
Abstract
In many British hospitals, HIV-positive patients access care via genitourinary (GU) medicine services. As a result of National Health Service (NHS) legislation, such patients may have information concerning HIV treatment filed separately from their general clinical records. We sought to evaluate accuracy of medication records of patients with both GU medicine and general hospital case-notes, and to assess clinical risk arising from incorrect or incomplete recording. In this retrospective review, 156 episodes of care from 100 HIV-positive patients with separate HIV case-notes were evaluated for accuracy of medication recording, when paired with clinical notes from attendances in other hospital departments. Discrepancies were observed in 52.6% of care episodes; significant discrepancies were apparent in 7.8%. The dual case-note system represents significant risk to patient care. We recommend that hospitals that continue to operate this system urgently consider amalgamation of HIV care records into hospital case sheets, in line with current national standards.
INTRODUCTION
Under the Data Protection Act 1998, there is a requirement to secure all patient information confidentially, and to disclose information only according to need. For example, clinical and medical histories may be accessed by practitioners involved in patient care. The National Health Service (NHS) Trusts and Primary Care Trusts (Sexually Transmitted Diseases) Directions 2000 specifically enforce confidentiality regarding information relating to sexually transmitted infections (STIs) and how these data can be shared, 1 and this has led to separate case-notes being kept by hospital genitourinary (GU) medicine departments from general hospital case-notes. For HIV-positive patients diagnosed and cared for by GU medicine departments, this could mean information concerning their HIV treatment is stored separately from information concerning any other conditions or treatment received from other hospital departments. Although information concerning HIV treatment is accessible to health-care professionals involved in care of a patient, the separate case-notes and often separate storage location may become a barrier to sharing important clinical information.
Since illness in HIV patients often presents to or requires input from other specialties, maintaining dual case-notes in such patients may pose a significant risk for medication error, duplication of tests or poor clinical practice. The British HIV Association Standards for HIV Clinical Care 2 recommend that information relating to HIV treatment should be recorded in ordinary NHS records and alongside that relating to any other condition, identified by patient name and date of birth. They do however state that information regarding sexual history and other STIs may be stored separately in GU medicine records.
In a survey of British GU medicine departments, combined case-notes were found to be in place in only 11% of centres in 2007; 3 42% of respondents reported encountering difficulties in communication that affected delivery of care for an HIV-positive patient and 67% of respondents felt that ‘normalization’ of HIV care would be the best option for HIV management.
We sought to assess the accuracy of medication records of HIV-positive patients who have both GU medicine and hospital case-notes. Since HIV patients often take complicated treatment regimens with a high propensity for drug interactions, 4,5 we assessed the clinical risks arising from incorrect or incomplete recording of medication, which could lead to significant interactions. As GU medicine and infectious diseases (ID) teams often work in partnership in the care of HIV patients and share access to secure electronic records and case-notes, we sought to ascertain whether medication recording errors are less frequent between GU medicine and ID, than between GU medicine and other directorates.
METHODS
This was a retrospective case-note review. After approval from the hospital audit department was obtained, medication lists recorded in general hospital case-notes from outpatient or inpatient episodes were compared with those in GU medicine case-notes, matched within 18 weeks from the date of the hospital visit and a routine GU medicine clinic visit. Medication information was obtained from various sources, including clinical notes, clinic letters/summaries, referral letters and inpatient drug prescription charts, which were filed in the patients’ notes.
Patients included were those accessing routine HIV care via GU medicine outpatient services and taking antiretroviral (ARV) therapy at the time of review. All patients had information relating to their HIV care filed in separate GU medicine case-notes and had accessed another department in the hospital, including ID, as an outpatient or inpatient between 1 January 2008 and 1 April 2010. Patients attending accident and emergency services as an isolated event were excluded, as were patients receiving their routine HIV care via ID outpatient clinics at the time of audit. Medication lists from both sets of case-notes were transcribed onto data collection forms that identified patients by a numerical code only, and these were subsequently entered into an anonymous database. A central list was maintained in the secure case-note storage area, which linked codes to patient details in order to allow follow-up of any discrepancies observed. All data collection and analysis were carried out by clinical staff involved in patient care.
Each discordance in medication recording between pairs of case-notes was analysed and discussed by a specialist registrar and a pharmacist involved in HIV care, to determine whether any actual or considerable potential for harm could have resulted from the medication recording discrepancy. A discrepancy was defined as any instance where information concerning a patient's medication differed between two sets of case-notes, when matched within 18 weeks. Harm was defined as any instance where a medication recording discrepancy caused a significant adverse impact on patient care including any of the following: a delay in appropriate treatment, delay in optimization of non-ARV therapy and prescription of incorrect medication. Potential harm was defined as any instance where a medication recording discrepancy posed sufficient potential risk to require intervention, for example, drug–drug interactions (DDIs) where one of the interacting drugs was not recorded in one set of case-notes, leading to potential for decreased efficacy of an ARV or a non-ARV, or toxicity. Errors considered to pose significant risk were acted upon.
RESULTS
The GU medicine case-notes of 100 patients were paired with corresponding hospital case-notes and from these, 154 episodes of general hospital care were evaluated. An episode of care was defined as a hospital visit which could be paired with a GU medicine clinic visit within 18 weeks. Patients attended a broad range of hospital departments (Figure 1). The ID unit was the department visited most frequently, accounting for approximately half of all attendances.
Range of non-genitourinary hospital departments visited by 100 HIV-positive patients receiving HIV care via genitourinary medicine services and taking antiretroviral therapy. ENT=ear, nose, throat surgery; ID=infectious diseases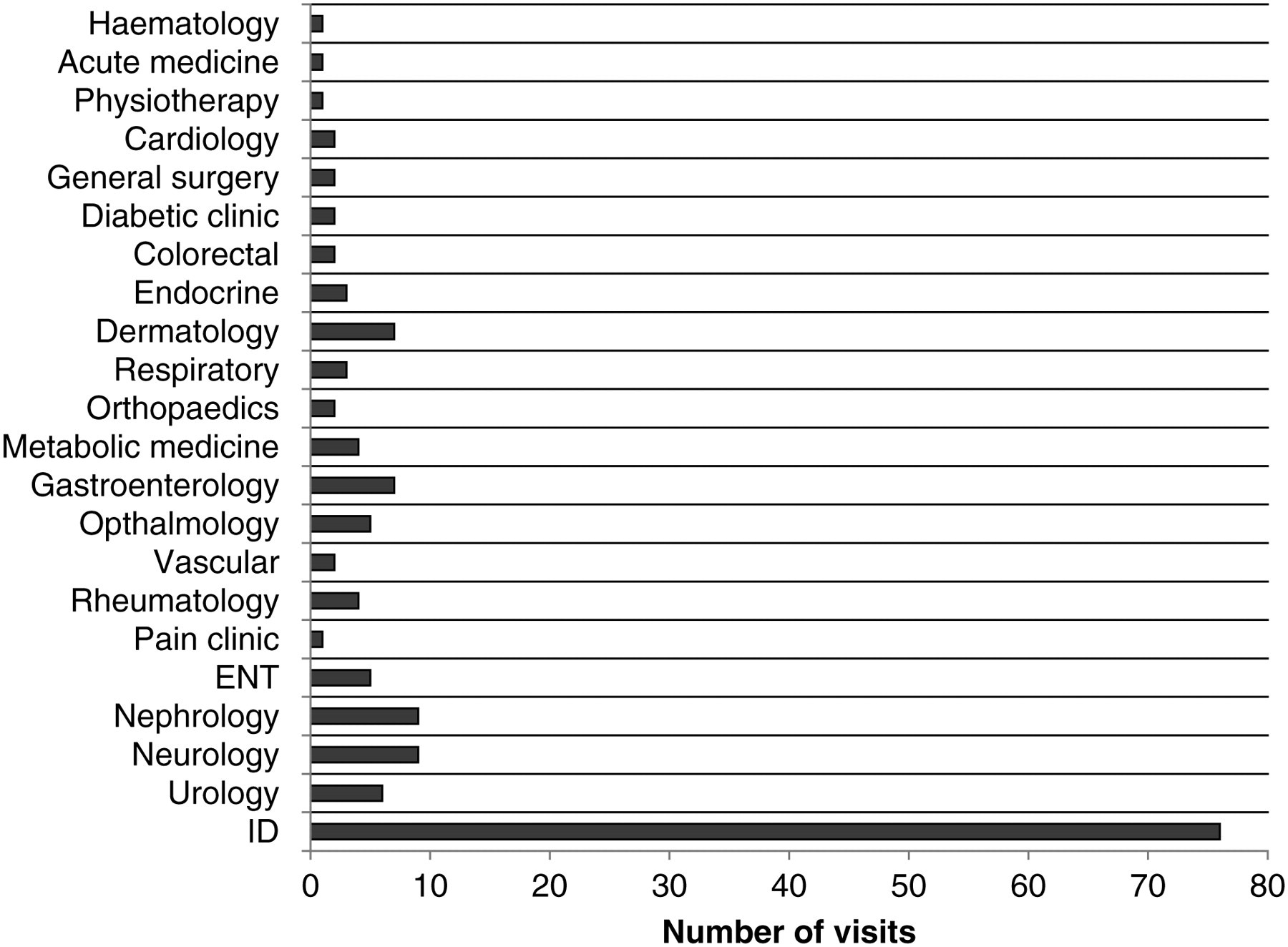
Medication recording discrepancies were observed between GU medicine and corresponding hospital case-notes in 52.6% of the episodes evaluated (Figure 2). Medication recording errors were categorized as follows: medication changed between the time of referral from one department to another and clinic attendance; doses of ARV agents not recorded in hospital notes; allergy recorded in one set of notes but not the other; DDIs which would usually require monitoring or dose adjustment that could not be managed due to one department not having a full medication list; discontinued medication recorded in either GU medicine or hospital notes as current; a dose of a non-ARV medication differing between sets of case-notes, where a department has not been notified of a medication change; doses of non-ARV medication omitted from either hospital or GU medicine case-notes; an incorrect non-ARV medication recorded in the hospital notes, for example, substitution of a medication which is being supplied by the GU medicine department; either ARV or non-ARV medication not recorded in the hospital case-notes, but listed as a current medication by GU medicine; and any non-ARV medication not recorded in the GU medicine notes which is listed as a current medication by another hospital department. Errors involving omission of current medication from one set of notes were the most frequently observed (Figure 2).
Categories and frequencies of medication recording discrepancies observed in 156 episodes of care for HIV-positive patients with dual case-notes attending for care at non-GU hospital departments. ARV=antiretroviral; GU=genitourinary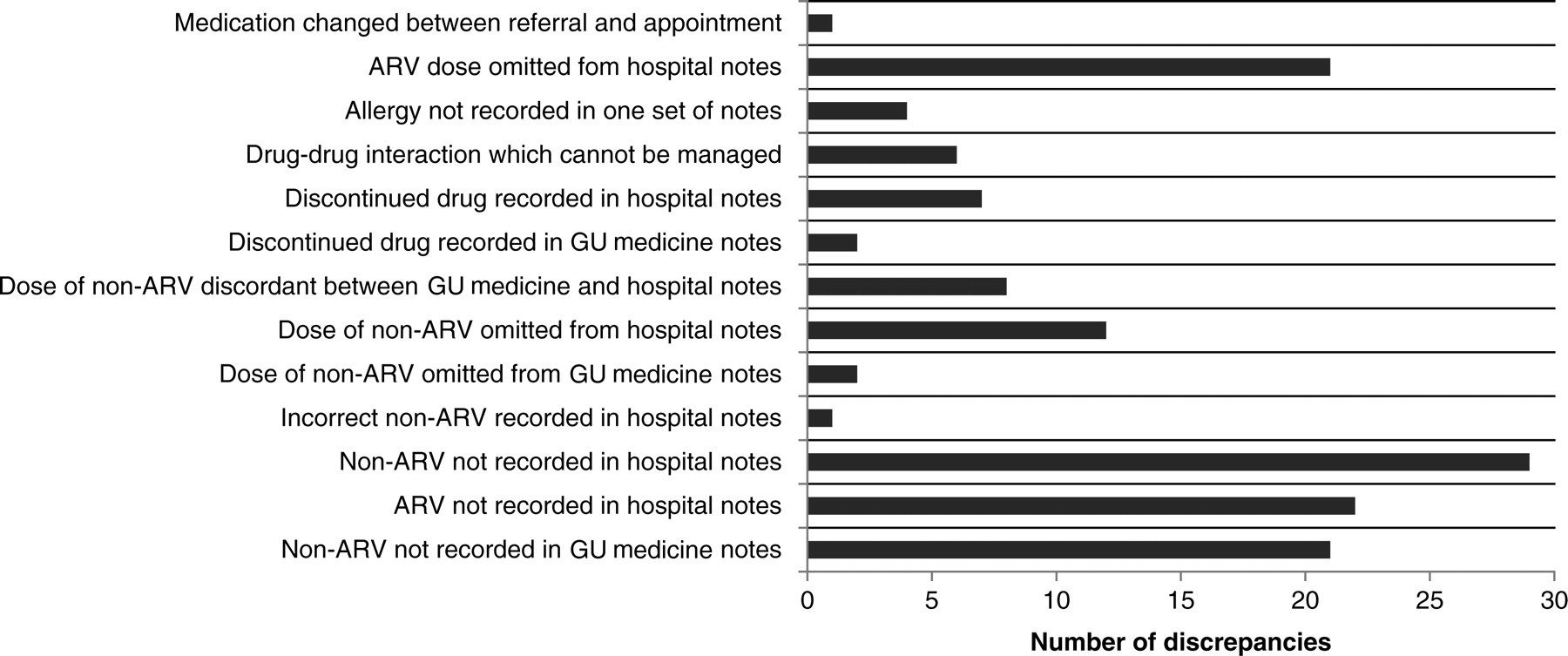
Type and frequency of errors considered to significantly affect patient care
DDI=drug–drug interaction; ARV=antiretroviral; ID=infectious diseases; GU=genitourinary; GP=general practitioner
For some of the significant discrepancies, it was clear from case-note review that the medication issue had been resolved. Where this was not evident, accurate current medication was recorded in both sets of case-notes and all teams involved in ongoing care of the patient were informed of the discrepancy, the cause and any resultant DDIs, if applicable.
A summary of discordant case-note pairs and significant discrepancies observed in 154 episodes of care from 100 HIV-positive patients, receiving HIV care via genitourinary medicine, when attending infectious disease departments compared with non-infectious disease hospital departments
ID=infectious diseases
The proportion of discrepancies with potential to have a significant impact on patient care was 8% for ID department episodes and 4% for non-ID episodes, but this difference was not statistically significant (Fisher's exact test).
DISCUSSION
The advent of combination ARV therapy has led to increased life-expectancy 6 and hence an ageing population of HIV-infected patients with co-morbidities. This has led to increased polypharmacy in patients taking ARVs, and an increase in attendances at non-HIV specialist departments. 7,8 This study has shown that HIV-positive patients can be expected to attend a broad range of hospital specialties, illustrating a clear need for accurate medication recording, enhanced pharmacovigilance among clinicians and efficient communication between relevant hospital departments, as well as with primary care.
Medication recording discrepancies were apparent in 52.6% of all care episodes evaluated. These included ARVs not being recorded in corresponding hospital notes, or medicines initiated by other departments not being recorded in GU medicine notes (Figure 2). This occurred mainly due to lack of communication between departments, for example, failure of other hospital departments to send copies of clinic letters or discharge summaries to GU medicine physicians. Similarly, updated clinic summary letters had had not been sent to other hospital departments involved in patients’ care after alteration of ARV regimens. Discrepancies of this kind were less likely to occur when a GU medicine physician had referred the patient to another department and included a current medication list with the referral letter. In seven cases, patients had been referred by their GP to a hospital department. In two of these cases, a new medication had been initiated, and the GU medicine physician did not receive a copy of the clinic summary detailing the newly initiated drug, which was sent to the GP. This issue can potentially be complicated for patients who are prescribed medications for conditions unrelated to HIV treatment by the GU medicine department rather than via their GP. For example, in one instance, a dose of a medicine was adjusted by a hospital specialist, and the GP alone was sent a copy of the clinic summary; GU medicine prescribers were therefore unaware of the change. The reluctance of some patients to disclose their HIV status to their GP can further exacerbate potential problems, as in such cases, GU medicine physicians may prescribe non-ARV medications rather than the patient's GP, in order to monitor the effect of possible interactions with their ARVs. The low rates of HIV status disclosure by patients to their GPs observed in recent years 9 will hopefully improve as HIV testing and treatment becomes increasingly normalized.
Due to the necessity to update clinical information between the different sets of case-notes, it is possible that medication recording errors were recorded in the time taken for clinic letters to be filed between clinic visits. Although this factor in itself could cause delays to clinicians receiving current clinical information from other departments, this was not the cause of the majority of discrepancies observed. A subsequent update from a recent clinic/inpatient visit after the time of this review could potentially have made case-note pairs concordant in six (7.4%) of the reported recording errors. For the majority of cases, incomplete or inaccurate medication lists in clinic summaries, discharge summaries and referral letters, as well as failure to copy summaries to relevant departments, were factors that precipitated medication recording discrepancies.
Although discrepancies were observed in over half of the care episodes evaluated, only 7.8% of episodes had a discrepancy with potential to significantly affect patient care, involving 12% of the 100 patients evaluated. At the time of case-note review, each discrepancy was analysed to assess whether any adverse impact on patient care had occurred as a result, or whether there was significant potential for adverse outcome (Table 1). Although the DDIs observed did not involve co-administration of contraindicated agents, the interactions required management in the form of closer monitoring for adverse events, clinical effect, laboratory tests or therapeutic drug level monitoring. DDIs, or inability to manage DDIs, resulted from incomplete medication recording due to the communication issues discussed above, particularly when another department initiated a new drug without informing the GU medicine department, or in the absence of current information concerning the patient's ARVs.
The prescription of incorrect medication resulted from discontinuation or switches of medication not being communicated to the relevant department. Delays in treatment optimization of a non-ARV drug resulted from dose changes not being communicated to the GU medicine physicians when they were the prescribers of a non-ARV medication, or when a hospital department wished to change a dose or a therapy, but did not have a current medication list from GU medicine. In one instance, a physician wrote in a clinic summary to a patient's GP, ‘I do not have up to date correspondence pertaining to HIV, as this is stored in separate case-notes’. Although the doctor could have requested this information from the GU medicine department, this illustrates that separate case-notes are perceived to be a significant barrier by non-GU medicine physicians.
Approximately half of the 100 HIV-positive patients reviewed in this study had attended ID as an inpatient or outpatient. At present there are several mechanisms in place to share information between GU medicine and ID departments to minimize drug errors and avoid the duplication of investigations. These include GU medicine case-notes following patients when they are admitted onto the wards, ready access for GU medicine and ID clinicians to electronic records of recent clinic letters in a confidential area of the hospital intranet, and a weekly combined ward round to discuss all HIV-positive inpatients and other jointly managed patients.
Despite these measures, our study revealed that there was no significant difference between ID and non-ID departments in their potential to have medication recording errors or significant errors. Junior doctors tend to be the main transcribers of medication lists to drug charts. The high turnover of doctors and poor awareness of the available mechanisms described are possible explanations of this finding.
Sharing of information between departments and also between primary and secondary care can be linked to national policy. For example, the NHS outcomes framework 2011/2012 outlines an indicator ‘reducing the incidence of medication errors causing serious harm’. 10 This has been incorporated into commissioning for quality and innovation payment frameworks at some centres providing services for HIV-positive patients, to improve and evaluate communication between specialist clinics and GPs.
The advent of electronic prescribing could potentially aid medication recording, by providing an accurate medication history from each prescribing episode. Any medication discontinued or initiated at a clinic visit or inpatient episode may be recorded via electronic notes created by doctors or clinical pharmacists. Such records would be available to all hospital staff involved in patient care, via a central system. The Department of Health in England is extending a programme to create an electronic Summary Care Record of medical details, accessible to authorized health-care professionals. 11 This will include details of the patient's current medication and will eventually become a national database, as no doubt will become common practice in various countries worldwide. Electronic records may help to ensure continuity between sets of hospital notes, hospital departments and also community records.
A survey on public and patient attitudes towards electronic Summary Care Records showed that most people viewed the idea positively, although a lack of awareness and understanding illustrates a clear need for appropriate public information. 12
There are confidentiality options for patients not wishing to disclose all health information to all health-care providers involved in their care. For example, a full Summary Care Record can be created, but explicit consent must be requested from the patient every time a health professional wants to access it. There is also an option for a ‘virtual sealed envelope’ option applied to selective sensitive information, for example, HIV status or sexual health information. This would mean that this selected information may not be disclosed to all health-care professionals. Although this option may be attractive to some HIV-positive patients, leading to incomplete information sharing between health-care professionals, some patients believed that the ‘sealed envelope’ option could further stigmatize the condition. 12
When improving methods of communication between hospital departments and also with primary care, it should be considered that patients may also receive treatment from private health-care providers. Care should be taken to specifically request such information from patients at the point of review and when taking medication histories.
Since the time of the audit, hospital and departmental policy has been amended so that new patients beginning treatment for HIV via GU medicine services have information concerning HIV treatment routinely filed in standard hospital case-notes, unless they choose to opt out. Existing patients are given information and asked for consent to merge information concerning HIV treatment into their standard hospital case-notes. Although this study illustrates a need for improved communication between hospital departments caring for HIV-positive patients and provides a clear argument for amalgamation of case-notes, practical issues and potential complications should be considered. For example, the location of case-note storage, particularly if GU medicine clinics take place at separate hospital sites from other specialties. Patient preference should be taken into account, allowing patients to opt out of merged case-notes, after providing sufficient information for them to make the decision. Any change in policy or procedure, such as ordering tests or medication, storage or retrieval of case-notes, should be disseminated to all appropriate staff and departments, in order to avoid any delay in patient care.
For example, patients may also have two incomplete pharmacy records, one detailing the medication dispensed under an anonymous GU medicine code and another detailing medication dispensed using the patient's name and hospital number. Ideally, when an existing patient's records are amalgamated, this information should be disseminated to pharmacy who can then merge the patient's electronic dispensing records accordingly.
Pharmacists have a key role in maintaining the medication records of inpatients, with ward pharmacists taking medication histories and undertaking medicines reconciliation at the point of admission. This routinely involves communication with primary care to generate an accurate and complete medication list. Studies involving medicines reconciliation by pharmacists in HIV outpatient settings have shown benefits such as increased recognition of DDIs and improved accuracy of medication recording. 5,13 Pharmacist involvement in outpatient clinics may therefore aid comprehensive recording of medication.
We did not assess the frequency of discrepancies of therapy records between GU medicine or hospital case-notes and patient-held records. It is policy in both the GU medicine and ID departments to provide HIV-positive patients with ‘HIV passports’ which include details of their ARVs, recent laboratory records, etc., so that the patient has more ownership of their health data and in order to try and reduce prescribing errors described here. Such policies are encouraged in national guidelines. 2 However, not all patients attending our services wish to carry their records in this manner, and we were unable to assess their accuracy in the current study.
The dual case-note system relies upon efficient communication between all departments involved in patient care, as well as stringent documentation and update of records. Accurate, clear and comprehensive medication recording is required in clinical notes, clinic summaries and referral letters. We recommend that NHS Trusts that continue to operate this system consider amalgamation of HIV care records into hospital case-notes wherever practicable, in line with national standards. Amalgamation will be of particular relevance with the introduction of electronic health-care records in the UK, 11 the primary aim of which is to ensure continuity between hospital and community records. In addition to amalgamation of case-notes, or where this is not possible or supported by patients and clinicians, improved sharing of information concerning medication may reduce the incidence of recording discrepancies. However, systems must be in place to ensure that information recorded is accurate and current, which could be managed by doctors and clinical pharmacists, ideally including communication with primary care.
Footnotes
ACKNOWLEDGEMENTS
We thank the National Institute of Health Research (NIHR – Department of Health) and the Northwest Development Agency (NWDA) for infrastructural and project support.