
Abstract
A survey of consultants in Plymouth Teaching Hospital was performed to identify barriers to HIV testing in secondary care. Testing practices were compared with those recommended by the UK HIV testing guidelines and barriers to testing described.
Keywords
INTRODUCTION
Approximately 28% of the 77,400 individuals living with HIV in the UK at the end of 2007 were unaware of their diagnosis. 1
In order to try to reduce the morbidity, mortality and onward transmission associated with undiagnosed HIV infection, 2,3 strategies have been implemented around the world to increase testing. 4 In the UK, a targeted testing approach has been adopted as described in the HIV testing guidelines published in 2008. 5
Barriers to HIV testing have been described in both patients 6,7 and health-care professionals. 8 This paper attempts to identify some of those barriers among hospital consultants.
METHODS
In May 2009, a postal confidential questionnaire exploring attitudes and knowledge on HIV testing was sent to 185 teaching hospital consultants in Derriford Hospital, a teaching hospital in Plymouth. Radiology, anaesthetic, psychiatric and pathology consultants were excluded. Anonymity was optional. Respondents were asked about HIV testing practices, barriers to testing, awareness of HIV testing guidelines and their opinions about patient views on testing. The questionnaire was sent a second time electronically in an attempt to improve the response rate.
RESULTS
A total of 108/187 (58%) responded. Of those responding, 41/108 (38%) replies came from specialties specifically referred to in the new HIV testing guidelines (TG specialties), 21 (19%) from other medical specialties, 35 (32%) from surgical specialties, five (5%) from obstetrics and gynaecology and five (5%) from paediatricians, one without the specialty named. Sixty-four percent of respondents had performed an HIV test in a patient in the past and of these 42% were from TG specialties.
Eleven out of 108 (10%) described having an opt out policy within their department for a specified patient group and these included patients with TB (1), hepatitis B/C (1), pregnancy (4), primary immunodeficiency (1) and for those undergoing haemodialysis or involved in transplantation (4).
Fifteen out of 23 (65%) respondents from specialties where opt out testing is recommended by the HIV testing guidelines said they had no/were unaware of any opt out policy in their department.
An HIV risk assessment was done in all patients by 3/108 (3%) respondents and in some patients by 57 (53%) respondents. Criteria used for selecting patients in whom they needed to do a risk assessment included medical diagnosis alone (40%) and medical diagnosis and risk group (47%).
Overall, 80/108 (74%) respondents could list a medical condition associated with HIV and of the 41 respondents from the TG specialties, 10/41 (25%) could list all the target medical conditions in the guidelines. Seven out of eight respondents from emergency medicine came up with a selection of diagnoses, but none included seroconversion.
Only eight out of 108 (7.4%) respondents were aware of the HIV testing guidelines; 4/8 knew how they applied to their specialty.
Thirty-three out of 108 (31%) said there were obstacles to HIV testing within their practice, see Figures 1 and 2.
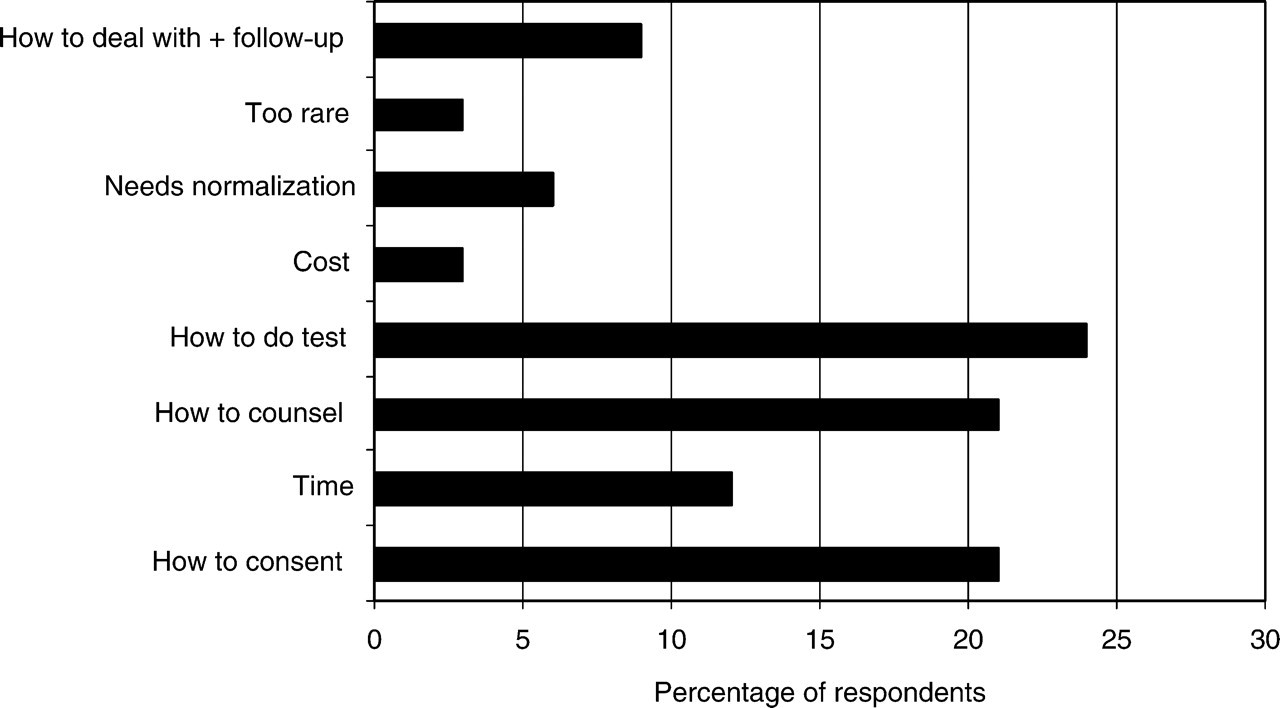
Perceived obstacles to HIV testing
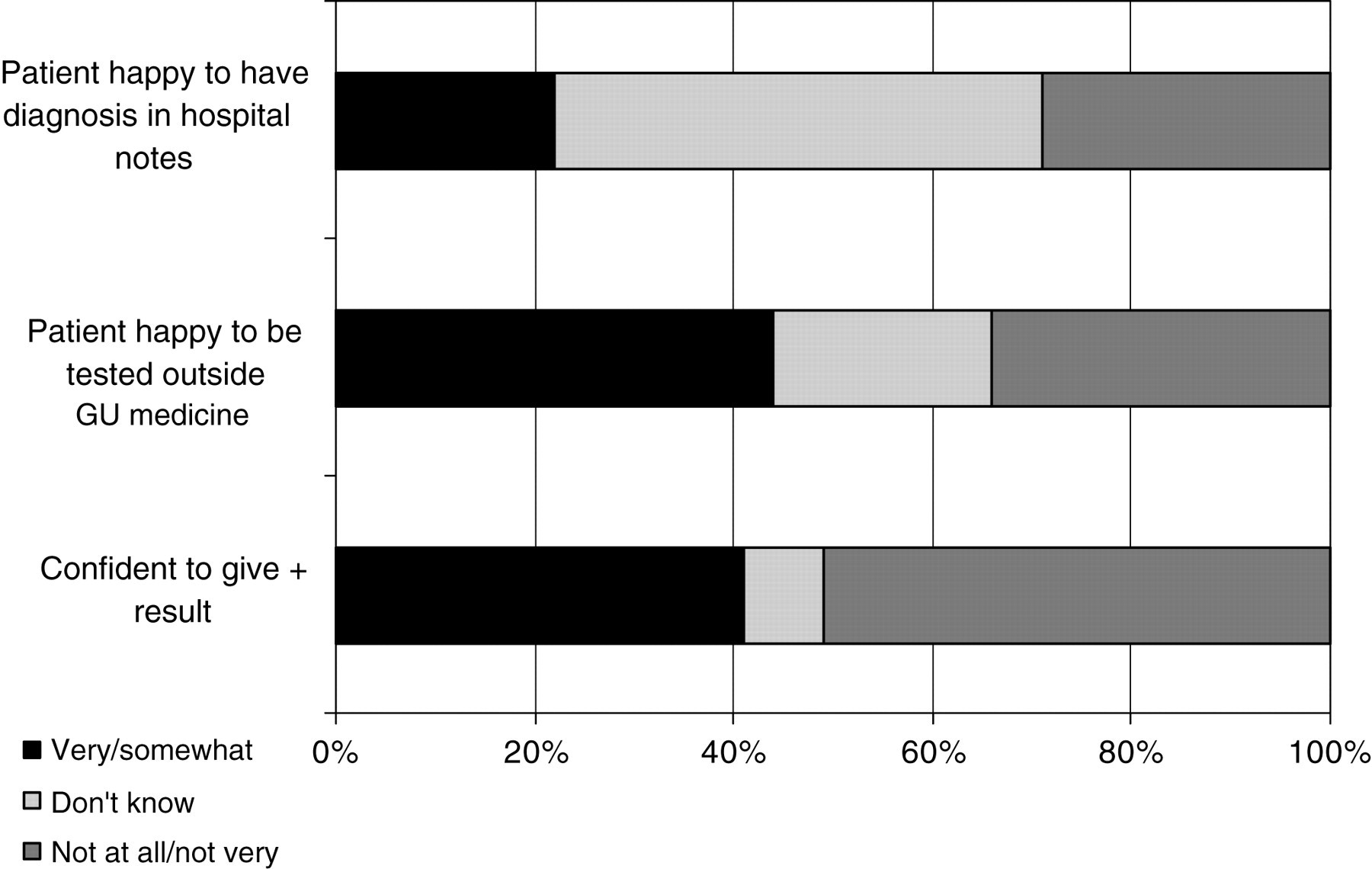
Consultant views on testing outside sexual health services. GU = genitourinary
However, 77% (83/108) felt it was always useful to their practice to know if a patient is HIV positive and 19% (21/108) felt it was useful in some cases.
DISCUSSION
Diagnosing the undiagnosed remains a huge challenge requiring urgent attention. 9 Much work has been done around patient barriers to testing; often, however, it is the medical profession which fails to diagnose patients when we have the opportunity. 10 The majority of patients in secondary care are happy to be tested (Dr Neale, South West HIV Association meeting, May 2009).
We must ensure that health-care professionals are not the cause of any barriers to testing. Education should target identified barriers and systems should be in place to eliminate obstacles to testing outside of sexual health services. We need to empower our colleagues to ensure they see the diagnosis of HIV as much their remit as ours.