
Abstract
Cryptococcus remains an important opportunistic infection in HIV patients despite considerable declines in prevalence during the highly active antiretroviral therapy era. This is particularly apparent in sub-Saharan Africa, where Cryptococcus continues to cause significant mortality and morbidity. This review discusses the microbiology, epidemiology, pathogenesis and clinical presentation of cryptococcal infections in HIV patients. Additionally, a detailed approach to the management of cryptococcosis is provided.
INTRODUCTION
Cryptococcus neoformans is an encapsulated yeast that remains an important pathogen, particularly among patients with the human immunodeficiency virus (HIV). A rare disease prior to the HIV epidemic, Cryptococcus is now among the leading causes of meningitis in sub-Saharan Africa. 1,2 Despite the advent of highly active antiretroviral therapy (HAART), Cryptococcus is a significant disease among HIV-infected persons. For example, the 10-week mortality in HIV patients in developed countries remains high, ranging from 10% to 25%. 3,4 In resource limited settings, mortality is even higher, with rates of 37–43%, even when amphotericin B has been used. 5,6 In a Zambian study of 130 AIDS patients without access to antiretroviral therapy who were treated with fluconazole (200 mg), the six-month mortality was 100%, with a median survival of only 19 days. 7
This review discusses the epidemiology and pathophysiology of cryptococcosis, as well as its most notable clinical manifestations. Additionally, a summary of the approach to treatment for Cryptococcus, as described in recent guidelines, is provided. 8
MICROBIOLOGY AND EPIDEMIOLOGY OF CRYPTOCOCCAL INFECTIONS IN HIV PATIENTS
The asexual yeast C. neoformans had been classified as four serotypes based on the capsular polysaccharide, glucuronoxylomannan. 1 Capsular types A through D correspond to the variants C. neoformans var. grubii (A), C. neoformans var. gattii (B and C) and C. neoformans var. neoformans (D). Recently, Cryptococcus gattii has been classified as a separate species, as detailed analysis has shown it to be genetically distinct from C. neoformans. 9
Cryptococcus is distributed worldwide and exists in high concentrations in bird guano, particularly pigeons and chickens. 10,11 However, human infection usually occurs without a history of direct contact with birds. 1 C. gattii, on the contrary, generally occurs in the tropics and subtropics and is found in decaying vegetation, particularly from the red river gum (i.e. eucalyptus) trees. 12 An outbreak of C. gattii infections that occurred on Vancouver Island from 1999 to 2004 was linked to the importation of eucalyptus trees from Australia. 13,14
Cryptococcus is a well-recognized opportunistic infection among those with deficits in cell-mediated immunity, such as HIV patients and other immunocompromised populations including patients with organ transplantation and rheumatological conditions requiring immunosuppressive agents. 15,16 In HIV patients, it is classified as an AIDS-defining condition. 17 Despite the reduction in the number of cases among HIV patients since the advent of HAART in the developed world, 18 approximately one million cases of cryptococcosis occur worldwide each year, 19 with the largest burden in Africa. In the USA, cases continue to be seen, especially among HIV patients diagnosed late in the disease course and among persons receiving immunosuppressive agents.
PATHOGENESIS AND CLINICAL MANIFESTATIONS
Cryptococcus is a basidiomycetous yeast that survives environmentally in the sexual form, producing hyphae with terminal basidiospores (chains of unbudded yeast). These basidiospores may break off and become aerosolized, 1 and at 3 µm in size, are small enough to deposit in the alveoli. 20 In the majority of hosts, infection is asymptomatic. However, in the patient with severe cell-mediated immunodeficiency, the organism may enter the circulation and survive in vivo in the haploid, asexual state leading to disseminated disease. The characteristics of Cryptococcus that permit its survival within the host include a polysaccharide capsule, which allows the organism to escape phagocytosis. 21,22 Further, the phenol oxidase enzyme uses catecholamines as substrate to produce melanin, which accumulates in the cell wall. It is the use of catecholamines that may provide a predilection for involvement of the central nervous system (CNS). 23
Clinical manifestations of Cryptococcus most commonly involve the lungs and CNS, although several other sites may be involved. The site of infection appears to vary by the serotype of Cryptococcus and the immunocompetence of the host. For example, C. gattii typically causes a pulmonary infection in immunocompetent hosts, but may also cause disease among HIV-infected persons. Pulmonary disease usually presents as an acute pneumonia or as non-calcified granulomas, which are often difficult to detect radiographically. Some patients develop a prolonged cough or dyspnoea due to chronic pneumonia.
Cryptococcus typically causes opportunistic disease in patients with deficits in cell-mediated immunity. 3,15,16,24 Although incidence and mortality have decreased in the era of HAART, cryptococcal meningitis remains an important cause of morbidity and mortality in the AIDS population, especially in the developing world. 25 Cryptococcal meningitis generally presents with a headache of insidious onset and several weeks duration. Fevers usually do not occur until late in the disease course, and nuchal rigidity is often absent. 1 In AIDS patients with cryptococcal meningitis, extraneuronal involvement is quite common, as high as 50% in one case series. 26 Common sites of infection include the lungs, bone marrow, skin and genitourinary tract. 27 Cutaneous dissemination may be seen in about 10% of cases (typically described as molluscum-appearing skin lesions) and as osseous involvement in approximately 5%. 1 While cryptococcal meningitis generally occurs in immunocompromised patients, it can be seen in immunocompetent individuals as well. 28,29
DIAGNOSIS
The diagnosis of cryptococcosis is most often made by the latex agglutination test for capsular polysaccharide antigen. This antigen can be obtained from either cerebrospinal fluid (CSF) or serum, and when present in CSF, is over 90% sensitive and specific for the diagnosis of cryptococcal meningitis. 30 False-positives can occur though, particularly in the presence of a positive rheumatoid factor. 31 In resource-limited settings, the latex agglutination antigen test is often not available, thus methods of detection of the organism include blood cultures (Figure 1), CSF culture and India ink smear. However, India ink stains are less sensitive than the capsular antigen. 1 In one study of HIV-negative adults with cryptococcosis, India ink was 51% sensitive and CSF culture 89% sensitive among the 157 patients with meningitis. In contrast, the antigen test had a sensitivity of 97% and 87% from the CNS and blood, respectively. 32 In a study involving both HIV-positive and -negative patients, the India ink stain was positive in 80% (48/60) of patients with cryptococcal meningitis. 33 If isolated from culture, Cryptococcus appears as singular, narrow-based budding yeast that is urease negative and can be distinguished by its preferential growth on birdseed agar (see Figures 1–4).
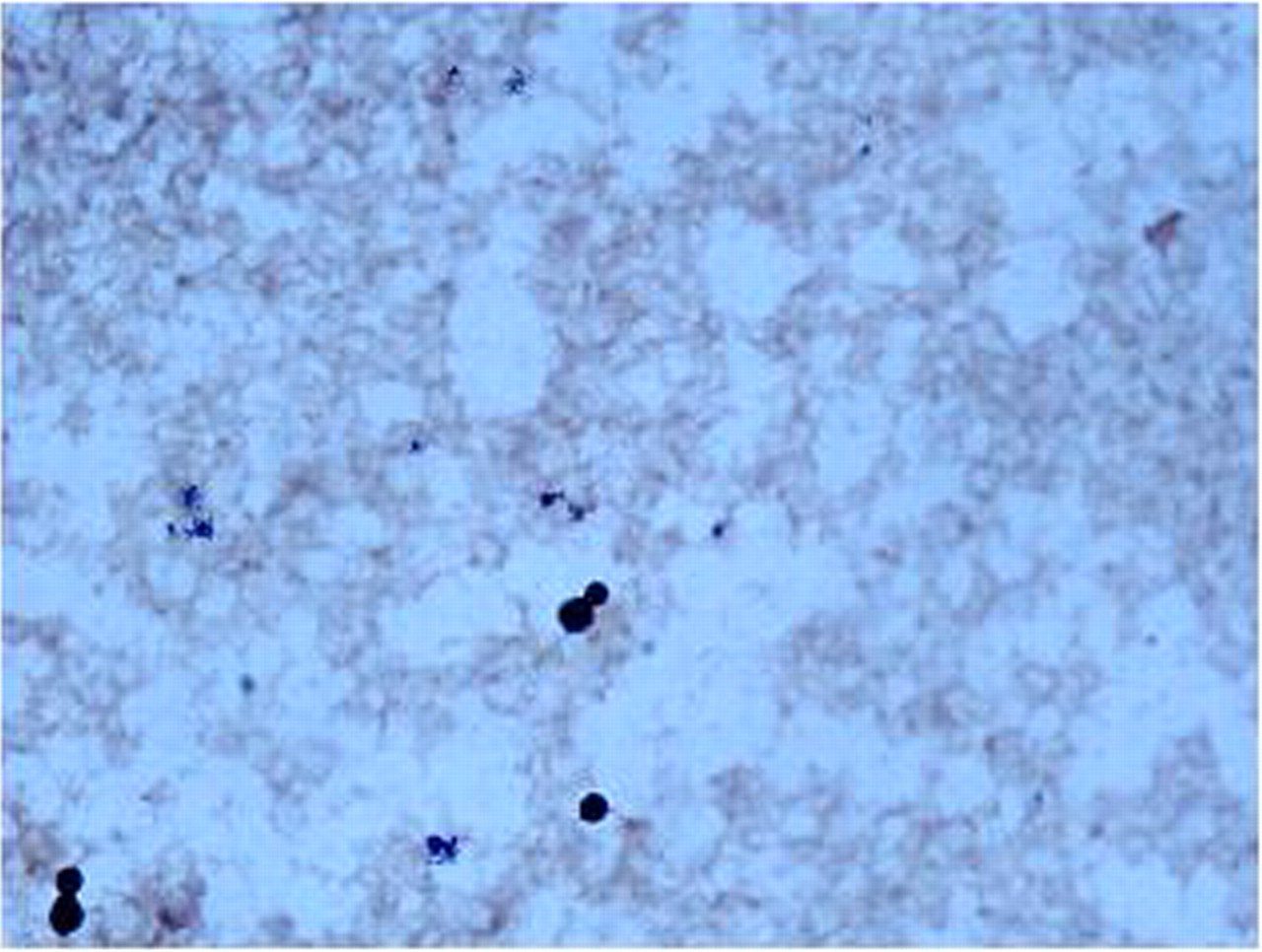
Gram stain from a positive blood culture of a patient with AIDS showed narrow-based budding yeast
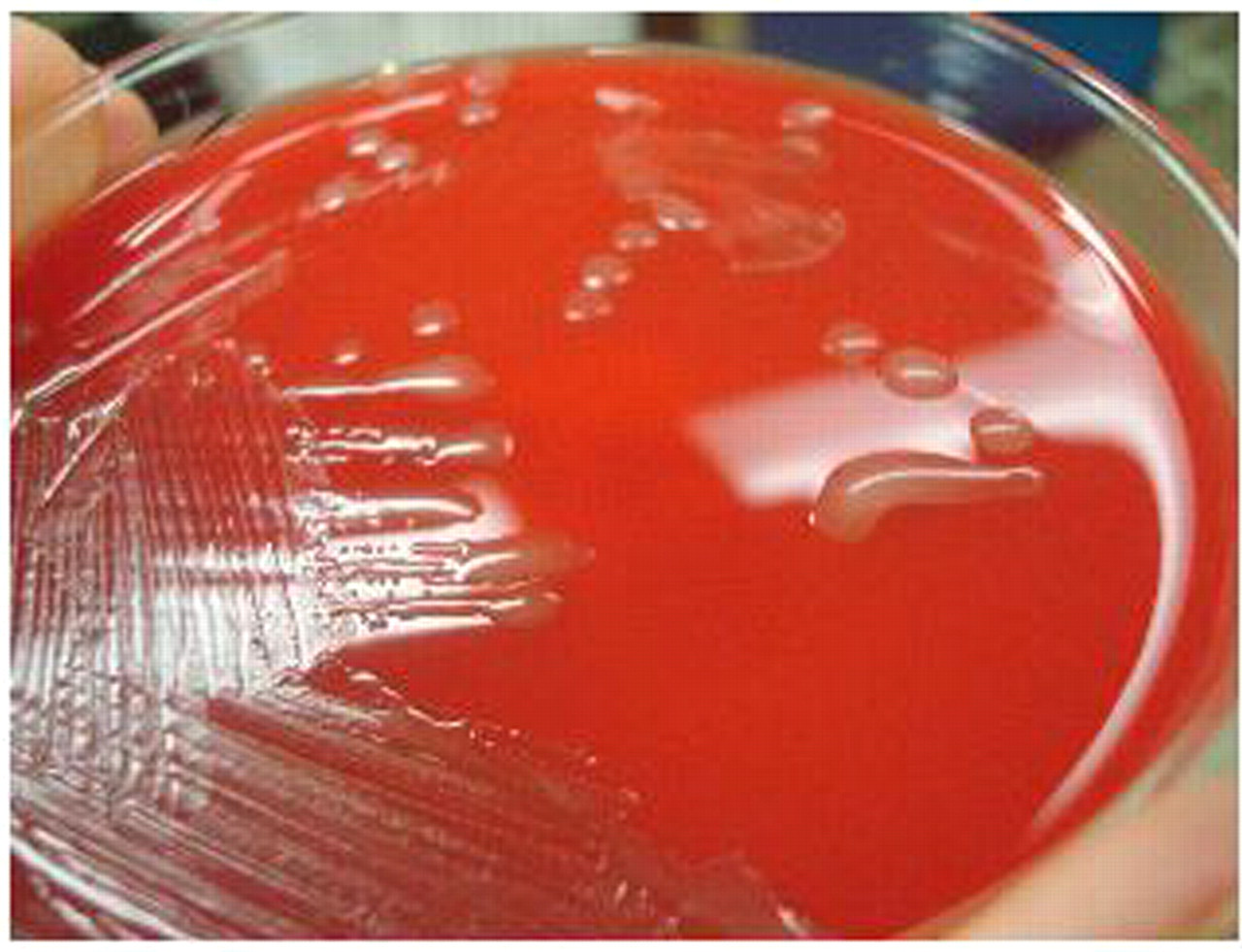
The yeast grew on fungal media (Sabouraud dextrose agar), chocolate agar and sheep's blood agar (shown here), displaying cream coloured, smooth, mucoid colonies
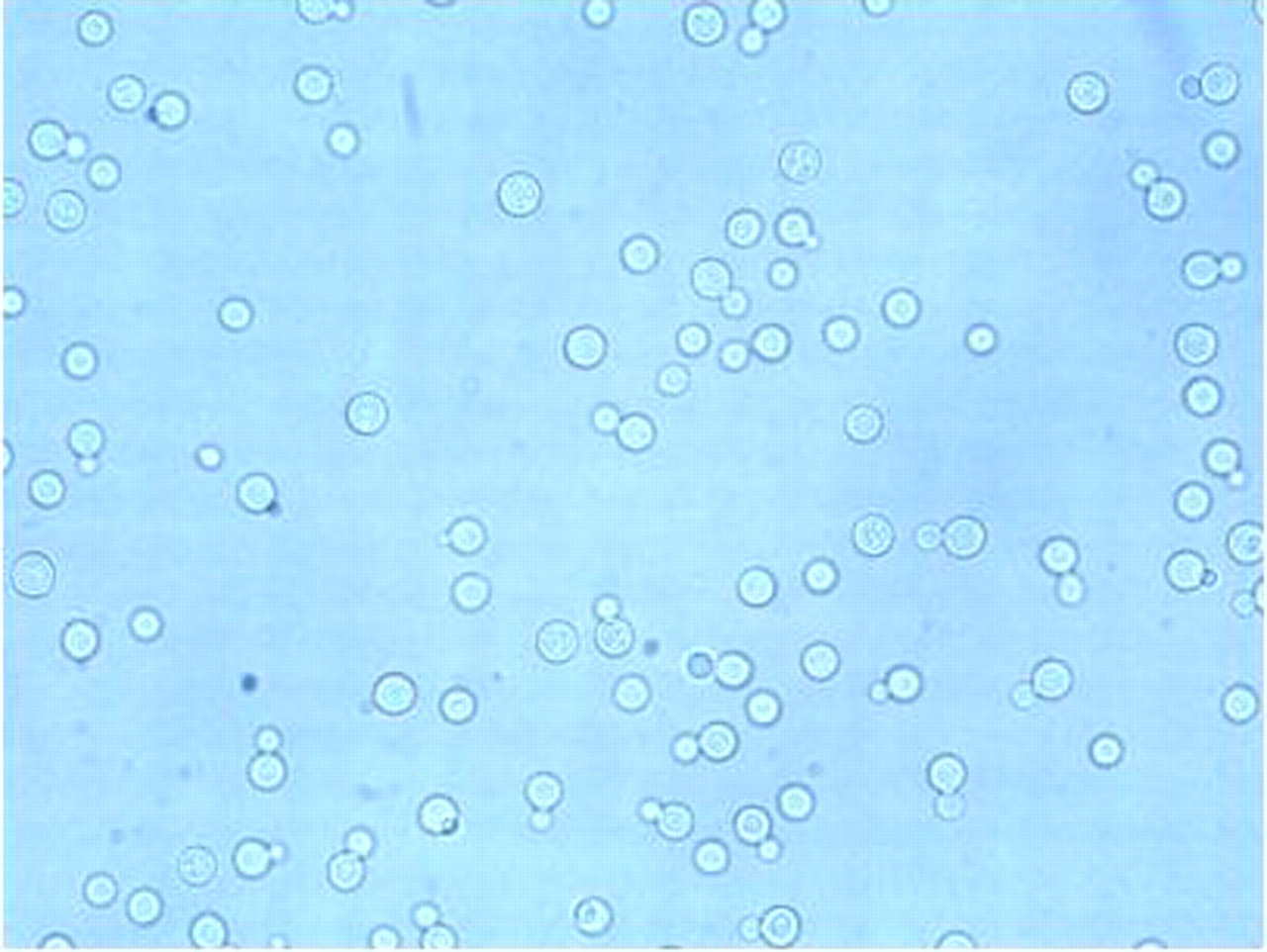
Wet mount from the colonies in Figure 2 showing round celled yeast, with narrow budding single-daughter cell, consistent with Cryptococcus

Cryptococcal neoformans was confirmed by both biochemical testing and the brown coloured colony growth on birdseed agar, as C. neoformans selectively absorbs melanin from this media (top is patient's sample, and bottom is negative control growing Candida albicans)
The diagnosis of cryptococcal meningitis is established by lumbar puncture, which usually shows elevated opening pressure, high protein and elevated white cell count. The indicators of more severe disease on CSF sampling include elevated opening pressure, low glucose, leukocyte count less than 20 cells/mm3, elevated cryptococcal antigen titre and the presence of the organism by India ink stain. 34
TREATMENT
The treatment for meningitis or other forms of invasive cryptococcal disease is divided into a two-week induction phase, followed by an eight-week consolidation phase, and then a prolonged maintenance phase thereafter. 35,36 An important distinction is made in the guidelines to differentiate treatment of CNS versus non-CNS disease 8,35 ; therefore, a lumbar puncture should be performed among immunocompromised patients with cryptococcal disease to rule out meningitis. 8
The recommended initial management of cryptococcal meningitis in patients with HIV consists of the rapidly fungicidal regimen of amphotericin B (0.7–1 mg/kg/day) plus flucytosine (100 mg/kg/day; Table 1). 8,35 Clinical outcomes were improved in AIDS patients with cryptococcal meningitis in South Africa when the induction phase consisted of the combination of flucytosine and amphotericin B, versus amphotericin B alone. 36 Studies have shown that amphotericin B (0.7 mg/kg/day) plus flucytosine (100 mg/kg/day) was found to be more rapidly fungicidal and have lower risk of mycological failure at two weeks than amphotericin B alone or in combination with fluconazole. 37,38
Recommended therapy for cryptococcal meningitis, disseminated disease or fungaemia in HIV patients
Adapted from Perfect JR, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 Update by the IDSA. Clin Infect Dis 2010;
HAART, highly active antiretroviral therapy
*Amphotericin B deoxycholate (AmBd) 0.7–1 mg/kg intravenous daily
†Lipid formulations of amphotericin (LFAmB): Liposomal AmB 3–4 mg/kg daily or AmB lipid complex (ABLC) 5 mg/kg intravenous daily
‡Flucytosine 100 mg/kg daily, divided four times a day, oral route preferred
§Already receiving fluconazole
**Maintenance therapy to be continued for at least 12 months. Can then consider stopping if receiving HAART with a CD4 > 100 cells/mm3 and undetectable or low HIV viral load for at least three months
††Reserved for patients not able to tolerate azoles
Regarding the appropriate dose of amphotericin B, a study compared two different doses (0.7 versus 1 mg/kg/day) in a group of HIV patients with cryptococcal meningitis in South Africa 39 ; both groups were also treated with flucytosine for 14 days. The higher dose amphotericin B was more rapidly fungicidal. While there was no difference in mortality in this study, it has been shown that more rapid clearance of infection correlates with improved clinical outcomes. 40,41
Lipid formulations of amphotericin are considered as alternate therapies to amphotericin B; these agents are useful in the setting of renal impairment and are generally associated with fewer adverse events compared with amphotericin B. Although there has been no proven benefit in clinical outcomes with liposomal amphotericin, a trend toward earlier fungicidal clearance has been shown. 42,43 Of note, these formulations are considerably more expensive and are generally unavailable in resource-limited settings. For any amphotericin product, it is important to provide intravenous hydration before and after dosages as a renal-protective measure, and to monitor electrolytes and kidney function closely. 8 Typically patients receiving amphotericin require administration of supplemental potassium, and sometimes magnesium and phosphorus as well.
Improvement in outcomes for patients with cryptococcal meningitis depends not only upon the choice of initial antifungal therapy, but also appropriate management of elevated intracranial pressure (ICP). An increased opening pressure is a poor prognostic indicator in cryptococcal meningitis 34,44 and is associated with higher CNS fungal burden. 45 Therefore, opening pressures greater than 25 cm of CSF should be treated with serial (e.g. daily) lumbar punctures until the pressure normalizes to less than 20 cm of CSF. 8,35,44 One approach is to remove a CSF volume that halves opening pressure (typically 20–30 mL), especially in settings of extremely high pressures. 8,35,46 For recurrent symptoms, repeat lumbar drainage should be performed. While CNS mass lesions or cryptococcomas are uncommon, imaging with CT scan or MRI should be performed prior to lumbar puncture to avoid the risk of herniation. 8 Placement of temporary lumbar drain may be necessary if opening pressure cannot be otherwise controlled, particularly if neurological sequelae are persistent. 35,47
Even in the absence of neurological symptoms, a lumbar puncture should be performed among immunocompromised patients with cryptococcal disease to exclude underlying meningitis. Even in the absence of meningitis, immunocompromised patients with severe or disseminated disease (i.e. involvement in more than one organ system or a positive blood culture for Cryptococcus) should be managed with the same antifungal regimen as those with meningitis. 8
In resource-poor settings, some recommendations are difficult to adhere to, since amphotericin B, and particularly its lipid formulations, may not be readily available. 42 While data are limited regarding the most effective initial therapy in settings where there is no immediate access to these medications, a recent study showed that fluconazole at high doses (1200 mg daily) leads to a more rapid decrease in CSF antigen titre than traditional dosing of 800 mg daily. 48 Furthermore, a randomized controlled trial in Malawi showed that an oral induction regimen of fluconazole (1200 mg daily) plus flucytosine (100 mg/kg daily) resulted in earlier fungicidal clearance and a trend toward decreased mortality when compared with induction with 1200 mg fluconazole alone. 41 This approach is an alternative recommendation in current guidelines, 8 and particularly useful in Africa where fluconazole is now widely available, although access to flucytosine remains limited. 41 It is important to recognize that in cases where fluconazole alone is utilized, resistance has been reported (especially in Africa) and may result in symptomatic relapse. 49
If access to flucytosine is limited, the induction regimen of amphotericin B plus fluconazole is preferred. 8 A recently published phase II study showed a trend toward better long-term outcomes of induction therapy with amphotericin B plus 800 mg fluconazole daily compared with amphotericin B alone. 50
When amphotericin B formulation plus flucytosine can be used, the induction therapy should be continued for two weeks, after which time a repeat lumbar puncture should be performed to evaluate for CSF sterilization. Consolidation therapy with fluconazole 400 mg daily for 8–10 weeks should be initiated, but if the CSF culture is positive, consideration should be made for reinstituting the two-week induction regimen depending upon the clinical status of the patient (Table 1). 8 Of note, growth within the CSF typically occurs within one to two weeks. Extension of induction therapy is also recommended among patients who remain comatose, are clinically deteriorating, or have persistent elevated ICP and a poor clinical response. 8
In the HIV-positive patient with meningitis, lifelong maintenance therapy is often necessary. Following induction and consolidation therapy (Table 1), lifelong suppressive treatment with fluconazole (200 mg daily) is recommended once CSF sterilization has occurred. 8,35 Itraconazole (400 mg daily) can be used as well, but has been shown to be inferior to fluconazole, 51 therefore it is recommended only in cases where fluconazole cannot be given. 8 If immune reconstitution occurs due to initiation of a successful HAART regimen, the CD4+ T lymphocyte count remains greater than 100 cells/mm3 for at least three months and the HIV viral load is low/undetectable, consideration of discontinuation of therapy can be made.
Of note, a minimum of 12 months of antifungal therapy should be administered before discontinuation. Some specialists prefer to document sterilization of CSF with repeat lumbar puncture in this situation, although this practice is not essential. 35 One prospective randomized study of HIV patients with cryptococcal meningitis evaluated whether maintenance therapy could be stopped after HAART initiation and subsequent immune reconstitution. After 48 weeks of follow-up, there were no cases of recurrent meningitis in those patients whose maintenance therapy had been stopped. 52 However, if the CD4 count falls below 100 cells/mm3 during follow-up, maintenance therapy with fluconazole should be reinstituted. 8
Despite the important role of antigen testing in the diagnosis of cryptococcal disease, serum antigens have a limited role in monitoring response to therapy. 53,54 While the serum titre decreases over time in most patients, it does not differentiate well between clinical response and persistent disease. 53 However, monitoring the CSF antigen level may be useful during acute infection, in that an unchanging or increasing titre has been correlated with clinical and microbiological failure. 54
There are several notable drug interactions between the antifungal agents used to treat cryptococcosis and antiretrovirals. Nevirapine clearance is decreased two-fold by fluconazole; to compensate for this in one clinical trial, those who were prescribed nevirapine had their dosage of fluconazole decreased from 800 mg to 400 mg daily. 41 Fluconazole also increases the area under the curve for zidovudine, so monitoring for zidovudine toxicity is important when these drugs are co-administered. The combination of zidovudine and flucytosine administration carries the combined potential bone marrow toxicities of both agents, so close monitoring is warranted. Flucytosine levels should be monitored if this test is available, 35 but adverse effects have been relatively low in clinical trials performed in developing countries without drug level monitoring. 36,41
Finally, it should be noted that in HIV patients with cryptococcal meningitis who initiate antiretroviral therapy are at particularly high risk for the immune reconstitution inflammatory syndrome (IRIS), manifested by meningeal symptoms and elevated opening pressure. 55 In one study, up to 30% of patients developed IRIS when HAART was initiated within one month of diagnosis with cryptococcal meningitis. 56 It is important to monitor for signs of increased ICP (e.g. confusion, papilledema, clonus) and to manage it with serial lumbar punctures, especially if the ICP is high (>25 cm of CSF). 35 It is essential to determine if CNS symptoms are due to IRIS versus disease progression or relapse; results of repeat cultures and trends in CSF antigen titres can be helpful. 56 Management of IRIS cases includes continuation or introduction of antifungal therapy and in severe cases, consideration for corticosteroids. Recent guidelines suggest that initiation of HAART should occur 2–10 weeks after commencement of antifungal therapy in an effort to reduce the occurrence of IRIS, 8 with some favouring waiting closer to the 10-week time point. Overall, a history of cryptococcal infection is an important consideration before HAART initiation.
In addition to IRIS that occurs during the treatment of cryptococcal disease, ‘unmasking’ IRIS can also occur in which symptoms due to Cryptococcus appear after HAART is initiated. In a retrospective study in South Africa, stored plasma from 7% of patients who had initiated HAART were positive for cryptococcal antigen. In the subset of patients with CD4 count less than 100 cells/mm3, a cryptococcal antigen titre of 1:8 was 100% sensitive and 96% specific for predicting the development of cryptococcal meningitis during the first year of HAART, suggesting a potential role for a pre-emptive treatment strategy in this highly endemic setting to reduce the risk of the development of both meningitis and IRIS; further studies are needed. 57 Primary prophylaxis among HIV patients in the USA is not currently recommended. 8
Alternate therapies such as mannitol or acetazolamide for elevated ICP in the setting of meningoencephalities are not currently recommended. 8 Corticosteroids may be considered in select settings, including IRIS with CNS inflammation and increased ICP, cryptococcomas with mass effect and oedema, and acute respiratory distress syndrome (ARDS).
For patients who develop pulmonary cryptococcosis with mild to moderate illness (no diffuse pulmonary infiltrates, ARDS or dissemination,) fluconazole 400 mg for 6–12 months is recommended (Table 2), although there have been no randomized trials to date that have determined the optimal treatment in HIV-infected persons. 8 Patients with disease manifesting as a severe pulmonary illness, such as ARDS, should be initially managed with amphotericin B (0.7–1 mg/kg/day) plus flucytosine, as in meningitis. 8 Therapy for non-CNS disease can generally be discontinued after one year of therapy if the CD4 count is >100 cells/mm3 and the titre is ≤ 1:512 and/or is stable.
Treatment approach for pulmonary cryptococcosis in HIV patients
Adapted from Perfect JR, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 Update by the IDSA. Clin Infect Dis 2010;
CONCLUSION
In summary, cryptococcal disease remains an important cause of morbidity and mortality, particularly in HIV patients in resource-poor environments. Cryptococcal infection should be considered in the differential diagnosis of immunocompromised patients presenting with meningitis, pneumonia or molluscum-like skin lesions. Updated treatment guidelines have recently been published to assist in the management of cryptococcal disease. 8 Although still a significant cause of morbidity and mortality in the HIV patient, great strides have been made to reduce this burden through adherence to treatment guidelines and the availability of HAART.