
Abstract
Primary HIV infection normally shows an asymptomatic presentation or symptoms resembling infectious mononucleosis. However, severe unusual presentations have been reported. We report a case of acute ventricular fibrillation during primary HIV infection. Moreover, the rapid development of symptoms, the profound pancytopaenia and the marked elevation of liver enzymes make this case rather unique. Therefore, acute ventricular fibrillation should be added to the list of complications of primary HIV infection.
Cardiac involvement is relatively common in patients with AIDS and may lead to an increased incidence of unexpected and sudden cardiac death. 1,2 Therefore, careful cardiological evaluation has been recommended in HIV-positive patients. However, most previous studies have reported impairments in cardiac systolic function, whereas malignant arrhythmias have not yet been reported in patients with HIV infection. We report a case of a woman with sudden ventricular fibrillation during primary HIV infection.
CASE REPORT
A 22-year-old woman presented to our emergency room with a nine-day history of fever, chills, headache, vomiting and diarrhoea. Seven days before admission, she had returned form a holiday trip to Spain. Her past medical history was unremarkable and she was not taking any prescription medication. On examination, the patient was acutely ill with a body temperature of 38.3°C, and a blood pressure of 100/60 mmHg. Other vital signs were normal. There was bilateral cervical lymphadenopathy, the oropharynx was erythematous with tonsillar enlargement, neck flexion caused discomfort and mild abdominal tenderness was detected. The remainder of the examination was normal. The patient's WBC was 2.8 (normal value >4×109/L), platelets were 96 (normal value >150×109/L), creatine was 150 (normal value <106 µmol/L), C-reactive protein was 12.8 (normal value <10 nmol/L), aspartate aminotransferase and alanine aminotransferase levels were 292 and 178, respectively (normal value for each <32 U/L), creatinine kinase value was 312 (normal value <149 U/L) and creatine kinase-muscle-brain (CK-MB) level was 31 (normal value <24 U/L). Moreover, an HIV-1/2 enzyme immunoassay (EIA; BioRad, Marnes la Coquette, France) was negative, as were serological tests for hepatitis A, B and C and H1N1 influenza.
The patient was transferred to the intensive care unit under the working diagnosis of an infection of unknown cause with multiorgan involvement. She received intravenous electrolyte and fluid solutions and amoxicillin-clavulanate as an antibiotic (only for 1 day). An ultrasonogram of the abdomen detected splenomegaly, whereas a lumbar puncture, a transthoracic echocardiogram, an electroencephalogram, an electrocardiogram (ECG) and a chest X-ray presented normal findings. On day 2 after admission, WBC and platelets dropped to 1.9×109/L (0.64×109/L segmented neutrophils) and 47×109/L, respectively. Therefore, a bone marrow aspirate was performed, which revealed an infection-induced pancytopaenia, but no signs of leukaemia. Repeated blood and urine cultures remained sterile. Testing for antibodies against cytomegalovirus, herpes simplex virus, Epstein–Barr virus, toxoplasmosis, chlamydia, leptospira, leishmania, entero-, adeno- and parvo-virus B19 revealed no evidence for acute infections with these pathogens.
By day 4, her symptoms eased and laboratory findings returned to normal (except for liver enzymes) and her WBC. Subsequently, the patient was transferred to a regular ward. On day 6, the HIV was 3.4×109/L EIA was repeated and had become positive, while the Western blot was still negative. On the morning of day 7, the patient reported no complaints except for vomiting the previous day. However, at noon she was found unconscious with inadequate breathing and a weak pulse, and advanced cardiac life support was started. ECG monitoring detected ventricular fibrillation and three rounds of defibrillation plus 300 mg of amiodarone intravenously was needed before sinus rhythm could be restored. Moreover, high doses of catecholamines were required to stabilize blood pressure, and on echocardiogram severe global systolic dysfunction with a left ventricular ejection fraction of 20% was seen. Laboratory findings included elevated troponin T values up 1.8 µg/L (normal value < 0.04 µg/L) and a reduced serum potassium of 3.0 mmol/L (normal value 3.5–5 mmol/L). After 24 hours on mechanical ventilation, the patient was extubated, global systolic function returned to normal, catecholamine infusions were stopped and no focal neurological deficit was detectable. Of note, three days later cardiac magnetic resonance imaging revealed an epicardial pattern of abnormal patchy myocardial delayed enhancement, which is highly indicative of myocarditis (Figure 1).
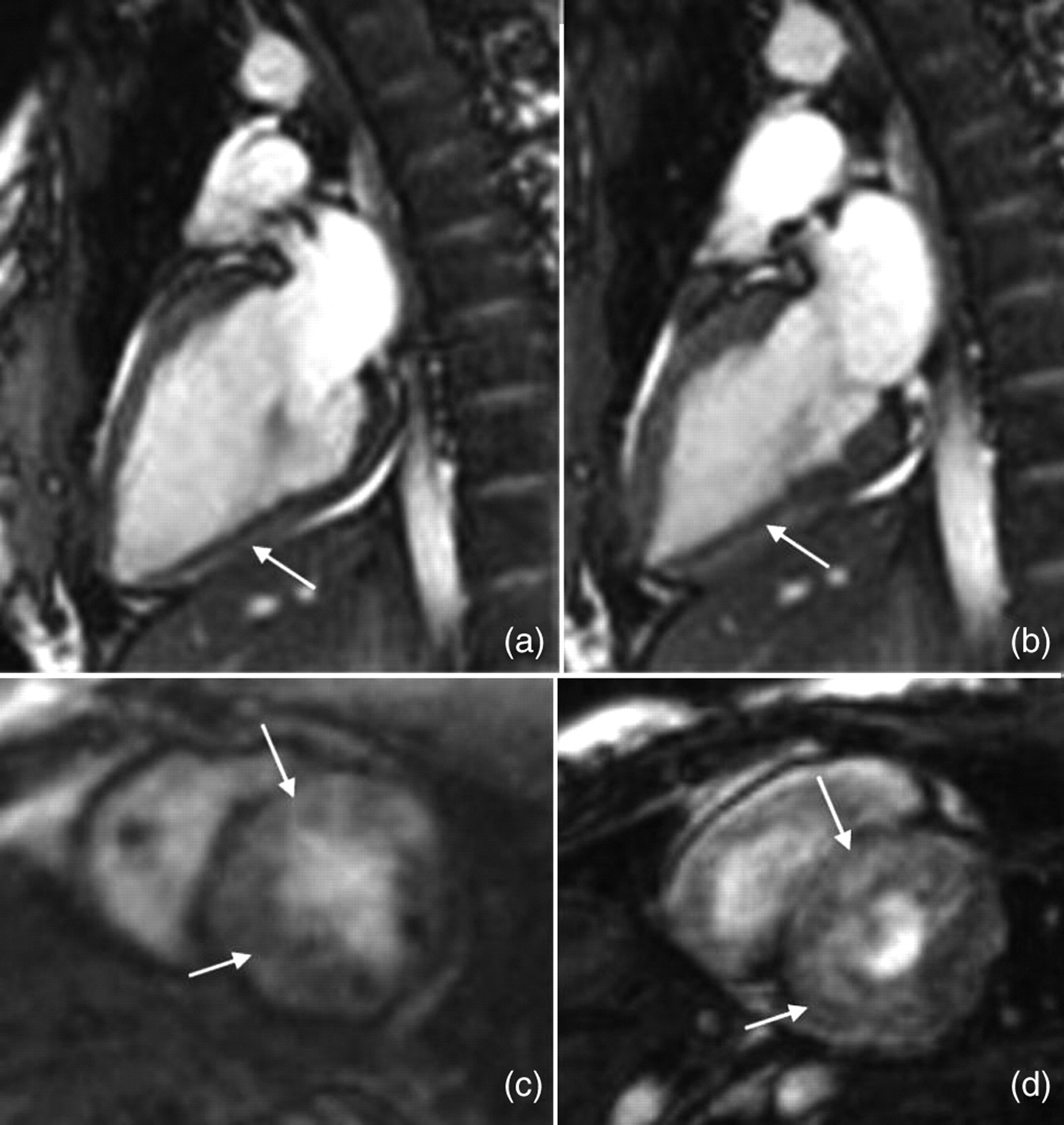
Cardio magnetic resonance imaging demonstrating myocarditis: (a, b) shows Cine-TRUFI sequences in vertical long axis. (a) presents the end-diastolic and (b) the end-systolic phase. The arrows point at stiffness and lower contractility corresponding to hypokinesia of the posterior myocardial wall. (c, d) Shows short axis of late enhancement sequences 10 minutes after application of gadolinium contrast media. The arrows point at spotted intra-myocardial contrast enhancement, which can be caused by inflammation and possibly resultant fibrosis
On day 10, primary HIV infection was confirmed by polymerase chain reaction with an HIV-1 RNA of 1.8 million copies per mL and a CD4+ count of 318 cells/mm3. When the patient was informed about the diagnosis, she revealed that she had unprotected sexual intercourse 14 days earlier. After initiating antiretroviral treatment with efavirenz, emtricitabine and tenofovir disoproxil fumarate, the patient's condition improved further; her liver function, troponin-T levels and WBC normalized and the patient was discharged from hospital. For cardio-protection she received a Life Vest defibrillation system (CORIZON GmbH, Kerpen, Germany) for four weeks. In the meantime no further arrhythmic events occurred; her transthoracic echocardiogram, ECG, troponin-T and potassium levels remained normal.
To our knowledge, this is the first report of acute ventricular fibrillation during primary HIV infection. Moreover, the rapid development of symptoms, the profound pancytopaenia and the marked elevation of liver enzymes make this case rather unique. However, similar severe manifestations have been reported in the literature. For example, Tattevin et al. 3 reported of a 16-year-old girl with acute liver failure during primary HIV infection. Nonetheless, ventricular fibrillation may be added to the list of severe manifestations of primary HIV infection.