
Abstract
Little is known about the predictors of antiretroviral treatment (ART)-associated tuberculosis (TB) in developing nations. The objective of this study was to determine predictors of ART-associated TB in adults with HIV infection at Jimma University Hospital, Ethiopia. A nested case-control study was conducted in October 2009. The study population consisted of adults with HIV infection (aged >14 years) who developed active TB in the first six months since ART initiation and controls that did not develop active TB. Data were collected using a structured and pretested questionnaire. Cox proportions hazards analysis was done to determine predictors of ART-associated TB. A total of 357 patients (119 cases and 238 controls) participated in the study. After six months of follow-up, cumulative incidence of ART-associated TB was 5.2% (123/2355). Forty (33.6%) cases were lost to follow-up after they developed ART-associated TB and 11 (9.2%) died. Fifty-one (21.4%) controls interrupted ART and 11 (4.6%) died. A CD4 lymphocyte count increase >0.5/μL/day (adjusted hazard ratio [AHR] = 19.80, 95% confidence interval [CI]: 9.52, 41.12, P < 0.001), a base-line CD4 lymphocyte count <200 cells/μL (AHR = 9.59, 95% CI: 2.36, 39.04, P = 0.002), World Health Organization (WHO) clinical stage 3 or 4 (AHR = 3.04, 95% CI: 1.62, 5.69, P < 0.001), night sweats during ART initiation (AHR = 1.53, 95% CI: 1.06, 2.21, P < 0.001) and high ART adherence (AHR = 1.30, 95% CI: 1.13, 1.50, P < 0.001) were independent predictors of ART-associated TB. HIV-infected adults with these risk factors should be followed cautiously for the development of ART-associated TB. Good ART adherence and a good immunological response during ART were associated with ART-associated TB, most likely because of an immune reconstitution inflammatory syndrome unmasking the TB.
Keywords
INTRODUCTION
In sub-Saharan Africa, tuberculosis (TB) has long been identified as the first cause of HIV-related mortality in adults. 1 Even though antiretroviral treatment (ART) has decreased the incidence of HIV-associated TB by 80%, TB remains the most common cause of morbidity in adults receiving ART. 2–4 A higher mortality was observed in patients who develop TB after ART initiation compared with those who did not develop TB, and only 50% of patients who develop TB after ART successfully complete their TB treatment. 5 In African countries with the highest TB mortality rate, the HIV-positive TB mortality rate is 2.2 times greater than the HIV-negative TB mortality rate. 4
TB occurring after the initiation of ART in resource-poor settings can be due to undiagnosed prevalent TB or subclinical TB becoming apparent after ART initiation (unmasking). 6 Unmasking TB immune reconstitution inflammatory syndrome (IRIS) defines a subset of patients with ART-associated TB who develop rapidly progressive signs and symptoms of TB after initiation of ART. 7
We determined in a case-control study the incidence and risk factors for ART-associated TB among patients treated for HIV infection in a referral hospital in Ethiopia.
METHODS AND MATERIALS
A nested case-control study was done at the Jimma University specialized referral hospital that serves more than 10 million people in Ethiopia. The study took place from 30 September 2009 to 30 October 2009, and included all adult patients with HIV infection ever enrolled for ART since 8 June 2003 through 14 August 2009. During the study period, a total of 4499 clients were enrolled for HIV care at the ART clinic of the hospital of whom 2355 adults were taking ART. From this cohort, cases and controls were included in the study. Cases were all adults above the age of 14 years diagnosed with active TB within the first six months after initiation of ART (ART-associated TB). Controls were adults who did not develop active TB after initiation of ART. Patients who started ART while on TB treatment were excluded. The diagnosis of TB was based on the World Health Organization (WHO)'s case definitions and diagnostic algorithms, 8,9 and the clinical judgements of the clinician in charge. For each case, two controls were selected using systematic random sampling.
Data were collected using a structured and pretested questionnaire by five trained resident physicians. The questionnaire was adopted from the nationwide and uniformly used patient registration and follow-up form of HIV patients in Ethiopia. The content of the questionnaire included sociodemographic and clinical characteristics of patients and outcome of ART-associated TB.
Data were cleaned for inconsistencies and missing values and analysed using SPSS 16.0 statistical software (SPSS Inc, Chicago, IL, USA). Univariate analysis was done to describe the sociodemographic and clinical characteristics of patients. To control for the effect of confounding variables, stepwise backward and forward proportional hazard regressions (Cox-regression) were done to identify predictors of ART-associated TB. All patients were censored at the time of the last recorded visit. All possible interactions up to order 2 were tested. All reported P values are two-sided. All analyses were performed using the STATA statistical analysis software package (Stata Corp, College Station, TX, USA). Ethical clearance was obtained from the ethical committee of Jimma University. Confidentiality was maintained for all the patients’ information provided.
RESULTS
One hundred and twenty-three (5.2%) adults developed ART-associated TB within the first six months of ART. Four cases were not included due to incomplete sociodemographic data. Therefore, 119 cases and 238 controls were included in the study.
Baseline characteristics of patients developing tuberculosis (TB) after initiating antiretroviral therapy (ART) versus controls not developing TB at Jimma University Hospital, Ethiopia
SD = standard deviation; WHO = World Health Organization; INH = isoniazid; TLC = total lymphocyte count; CI = confidence interval
*Students t-test
†Fisher's exact test
‡Denominator: only women (15–45 years)
§History of tuberculosis treatment completion before the initiation of ART
**The time interval between completion of pre-ART tuberculosis treatment and initiation of ART
††Denominator was 117 for cases and 199 for controls
‡‡Wilcoxon rank-sum test
P < 0.05 considered significant
A repeat CD4 count was not available within six months in two (1.6%) cases and in 39 (16.4%) controls (P < 0.001). Reason for the absence of a repeat CD4 count in the two cases was the duration between baseline determination and end of follow-up being less than three months. In the controls, the reasons for no repeat CD4 were drop out (53.8%), transfer out (25.6%), death (12.8%) and three (1.2%) had less than three months duration between baseline determination and end of follow-up. Baseline CD4 count was lower in controls having no repeat CD4 count than those where a repeated CD4 count was performed (P = 0.006). CD4 rise was 1.056/μL/day in cases compared with 0.276/μL/day in controls (P < 0.001). A receiver operating characteristic (ROC) curve exploring the best cut-off of CD4 count rise as a predictor showed CD4 count to be a very strong predictor with 92.5% area under the ROC curve (Figure 2).
One hundred and fourteen (95.8%) cases developed ART-associated TB within the first three months and five (4.2%) after three months of ART (Figure 1). Among 32 patients who developed ART-associated TB in the first two weeks of ART, 24 (75%) had a baseline CD4 count <50 cells/μL.
Occurrence probability of antiretroviral treatment (ART)-associated tuberculosis within the first six months after starting ART in Jimma, Ethiopia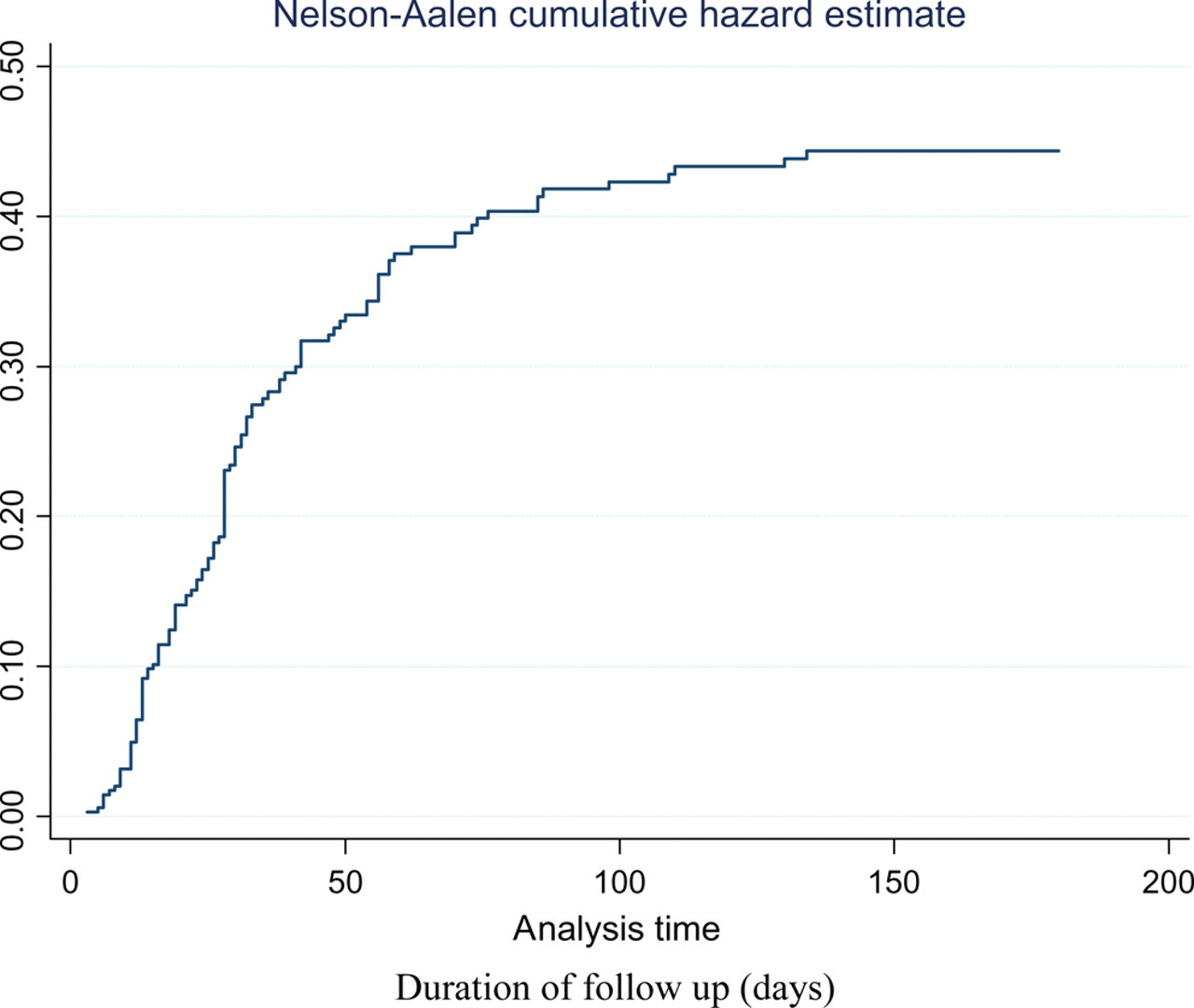
ART adherence was good in 118 (99.2%) cases before the development of ART-associated TB, but in only 79 (66.4%) cases during TB treatment. Among controls, 182 (76.5%) had good adherence to ART during the first six months of follow-up.
Among cases, after TB treatment initiation, 27 (22.7%) dropped out, two (1.7%) were lost, 11 (9.2%) died and seven (5.9%) were transferred out within six months of ART initiation. ART adherence was good in 79 (66.4%) cases after initiating TB treatment.
The rate of CD4 lymphocyte increase >0.5/μL/day was the most strongly associated independent predictor (adjusted hazard ratio [AHR] = 19.80, 95% confidence interval [CI]: 9.52, 41.12, P < 0.001) of ART-associated TB (Table 2; Figure 2). Baseline CD4 count <200 cells/μL (AHR = 9.59, 95% CI: 2.36, 39.04, P = 0.002), WHO clinical stage 3 or 4 (AHR = 3.04, 95% CI: 1.62, 5.69, P < 0.001), presence of night sweats for more than two weeks during ART initiation (AHR = 1.53, 95% CI: 1.06, 2.21, P < 0.001) and high ART adherence (AHR = 1.30, 95% CI: 1.13, 1.50, P < 0.001) were also independent predictors of ART-associated TB (Table 2).
Receiver operating characteristic (ROC) curve exploring CD4 change cut-off point for predicting antiretroviral treatment (ART)-associated tuberculosis in HIV-infected adults starting ART in Jimma, Ethiopia Predictors of developing tuberculosis (TB) after initiating antiretroviral therapy (ART) versus controls not developing TB, at Jimma University Hospital: Cox proportions hazards analysis HR = hazard rates; CI = confidence interval; ART = antiretroviral therapy; INH = isoniazid; WHO = World Health Organization *When ≥95% of ART is taken (i.e. of 30 doses ≤2 doses are missed or of 60 doses <3 doses are missed)
P < 0.05 considered significant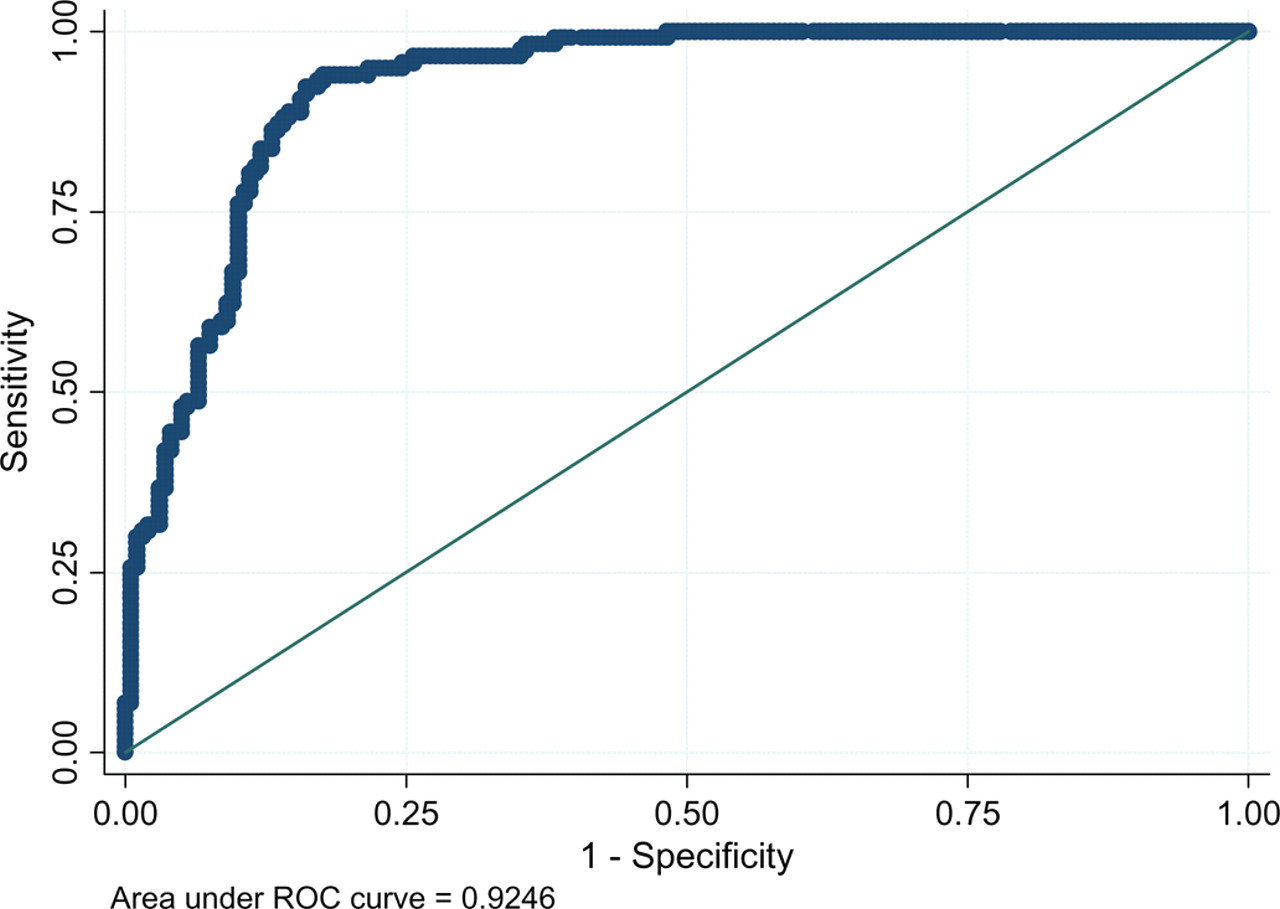
DISCUSSION
In our study, low CD4 count, WHO clinical stage 3 or 4 or night sweats during ART initiation were independent risk factors for ART-associated TB. Good ART adherence and a good immunological response during ART were also associated with TB, probably because of an IRIS unmasking the TB. Nevertheless, a portion of the ART-associated TB may reflect persistence of immune deficiency.
Only 5.2% of patients who commenced ART developed an ART-associated TB, which was low compared with the 11.8% previously reported from Addis Ababa. 10 A study done in Thailand reported a TB incidence density of 25.1 per 100 person-years. 11 We may have underestimated the number of ART-associated TB cases because a number of our patients dropped out, were lost to follow up or died. It has been well documented that after starting ART there is still a high early mortality rate because of TB. 12
In this study, the majority of patients (95.8%) developed active TB within three months of initiation of ART, which is similar to the previous reports. 13–15
Forty (33.6%) cases in this study disappeared after the start of anti-TB treatment and 11 (9.2%) died. The treatment of TB in patients taking ART is complex because of the high number of drugs administered simultaneously, which poses practical problem related to adherence and side-effects. 16–20 Previous studies have emphasized that adherence, adverse events and IRIS are important concerns in the concurrent management of TB and HIV. 10
The rate of CD4 lymphocyte increase of 0.5/μL/day was the main independent predictor of ART-associated TB, which has not been reported so far. Baseline CD4 count <200/μL was also an independent predictor of ART-associated TB, which is concordant with previous studies. 10,21–23
Night sweats of more than two weeks during ART initiation were a predictor of ART-associated TB. This suggests that the TB diagnosis was probably missed and that ART-associated TB could have been prevented by timely initiation of TB treatment. Unexpectedly, cough was not a predictor of ART-associated TB. We assume that in patients with cough, active TB case finding has taken place with sputum smear examination and, when indicated, chest X-ray to exclude TB before ART initiation, which is evident by the proportion with cough at ART initiation to be 17.6% in cases compared with 31.1% in controls (P = 0.007). Moreover, the fact that the cases had a lower mean baseline CD4 count compared with controls may in part suggest that the cases might be less responsive immunologically to develop cough while having ongoing pulmonary infection.
Good ART adherence was also an independent predictor of ART-associated TB. This could be explained by the fact that good ART adherence is associated with better immunological responses, leading to unmasking of TB after ART.
The limitation of our study is that since the repeat CD4 count determination of the cases might be done while taking both anti-TB therapy and ART, the initiation of anti-TB therapy in the cases might synergistically enhance the immunological response to ART unlike in the controls. Additionally, the lower baseline CD4 counts in controls having no repeat CD4 lymphocyte measurement compared with those having a repeat CD4 count may be a possible source of bias.
The strength of our study is that it has systematically addressed most of the possible confounders for the predictors of ART-associated TB and has explored various predictors including immunological response, which has not been reported before.
In conclusion, during routine care of persons with HIV infection TB remains under-diagnosed and treatment adherence of HIV/TB co-infected patients remains far from ideal. This study shows that HIV-infected adults with a low CD4 count, night sweats for more than two weeks, or in WHO clinical stage 3 or 4 at ART initiation should be followed cautiously for the development of ART-associated TB. Furthermore, good ART adherence and a good immunological response during ART were associated with TB, probably because of IRIS unmasking the TB. Finally, ART should be initiated earlier, before the CD4 count drops <350 cells/μL, as proposed by the new WHO guidelines.
Footnotes
ACKNOWLEDGEMENTS
We would like to thank all staff members of the Jimma University Hospital ART clinic and the medical team of Jimma University Hospital for taking care of the patients. NM has conducted the study, participated in the analysis of the data and written the paper. JPVG participated in the data analysis. All authors contributed to the design of the study, assisted with data interpretation, participated in the preparation of the manuscript and approved the final version.