
Abstract
To describe the frequency, risk factors, and clinical signs and symptoms associated with hepatotoxicity (HT) in patients on nevirapine- or efavirenz-based antiretroviral therapy (ART), we conducted a retrospective cohort analysis of patients attending the ART clinic in Kibera, Kenya, from April 2003 to December 2006 and in Mavalane, Mozambique, from December 2002 to March 2007. Data were collected on 5832 HIV-positive individuals who had initiated nevirapine- or efavirenz-based ART. Median baseline CD4+ count was 125 cells/μL (interquartile range [IQR] 55–196). Over a median follow-up time of 426 (IQR 147–693) days, 124 (2.4%) patients developed HT. Forty-one (54.7%) of 75 patients with grade 3 HT compared with 21 (80.8%) of 26 with grade 4 had associated clinical signs or symptoms (P = 0.018). Four (5.7%) of 124 patients with HT died in the first six months compared with 271 (5.3%) of 5159 patients who did not develop HT (P = 0.315). The proportion of patients developing HT was low and HT was not associated with increased mortality. Clinical signs and symptoms identified 50% of grade 3 HT and most cases of grade 4 HT. This suggests that in settings where alanine aminotransferase measurement is not feasible, nevirapine- and efavirenz-based ART may be given safely without laboratory monitoring.
INTRODUCTION
The majority of antiretroviral therapy (ART) programmes in sub-Saharan African countries are scaling up first-line ART using fixed dose antiretroviral regimens containing stavudine (d4T), lamivudine (3TC) and nevirapine (NVP). 1,2 In HIV-positive patients with tuberculosis (TB), efavirenz (EFV) replaces NVP. One of the primary concerns with these regimens is hepatotoxicity (HT) associated with NVP. 3–10 In a meta-analysis of controlled clinical trials, the risk of HT associated with NVP was 10%. 7 In a trial conducted in South Africa, this was as high as 17%. 6 In resource-rich countries, screening for HT during ART has been primarily based on serum alanine aminotransferase (ALT) levels, a liver enzyme that serves as a ‘proxy’ for liver inflammation and damage. HT is graded into four categories (grades 1–4) and severe HT implies grade 3 and grade 4 toxicity. Grade 3 toxicity is defined as an ALT >5 times the upper limit of the normal range (ULN) and grade 4 HT as an ALT >10 times the ULN. 11 Clinical guidelines recommend discontinuation of NVP or EFV at grade 3 or 4 HT. 12 The correlation of NVP-related HT with clinical symptoms remains poorly documented and ranges from 2% to 17% in the literature. 13
ALT testing requires laboratory technology that is sophisticated and expensive and therefore not routinely available at the health centre level in most resource-poor settings. In order that ALT testing does not act as a barrier to scaling up ART in such settings, World Health Organization (WHO) guidelines do not insist on ALT monitoring as a prerequisite to offering ART at the primary care level. 1 This, however, is in contrast to manufacturer guidelines that recommend vigilant ALT monitoring for NVP users for the first 18 weeks, and regular monitoring thereafter while on treatment. 3 Clinical trials support routine monitoring in the first 12 weeks 6,14,15 but it is unknown if routine ALT testing prevents morbidity or mortality in routine programme settings. Risk factors for HT in resource-constrained settings in sub-Saharan Africa are not well described.
This cohort study of adults commenced on first-line NVP- or EFV-containing ART regimens under programmatic conditions in Mozambique and Kenya describes the frequency of HT, examines possible risk factors associated with HT, and describes the relationship between elevated ALT levels and clinical symptoms and signs.
METHODS
Study setting and population
This study included patients from Mavalane, Mozambique, and Kibera, Kenya, where ART has been provided by Médecins Sans Frontières (MSF) since 2002 and 2003, respectively, in collaboration with the Ministries of Health. All patients are started on either NVP- or EFV-based triple therapy according to WHO guidelines for the provision of ART in resource-limited settings. The majority of patients were given the nucleoside backbone of d4T plus 3TC. Patients who had at least one follow-up visit and initiated ART in Kibera, Kenya, from April 2003 to December 2006 and in Mavalane, Mozambique, from December 2002 to March 2007 were included. Women who had previously received single or dual NVP-based therapy via the prevention of mother-to-child transmission (PMTCT) programme were also included. Treatment-experienced patients and children were excluded.
ALT measurements and HT
ALT testing was systematically offered to all patients at baseline, two weeks, four weeks, then every six months, and when clinically indicated. Laboratory testing was performed by the respective hospital laboratories with quality control ensured by MSF. ALT assays were conducted using a spectrophotometer following standard operating procedures. Clinical symptoms and signs consistent with hepatitis were nausea, vomiting, abdominal pain and/or jaundice. Serum ALT (units/litre) was graded using criteria established by the AIDS Clinical Trial Group 11 as follows: grade 0 = <1.25 × ULN; grade 1 = 1.25–2.5 × ULN; grade 2 = 2.6–5.0 × ULN; grade 3 = 5.1–10 × ULN; grade 4 = >10 × ULN. HT was defined as grade 2 ALT with associated clinical symptoms, or grade 3 or 4 ALT. Severe HT was defined as grade 3 or 4 ALT. HT was managed according to national and WHO guidelines, which recommend that NVP or EFV be substituted or stopped when grade 3 or 4 ALT or grade 2 ALT with clinical symptoms ensue.
Statistical analysis
Baseline characteristics and ART outcomes for all patients initiated on NVP- or EFV-based ART were exported from an electronic database maintained prospectively for routine monitoring and evaluation. Patients who stopped or substituted NVP or EFV because of potential HT were identified using this database and HT confirmed through chart review. Mortality was evaluated up to six months after initiation of ART since those occurring later were unlikely to be attributed to HT. Data were analysed using Stata (Version 10, College Station, TX, USA). Time from treatment initiation to HT event was estimated using the Kaplan–Meier method. Cox proportional hazards regression analysis was used to determine risk associated with HT. Logistical regression was used to determine risk factors for clinical signs and symptoms. Variables considered in the analyses included age, gender, baseline CD4 cell count, type of non-nucleoside reverse transcriptase inhibitor (NNRTI) (NVP or EFV), and programme site. The chi-squared test was used for determining the relationships between HT and mortality and to compare the association of grade of HT with clinical grades 3 and 4 HT. All available variables were included a priori in multivariate models. All tests and confidence intervals were considered to be significant at a P ≤ 0.05 (two-sided).
Ethics
The HIV/AIDS programmes in the two countries have been formally approved by the respective Ministries of Health. The procedures for selection and inclusion of patients within the ART programme follow WHO and national guidelines. General measures are provided to ensure patient confidentiality, consent for HIV testing, and counselling and support for those who receive a positive HIV test result. ART and all laboratory testing services (including ALT) are offered free of charge within the two projects. Ethical approval was given by an independent Ethics Review Board that screens research proposals by MSF.
RESULTS
Characteristics of the study population
Baseline characteristics and outcomes of patients on nevirapine- and efavirenz-based antiretroviral therapy
Continuous variables are given as median (interquartile range). Ordinal and discrete variables are given as n (%). WHO = World Health Organization; NVP = nevirapine; EFV = efavirenz; ART = antiretroviral therapy; LTFU = lost to follow-up; BMI = body mass index; HT = hepatotoxicity
Hepatotoxicity
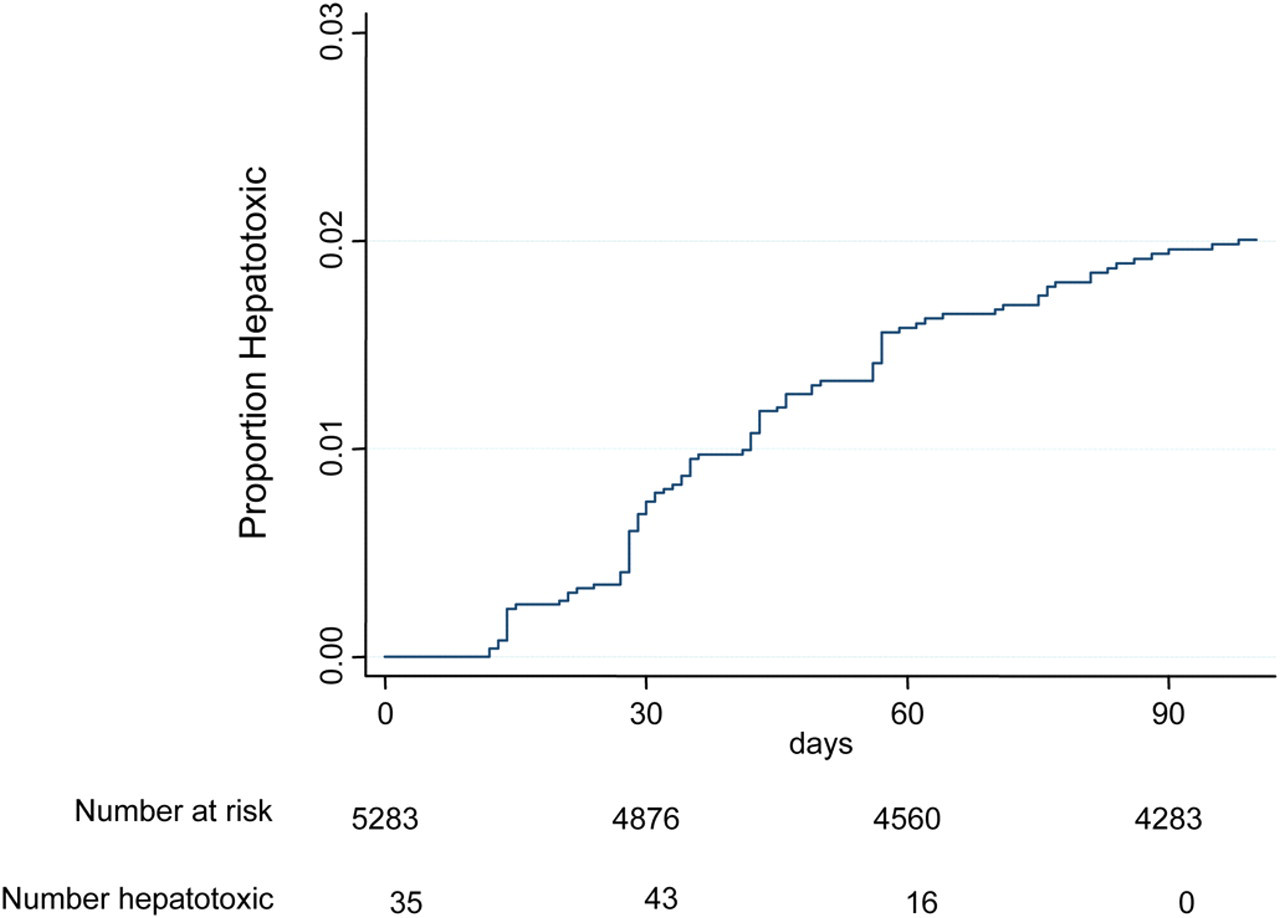
Overall, one hundred and twenty-four (2.4%) patients developed HT while on NVP- or EFV-based ART. This rate was similar if only women starting ART at CD4>250 cells/μL were considered: 12 HT events among 409 women (2.9%). Median time to HT was 43 days (IQR, 28–81) in the Kenya cohort and 46 days (IQR, 29–110) in the Mozambique cohort. Eleven (0.2%) individuals had grade 2 HT, 83 (1.5%) had grade 3 HT and 30 (0.5%) had grade 4 HT. Of 20 men starting ART with a CD4 > 400/μL, only one (5%) developed HT. Times to HT are shown in Figures 1 and 2. Ninety-four (76%) episodes of HT occurred in the first three months on ART. Of patients with HT, 111 (89.5%) had data on associated clinical symptoms available and 72 of these (64.8%) were clinically symptomatic (Table 2). On multivariate analysis, age, gender, type of NNRTI, baseline CD4 count and programme site were not associated with HT or clinical symptoms (Tables 2 and 3). All (100%) patients with grade 2 HT had clinical symptoms. Forty-one (54.7%) of patients with grade 3 (n = 75) and 21 (80.8%) of patients with grade 4 HT (n = 26) had associated clinical signs or symptoms (P = 0.018). On multivariate analysis, grade 4 HT (compared with grade 3 HT) was found to be independently associated with clinical symptoms (odds ratio [OR] = 3.72, 95% CI 1.16–10.39, P = 0.023). Four (5.7%) of 124 patients with HT died in the first six months compared with 271 (5.3%) of 5159 patients who did not develop HT (P = 0.315). After adjusting for gender, age, CD4 count, ART drug and clinic location, HT was not found to be a risk factor for mortality (hazard ratio [HR] = 0.53, 95% CI 0.20–1.42, P = 0.205) (Table 4).
Time to hepatotoxicity on nevirapine- or efavirenz-based antiretroviral therapy Time to early hepatotoxicity on nevirapine- or efavirenz-based antiretroviral therapy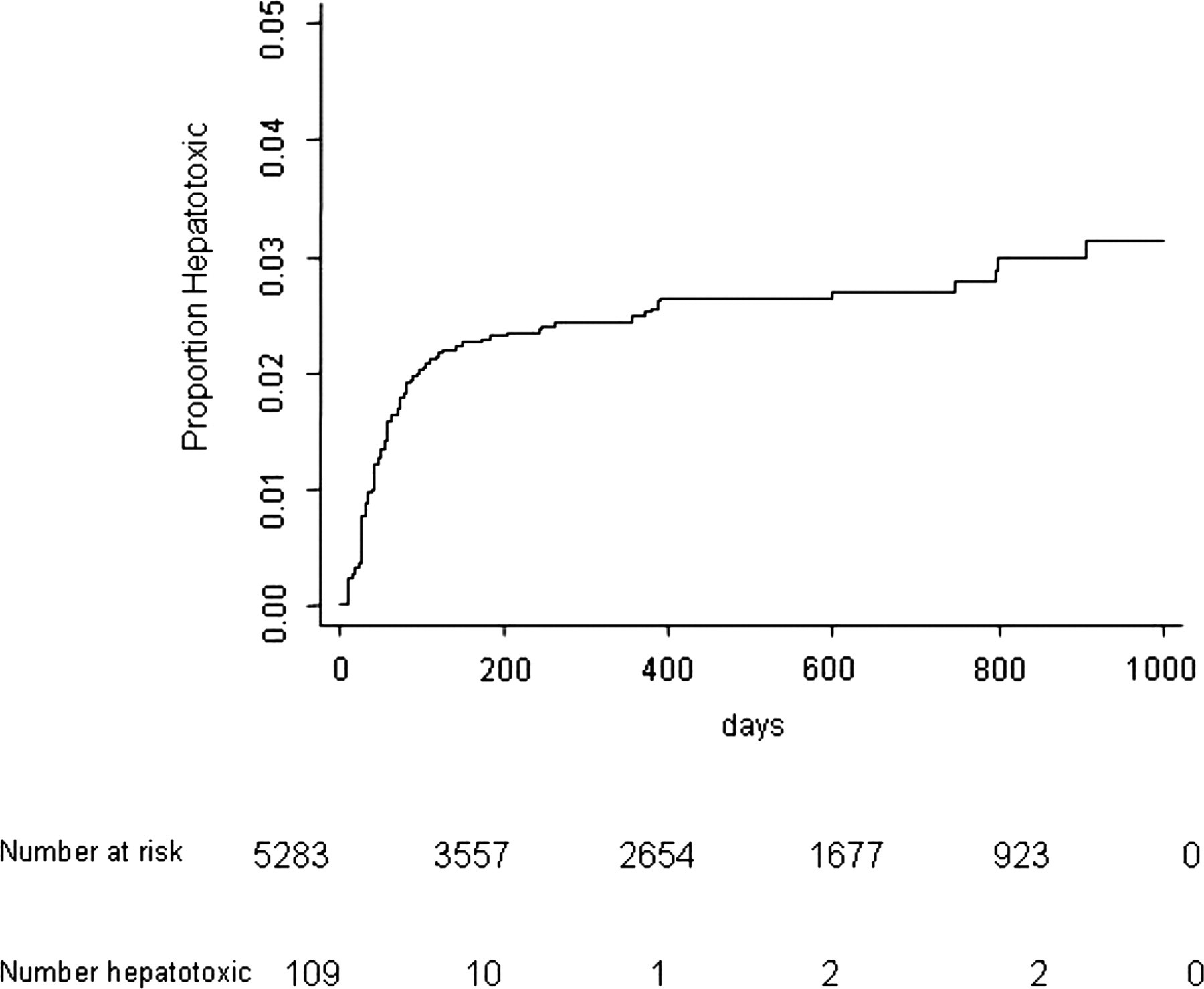
Adjusted associations between patient characteristics and hepatotoxicity
HR = hazards ratio; NVP = nevirapine; EFV = efavirenz; HT = hepatotoxicity; CI = confidence interval; ART = antiretroviral therapy
*Adjusted for all variables
Adjusted associations between patient characteristics and clinical symptoms and signs of hepatotoxicity
OR=odds ratio; NVP=nevirapine; EFV=efavirenz; HT=hepatotoxicity; ART = antiretroviral therapy; CI = confidence interval
*Adjusted for all variables
Adjusted associations between patient characteristics and mortality
HR = hazards ratio; NVP = nevirapine; EFV = efavirenz; HT=hepatotoxicity; CI = confidence interval; ART = antiretroviral therapy
*Six-month mortality
DISCUSSION
In this study the proportion of patients developing HT was low and not associated with increased mortality. Median time to HT was approximately six weeks. Clinical signs and symptoms alone identified half of grade 3 toxicity and most cases of grade 4 HT. This suggests that in settings where ALT measurements are not possible, NVP- and EFV-based ART might be given safely without laboratory monitoring.
In our setting, 2.4% of patients discontinued ART due to HT. Reports in the literature of NVP-associated HT have ranged from 2% to 18% with variable definitions of HT including asymptomatic ALT elevation, clinical symptoms consistent with hepatitis or a combination of both. 6,16 Few studies have reported on the frequency of discontinuation of ART due to HT in routine programmatic settings. In Thailand, 2% of patients on NVP-based ART and 0.5% of patients on EFV-based ART discontinued therapy due to HT. 17 In an MSF multi-centre observational cohort, 11 (1.6%) of 655 discontinued NVP-based ART due to HT. 18 While it has been recommended to stop NVP when asymptomatic grade 3 or 4 ALT elevation occurs, 4,12 morbidity and mortality associated with isolated liver enzyme elevations are not well established. NVP manufacturer inserts recommend ‘routine ALT testing until 18 weeks’ 4 but resource-constrained settings are challenged to do so given the limited availability of laboratory monitoring.
Defining risk factors for HT allows for selective ALT monitoring for higher risk patients where routine ALT monitoring is unavailable or prohibitively expensive. Conflicting data on the association of baseline CD4 count and HT have been reported. In some studies, higher baseline CD4 counts (>400 cells/μL for men and >250 cells/μL for women) have been associated with a greater risk for NVP-based HT; 19 other studies did not demonstrate such an association. 20,21 Considering our median CD4 count (125 cells/μL) was low we could not assess the risk of HT accurately for those with high baseline CD4 counts. One study found a marginal association between low baseline CD4 count (<100 cells/μL) and risk of HT among patients on an EFV-based regimen 22 but we did not find such an association.
The correlation of clinical symptoms with ALT elevation has not been well documented. In our study, the majority of patients with severe HT had clinical signs or symptoms. This suggests that grade 3 or 4 ALT alone without clinical symptoms may not necessarily require immediate drug substitution. In a meta-analysis of Boehringer Ingelheim-sponsored clinical trials, 125 subjects continued NVP despite developing severe (grades 3 and 4) HT and patients remained clinically asymptomatic and resolved their ALT abnormalities without morbidity. 7 In our study, HT was not associated with increased mortality. Therefore, if clinical symptoms can be correlated with HT in the most severe cases, and if drug-associated HT is not associated with increased mortality, then routine ALT monitoring may not be necessary. In Uganda, where ALT monitoring was unavailable, HT was reported in 0.5% of patients and the cause of death in only one of 992 patients on NVP-based ART. 2
This study has a number of limitations. The main limitation was potential underreporting of HT. While both programmes in Kenya and Mozambique had standard ALT monitoring, it is unknown how well these were enforced. From a study in South Africa, we demonstrated that few patients were monitored according to protocol in the resource-constrained setting. 23 HT detection will be greater the more frequently ALT is monitored: in South Africa, patients who had ALT measured at baseline, four weeks, eight weeks and 12 weeks were more likely to develop HT during the first three months compared with those who had ALT measured less frequently. 23 We also do not know if patients who died or were lost to follow up had HT and if so, whether this would have changed the findings. Given that, on average, losses occurred among patients who had been on treatment for six months, we consider it unlikely that these would have been due to severe hepatotoxic events. Another limitation is lack of data on associated risk factors for HT: alcohol use, concurrent TB treatment and hepatitis co-infection were not measured in these routine programmes 5,7 However, even though hepatitis co-infection rates are likely around 10%, 24–26 HT remained low in this study suggesting co-infection may not be a contraindication to starting NVP- or EFV-based ART. One study reported low body mass index as a risk factor for HT; 6 this could not be assessed in our study as height was not routinely recorded. Most patients were on ART that also included stavudine (d4T), which may have been a contributor to late HT. This effect was not measured in our study.
Nonetheless, we believe our findings have important public health implications regarding HT and the use of ART. First, HT associated with NVP- or EFV-based ART is rare in these programmatic settings; second, clinical symptoms are usually associated with severe HT; finally, HT was not associated with increased mortality. ALT monitoring is a barrier to scale-up of ART in resource-limited settings in sub-Saharan Africa; these data suggest that clinical rather than ALT monitoring might be sufficient. Prospective studies are warranted to confirm our findings, particularly for patients initiating NVP-based ART at higher CD4 counts.
Footnotes
ACKNOWLEDGEMENTS
Author contributions: KC was responsible for the overall design, analysis and writing of the paper. RZ, FR and MB wrote the first draft of the study protocol, which was reviewed by KC, MM and IZ contributed to the data collection. NF and RZ contributed to the concept, intellectual content and writing of the paper. The final version of the manuscript was seen and approved by all authors. The corresponding author held the final responsibility for submitting the manuscript for publication. The authors would like to thank the MSF field teams in Kibera, Kenya and Mavalane, Mozambique for their excellent clinical care of the patients in this study. Sources of Support: Médecins Sans Frontières, Brussels.