
Abstract
In 2004, the British Association for Sexual Health and HIV Scottish Branch audited HIV testing in new attendees diagnosed with a sexually transmitted infection at genitourinary medicine clinics in Scotland. In 2008 the audit loop was completed. Large increases were seen in rates of test offer and uptake, particularly in health boards with low baseline levels of testing. Overall rates of testing remain below those recommended and wide variability between boards persists.
INTRODUCTION
Late diagnosis of HIV continues to be a significant problem in the UK. Up to 24% of deaths associated with HIV are attributable to late diagnosis. 1 Delayed HIV diagnosis also has an impact on transmission: modelling suggests that over half of new infections are from people with undiagnosed HIV. 2 In 2004, a British Association for Sexual Health and HIV (BASHH) audit 3 was undertaken in Scotland against the Scottish Sexual Health Strategy standard of offering HIV testing to all genitourinary (GU) medicine attendees with acute sexually transmitted infection (STI) and documenting reasons for non-uptake. The results were presented at a Scottish BASHH meeting and published in the International Journal of STD and AIDS. In 2008/2009, the audit was repeated against this and subsequently published Scottish and UK HIV testing standards.
METHODS
The first 200 cases attending the largest GU medicine clinics in each health board during the first quarter of 2008 were taken from the STI Surveillance Scotland database. Cases were stratified by diagnosis of an acute STI; defined as chlamydial infection, non-specific urethritis, gonorrhoea, syphilis, trichomoniasis, first episode of genital warts or herpes, acute hepatitis B and first diagnosis of hepatitis C. Contacts of STI were also included. An auditor examined the records of those untested, recorded the offer of test and reasons for non-offer or declining.
RESULTS
A total of 1484 cases were identified (smaller clinics had less than 200 clients in the audit period), of which 1302 were eligible. The remaining 182 were not examined because 126 were known HIV positive, 19 were postal testing kits and never attended services, 26 notes were missing and in 11 no reason was given by the auditor for lack of information. In all, 573 cases were coded as untested for HIV and their notes examined.
Data for 2008 were not available for boards 2 and 10: one health board had been amalgamated with others and no longer submitted data independently, in another it was not possible to identify first attendees by clinic number.
Rate of HIV test offer (range) in all attendees was 82% (65–93%). Rate of test acceptance was 69% (49–79%) and rate of HIV testing was 56% (39–73%). The documentation of reasons for non-offer of HIV test varied from 23% to 100%.
Reasons given for declining a test were: 26% felt they were at low risk for HIV, 15% were needle phobic, 9% deferred their test until end of window period but did not return in the three months, 2% didn't want to know the result and 2% were for other reasons. For 45% no reason was given.
In all, 675/1302 (52%) eligible cases in 2008 were new attendees, of which 488 (72%) had an acute STI. The rate of offer of test in new attendees with an acute STI across Scotland in 2008 (2004) was 92% (61%) and the rate of testing was 65% (35%) (Figure 1). In 2008, three boards approached the standard of 100% offer of HIV testing in new attendees with an STI and, in all but one board, the rate of offer exceeded 90% (Figure 2).
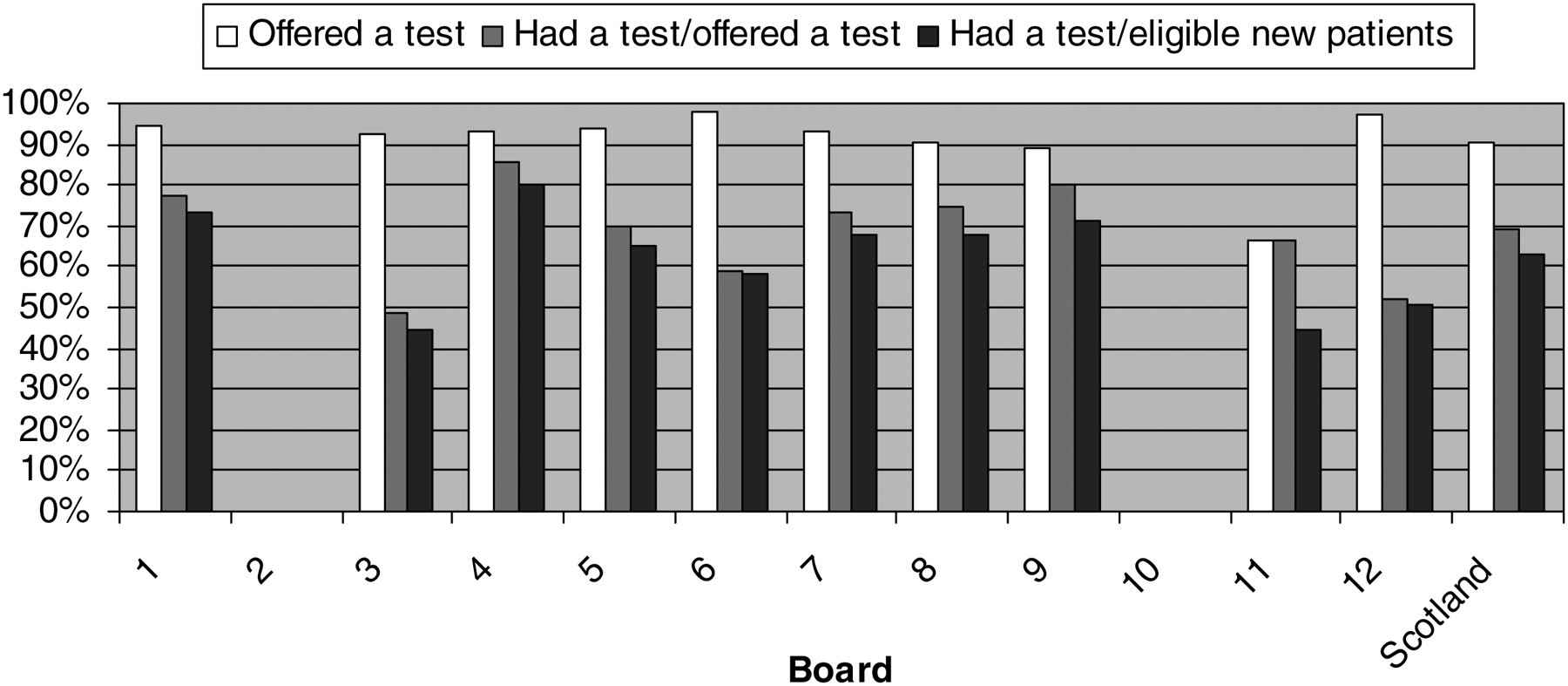
Offer and uptake of HIV testing by board, new attendees with acute STI, 2008. STI = sexually transmitted infection
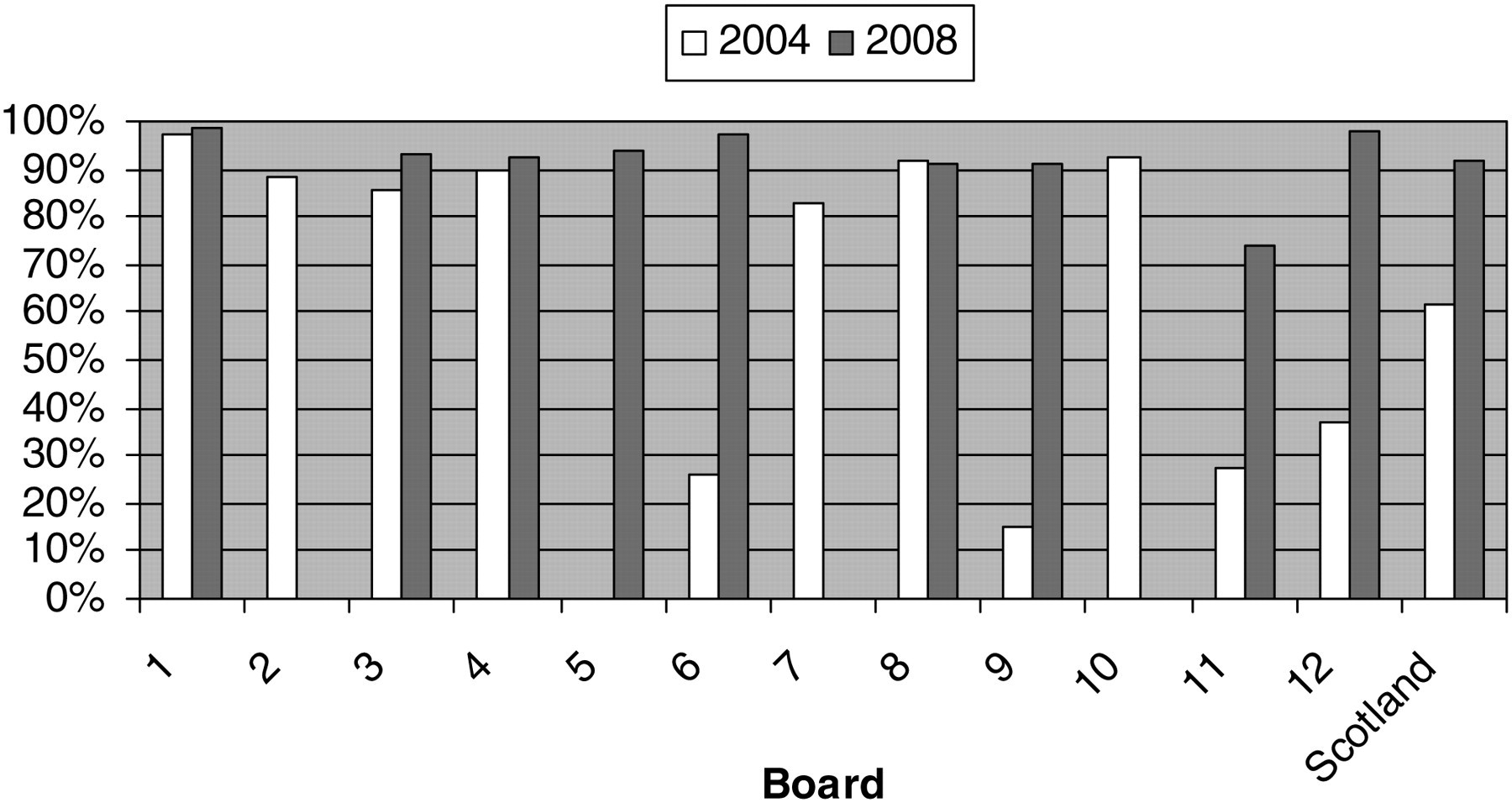
Proportion of new attendees with an STI offered an HIV test: 2004 versus 2008. HIV, human immunodeficiency virus; STI, sexually transmitted infection
In 2008, a total of 97 first attendees were members of groups with increased HIV prevalence (17 Black African/Caribbean, 58 men who have sex with men [MSM], 22 intravenous drug use [IVDU]). Ninety-three out of 97 cases (96%) were offered an HIV test of which 84/93 (90%) accepted. The overall uptake of HIV testing was 84/97 (87%). Of MSM first attendees in 2008 (2004), 58 (25) were eligible for HIV testing, 55 of which (25) were offered a test: rate of testing 95% (100%). In IVDU first attendees in 2008 (2004), 23 (14) were eligible for testing of which 22 (14) were offered a test: rate of test offer 96% (100%).
DISCUSSION
This audit cycle demonstrates dramatic changes in practice. It is not possible to attribute these changes to the feedback of the original audit findings to individual boards but this seems likely to have been a factor. The lowest rate of HIV test offer to new attendees with a STI improved from 0% to 74% and the biggest change in any single board was from 0% to 94%.
Documentation of why the offer of a test was not accepted has also improved from 28% to 53%, but there appears to be significant differences between clinics either in the recording of test offer, or the way in which tests are offered, that affects the likelihood of a test being accepted. Consequently in four boards the rate of testing in new attendees with an STI remained below 70%, the lowest rate of testing being 45%. The rate of test offer to those from higher prevalence groups has fallen to slightly below 100% and this is of some concern.
The most common documented reason for test refusal was self-perceived low risk. Similar findings were seen by Burns et al. 4 and, worryingly, their study suggested that a large proportion of clients who had perceived low risk in fact ‘did have significant risk factors’. In addition, a study from the USA found that test refusers were 2.2 times more likely to be HIV positive. 5 It is therefore important to still encourage testing within this group. One method that has been seen to be effective is providing clients with more information about the test: Wickramasinghe and Rogstad 6 showed a statistically significant association between test acceptance and receiving an information leaflet.
The rate of HIV testing among all GU medicine attendees in Scotland in 2008 (56%) remains considerably lower than the rates reported from 15 sentinel clinics in England in the same year 7 (93%). The denominator in the English data excludes those who do not have blood taken and is not directly comparable to the Scottish figure. It is not clear whether our audit data are merely more accurately representative of the testing rate across a range of clinics and settings, including those with fully integrated sexual and reproductive health services, or if there is a large difference between testing rates in comparable services in the two nations.
These results have been disseminated to the individual boards and discussed at a national meeting. The full audit report is available on the BASHH website.