, it is important to recognize that lymphomas occurring in HIV-positive patients are more likely to be high-grade B-cell lymphomas and are thus easier to recognize morphologically. They follow an aggressive clinical course. 24
Lymphadenopathy is a common presentation in HIV-infected patients. Careful evaluation is required to determine whether this is indicative of local infection or more serious systemic disease. The wide differential diagnosis provides a diagnostic challenge. The introduction of HAART has not only changed the spectrum of disease but also decreased the mortality associated with the disease, particularly malignancy. 25 Recent epidemiological studies identify higher rates of non-AIDS-defining cancers including Hodgkin's lymphoma. 26 In the present study, two cases of Hodgkin's lymphoma were diagnosed on lymph node excision, after FNA cytology was reported as ‘inadequate’. The application of additional laboratory methods to aid diagnostic interpretation of material obtained by FNA, including clonality analysis and immunophenotyping, maximizes the diagnostic yield and facilitates accurate diagnosis of lymphoid proliferations in these samples.27–29
HIV-associated Castleman disease most commonly encountered in clinical practice is multicentric mixed-variant or hyaline vascular type. Our experience supports the previously recognized difficulties of diagnosing Castleman disease using FNA cytology. 30
In the era of HAART, FNA cytology remains a useful investigation for HIV-infected patients with peripheral lymphadenopathy. Apart from being a useful tool for initial investigation, FNA cytology is particularly useful in diagnosing infection and malignancy. In patients with inadequate samples or inconclusive reports, a repeat FNA cytology procedure or open lymph node biopsy may be required in order to secure a diagnosis.