
Abstract
Although several antiretroviral agents are available, realistic options for initial therapy remain limited, as many are not licensed for treatment-naive patients, as reflected in national and international guidelines. A variety of factors influence treatment choice. From the physicians’ perspective, it is important to consider age, sex, co-morbid conditions, concomitant drugs and potential for adherence. Meanwhile, patients are concerned about the impact of side-effects on their day-to-day life and long-term future, drug efficacy, future options and time available in clinics. Patients’ concerns may be alleviated by detailed discussion throughout treatment, including the importance of adherence, the pros and cons of different treatments and potential side-effects. Positive outcomes in terms of not just viral load and CD4 counts but also improved duration and quality of life should be emphasized. Treatment must be tailored to each patient to maximize benefits and minimize risks.
Introduction
Several agents have become available since the licensing of the first antiretroviral more than 20 years ago. However, options for initial therapy are still limited, as some of the drugs are not yet licensed or used widely in treatment-naive patients. Moreover, old and emerging toxicities and interactions between antiretroviral drugs and/or other concomitant medications further limit the number of combinations we can offer in routine practice.
Guidelines
In the past few years, the antiretroviral options recommended in guidelines have actually narrowed, with thymidine analogues demoted from preferred to alternative status because of their association with lipoatrophy and other toxicities in the medium to long term. The International AIDS Society-USA Panel (IAS-USA) recommends two nucleosides plus a non-boosted protease inhibitor (PI) (efavirenz) or boosted PI as initial therapy. 1 The British HIV Association (BHIVA) expresses a preference for efavirenz over boosted PI and recommends a backbone of emtricitabine plus tenofovir disoproxil fumarate or abacavir plus lamivudine, with the caveat that abacavir should be avoided in patients with a significant background risk for cardiovascular disease (CVD) or a high baseline viral load due to data that have emerged over the last year. 2 The European AIDS Clinical Society (EACS) guidelines have a slightly broader spectrum of preferred agents, recommending efavirenz, nevirapine and a choice of three boosted PIs (amprenavir/ritonavir, lopinavir/ritonavir and saquinavir/ritonavir). 3 Abacavir plus lamivudine and emtricitabine plus tenofovir disoproxil fumarate are the fixed-dose combination backbones recommended by the EACS.
Although guidelines are crucial, their recommendations may not always be the best approach for every patient. Indeed, the guidelines themselves highlight the need for individualization of treatment:
‘HAART regimens always need to be individualized for the patient in order to achieve the maximum potency, durability, adherence and tolerability and to avoid long-term toxicities and any likely drug interactions’.
2
‘The initial regimen must be individualized, particularly in the presence of comorbid conditions’.
1
Treatment Patterns
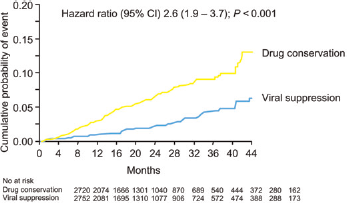
Irrespective of the starting regimen, patients are likely to be on treatment for longer than ever before, as a number of cohort analyses and sub-analyses of the Strategies for Management of Antiretroviral Therapy (SMART) subset have shown that patients who start treatment earlier, on the whole, have better treatment outcomes (Figure 1).
4
The SMART data also show that patients who interrupt therapy have not only more HIV-related problems but also higher rates of non-HIV-associated morbidity and mortality.
4
Therefore, not only are patients starting earlier, they are much less likely to interrupt highly active antiretroviral therapy (HAART) in the long term.
Strategies for Management of Antiretroviral Therapy study: opportunistic disease or death from any cause in those with continuous versus episodic use of antiretroviral therapy. Reproduced with kind permission from El-Sadr et al.
4
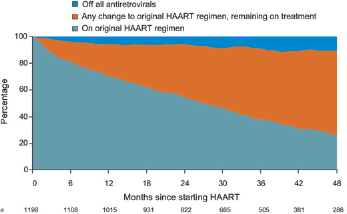
Nevertheless, a significant proportion of patients do stay on their first combination in the long term. Although the data shown in Figure 2 were published a few years ago and some of the regimens may be less tolerable than those currently used for initial therapy, they indicate that most patients switch their combination within four years for a variety of reasons.
5
Along with data from other cohort analyses, the results suggest that most switches are driven not by virological failure but by toxicity and dosing simplification.6,7
Percentage of patients on original highly active antiretroviral therapy (HAART) regimen with any change to original HAART regimen remaining on treatment and off HAART. Reproduced with kind permission from Mocroft et al.
5
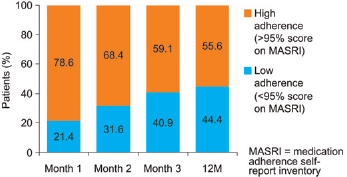
Adherence tends to wane over time. Indeed, in one study, more than 40% of patients self-reported low adherence (<95%) by 12 months (Figure 3).
6
This emphasizes the importance not only of discussing adherence at the baseline visit but also of reinforcing adherence messages throughout a patient's long-term care.
Adherence to highly active antiretroviral therapy over 12 months. Reproduced with kind permission from Home et al.
6
Factors Affecting Treatment Selection
Physicians’ perspective
To minimize adherence difficulties and optimize treatment outcomes, physicians base their treatment choice on a variety of patient-based factors. 1 ‘2 Many countries now perform baseline resistance testing to help guide treatment choices. Co-morbidities need to be considered, as do any concomitant medications that the patient may be on at the time of starting treatment or may be likely to need in the future. Age and sex are also important considerations: treatment choice may be different, for example, in women of child-bearing age. If patients are considered at risk of poor adherence, the physician is more likely to choose a combination that is less ‘fragile’ from a genetic point of view. Studies show, however, that physicians are very poor at predicting adherence, and more specific tools to maximize treatment choices are perhaps needed both initially and during long-term follow-up.
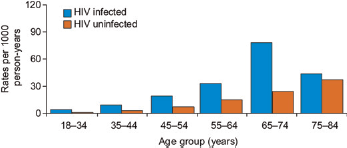
CVD has been a hot topic over the past year as a result of emerging data, and the fact that it is the main cause of death worldwide automatically positions it high on the list of factors to be considered. In an analysis that compared 3851 HIV-infected with 1,044,589 HlV-uninfected individuals, data were adjusted for cardiovascular risk factors such as age, lipid levels and, where possible, smoking.
7
Across the age spectrum, HIV-infected individuals had higher rates of myocardial infarction than their uninfected counterparts (Figure 4). Current assessment of cardiovascular risk is probably much better than previously, perhaps as a result of the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) analysis. At the HIV clinic at Chelsea and Westminster Hospital, more and more tools such as the Framingham equation are being used to estimate cardiovascular risk.
Rate of acute myocardial infarction per 1000 person-years in 3851 HIV-infected and 1,044,589 HlV-uninfected patients, 1996-2004. Reproduced with kind permission from Triant et al.
7
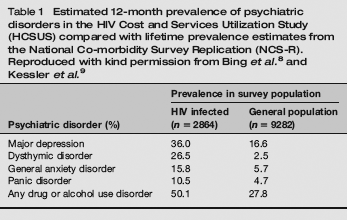
A study of more than 750 patients across five clinics in the UK found that 31% of patients reported some degree of suicidal thinking in the previous seven days. 10 For most of these patients, suicidal thoughts were infrequent or rare; however, for a small proportion such thoughts were frequent or even constant. This study also investigated factors that were significantly associated with suicidal thoughts; in common with results in late presenters, patients were more likely to be heterosexual and of black ethnic origin. A lack of disclosure of HIV status was also significantly associated with suicidal thoughts. Physicians could perhaps reduce the proportion of patients so affected by providing additional services and addressing disclosure issues with patients. As is the case with adherence, psychological morbidity is often discussed initially, but the messages are not always reinforced in the long term. Finally, and perhaps not surprisingly, physical symptoms were clearly associated with suicidal thoughts. 10 Starting treatment at the right time and managing symptoms and side-effects should at least partly alleviate these issues.
Patients’ perspective
Many patients’ concerns overlap with physicians’ but with a slightly different perspective. In terms of side-effects, for example, physicians may be concerned about the ratio of low-density lipoprotein cholesterol to high-density lipoprotein cholesterol or the grading of transaminase abnormalities, but patients, in general, are more likely to worry about the impact of side-effects on their day-to-day life and long-term future. Patients are also concerned about potentially stigmatizing side-effects such as lipoatrophy and lipohypertrophy, drug efficacy and the lack of options in the future. Indeed, future options are often raised as an issue during discussions about treatment switching for toxicity reasons, with patients concerned that they will then lose that drug option. Physicians must be clear that stopping a drug due to side-effects does not necessarily preclude its future use.
Another important issue for patients is the time available in clinics, with some patients feeling ‘swept away’ by some service innovations. In the UK, the trend is towards less frequent monitoring than the traditional three-monthly intervals, and services such as telephone- and Internet-based follow-up and home delivery of drugs are being introduced. These innovations streamline services and enable physicians to see more patients, but for each individual it may mean less time spent in the clinic. Some patients will always need more face-to-face time, and services should be tailored so that patients who need more input have access to the time they need and deserve.
What Patients Need to Know
Why treatment is important and the options available
When patients start treatment, a multitude of factors must be discussed, and a good multidisciplinary team is invaluable for this. Two issues are key at this stage. First, it is important that patients understand the importance of treatment. A discussion of how antiretroviral drugs work can be helpful, with the degree of detail adapted for each patient. Generally, however, the patient should understand how the drugs reduce viral load and increase CD4 counts, why they will make them feel better in the long term and why adherence is so vital. Demonstrating the benefits of long-term treatment can also be useful – for example, graphics that highlight the dramatic improvements in life expectancy obtained with treatment can help motivate patients to take their tablets every day. The second key issue is a discussion of the pros and cons of individual agents and combinations. Patients often access data emerging at conferences on the Internet, and physicians have a duty to keep up to date and disseminate information to colleagues who may not have attended those meetings.
Counselling about side-effects
Preparing a patient to expect the potential side-effects of a medicine can go a long way towards helping to manage those side-effects. Furthermore, an unexpected side-effect is often more concerning and frightening for an individual than a side-effect about which they have received counselling. A balance is involved, however, as it is not possible to discuss every side-effect listed in the summary of product characteristics, but discussing common side-effects and making sure patients have quick access to advice where needed can minimize their impact. Careful use of adjunctive therapy and timely switching when necessary also helps in minimizing the negative impact of side-effects.
Current Evidence
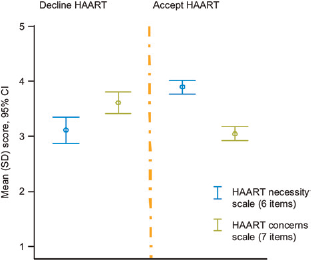
Patients’ belief in HAART is extremely important. A study of more than 130 patients determined two scores: a HAART necessity score (which indicated how necessary the patients thought HAART was) and a concern score (which indicated the degree of concern they had about HAART). Declining HAART (n = 38, 28%) was associated with doubts about necessity (odds ratio 7.41 [2.8–19.7], P < 0.001) and concerns about potential adverse effects (0.19 [0.07–0.48], P < 0.001) (Figure 5). These relations were independent of negative affect (depression) and clinical variables (CD4 count, viral load and years since HIV diagnosis). Patients’ relationships with their physicians and care providers are also crucial. In a sample of 1743 patients, those who replied ‘yes’ to the question ‘Does your HIV provider know you as a person?’ were significantly more likely to be on HAART, to be adhering to HAART and to have undetectable viral load than patients who replied ‘no’ or T don't know’.
11
Uptake of highly active antiretroviral therapy (HAART) in relation to baseline beliefs. Reproduced with kind permission from Home et al.
6
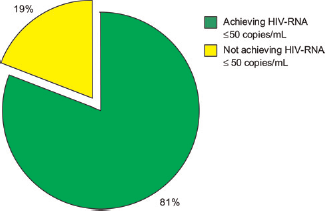
The positive outcomes that most patients obtain with treatment are another important message to convey. Data from the UK Collaborative HIV Cohort (UK CHIC), which includes a mixture of treatment-naive and -experienced patients, show that most patients who achieved an undetectable viral load over four years of follow-up maintained that viral load -even though a significant proportion were treatment experienced. Simple graphics showing such data can help emphasize the benefits of treatment to patients (Figure 6).
Percentage of patients on HAART achieving HIV-RNA ≤50 copies/mL (UK Collaborative HIV Cohort study; n = 12,648). Reproduced with kind permission from Benzie et al.
12
The manner in which information about side-effects is uncovered is important. Once physicians establish that a patient is doing well on treatment - with an undetectable viral load and an increased CD4 count - they may ask in passing if the patient has any side-effects, in which case the patient will often answer ‘no’. Physicians must therefore be specific when trying to discover whether a patient is experiencing any side-effects - for example, ‘Have you experienced any diarrhoea?’ may elicit a different answer. Importantly, patients may be experiencing considerable side-effects but tolerating them because of the positive impact of the treatment on their viral load and immunological results. Physicians must therefore emphasize that patients do not have to suffer with side-effects to achieve good results, as a combination with minimal or ideally no side-effects can often be found.
Treatment switch
For most patients the central nervous system (CNS) toxicities associated with efavirenz are transient and short lived and patients tolerate this drug well, which is why it features as a preferred agent in the BHIVA guidelines.
2
However, trials with newer agents, such as raltegravir and rilpivirine, showed that efavirenz is associated with high incidences of neuropsychiatric symptoms (Figure 7).13,14 In addition, some patients experience long-term CNS toxicity that may remain undetected if not managed appropriately. A retrospective analysis of a study that followed 40 patients who switched from efavirenz to nevirapine for CNS toxicity and elevated lipids found that 20 had neuropsychiatric side-effects.
15
All 20 reported an improvement after switching from efavirenz to nevirapine, with 14 (70%) reporting complete resolution of CNS toxicity. Eighteen patients in the study had sleep disturbance, and switching from efavirenz to nevirapine again provided improvement, with only one reporting no improvement and 14 reporting complete resolution.
Neuropsychiatric symptoms at 96 weeks in studies with raltegravir (RAL)*† (a) and rilbivirine (TMC278)‡ (b).1,2 *Raltegravir is not licensed for use in treatment-naive patients. †Depression, nightmare, confusional state, suicidal ideation, nervous system disorder, psychotic disorder, abnormal dreams, suicide attempt, acute psychosis, delirium, depressed level of consciousness, hallucination, auditory hallucination, completed suicide, major depression. ‡Rilpivirine is currently investigational and not licensed. **Once daily dose of 25 mg (dose being taken in Phase III trials). Reproduced with kind permission from Ward and Curtin
15
and Martínez et al.
16
EFV= efavirenz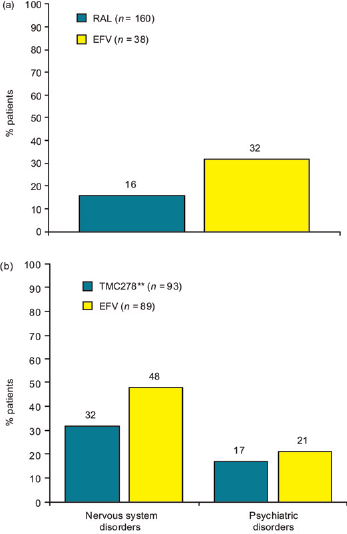
Switching clearly is important for resolution or at least improvement of many side-effects, yet there is frequently a reluctance to do so. This is probably a combination of physicians and patients being reluctant to switch treatment once vir-ological control has been achieved; however, several switch studies now show that, in general, virological efficacy is maintained after switching.16,17 More frequent monitoring is also a concern when a patient switches to a new agent, but most patients can usually find time for the few additional visits that may be required following a change in therapy. New side-effects or exacerbation of current side-effects are always a possibility when starting new drugs, but careful counselling, preparation and management of side-effects will help.
The NEFA study found that patients switching from PIs to abacavir had worse outcomes than those who switched to nevirapine or efavirenz over a three-year follow-up (perhaps not surprisingly considering what is now known about triple nucleoside combinations). 18 In studies such as RAVE and COMET,19,20 patients switching from thymidine to non-thymidine backbones maintained high rates of virological suppression. It is important to remember, however, that there will always be a small background failure rate year on year, whether treatment is switched or not.
Conclusion
All treatments are, to some degree, a compromise. Careful attention to preparing patients for treatment, careful initiation of therapy and ongoing evaluation (reassessing side-effects and assessing changes in patients’ lives that may mean a previously unimportant side-effect has become more important) can ensure that compromises are minimized. If fears about side-effects, stigma and the long-term future and options outweigh a patient's perception of the need for and benefits of treatment, patients are less likely to want to start HAART and more likely to adhere poorly once they do begin treatment. It is the duty of physicians to ensure that patients understand that the benefits of therapy outweigh the risks and in so doing to improve outcomes for all patients.