
Abstract
When counselling patients for postexposure prophylaxis after sexual exposure, we may need to inform them that the efficacy may be low, especially if the patient also had risks prior to the 72 hours between exposure and treatment. The use of a point-of-care test, as well as fourth generation HIV tests and HIV RNA in combination, can still miss seroconversion in the ‘eclipse’ phase of the infection as these tests are not designed to detect the earliest phase of infection.
A 29-year-old man attended our genitourinary medicine clinic requesting an HIV test. He reported a flu-like illness six weeks prior to this presentation, following which an HIV test performed at another clinic was negative. The patient's current male partner of four months was HIV-positive and was antiretroviral naive.
Initially the patient and his partner were having protected sex with condoms; however, when the patient developed what he presumed to be a seroconversion illness six weeks previously, he stopped using condoms and had several episodes of unprotected receptive anal (URAI) and oral intercourse. The last episode of URAI occurred 48 hours before presentation to our clinic. Our patient had not had sexual intercourse with any other partners in the last five months.
The Oraquick Advance rapid HIV-1 and HIV-2 antibody test (OraSure Technologies Inc, Bethlehem, PA, USA) was negative and the patient was offered HIV postexposure prophylaxis after sexual exposure (PEPSE). Serum on the day of presentation was tested by the ADVIA Centaur HIV Antigen/Antibody assay (Siemens Healthcare Diagnostics Inc, Tarrytown, NY, USA), a fourth generation HIV test, and this was also negative.
The patient adhered fully to the PEPSE regimen of tenofovir/emtricitabine once daily and lopinavir/ritonavir twice daily. 1 Despite having some nausea and diarrhoea initially, he completed the four-week course. He abstained from sexual intercourse during PEPSE and returned at the end of the course for a repeat blood test. At this point the fourth generation HIV test was positive for HIV-1 with a subsequent viral load test of 7820 copies/mL. Stored serum at presentation was tested retrospectively for HIV RNA and this was undetectable (Figure 1). A baseline resistance test showed clade B HIV-1 with no resistance.
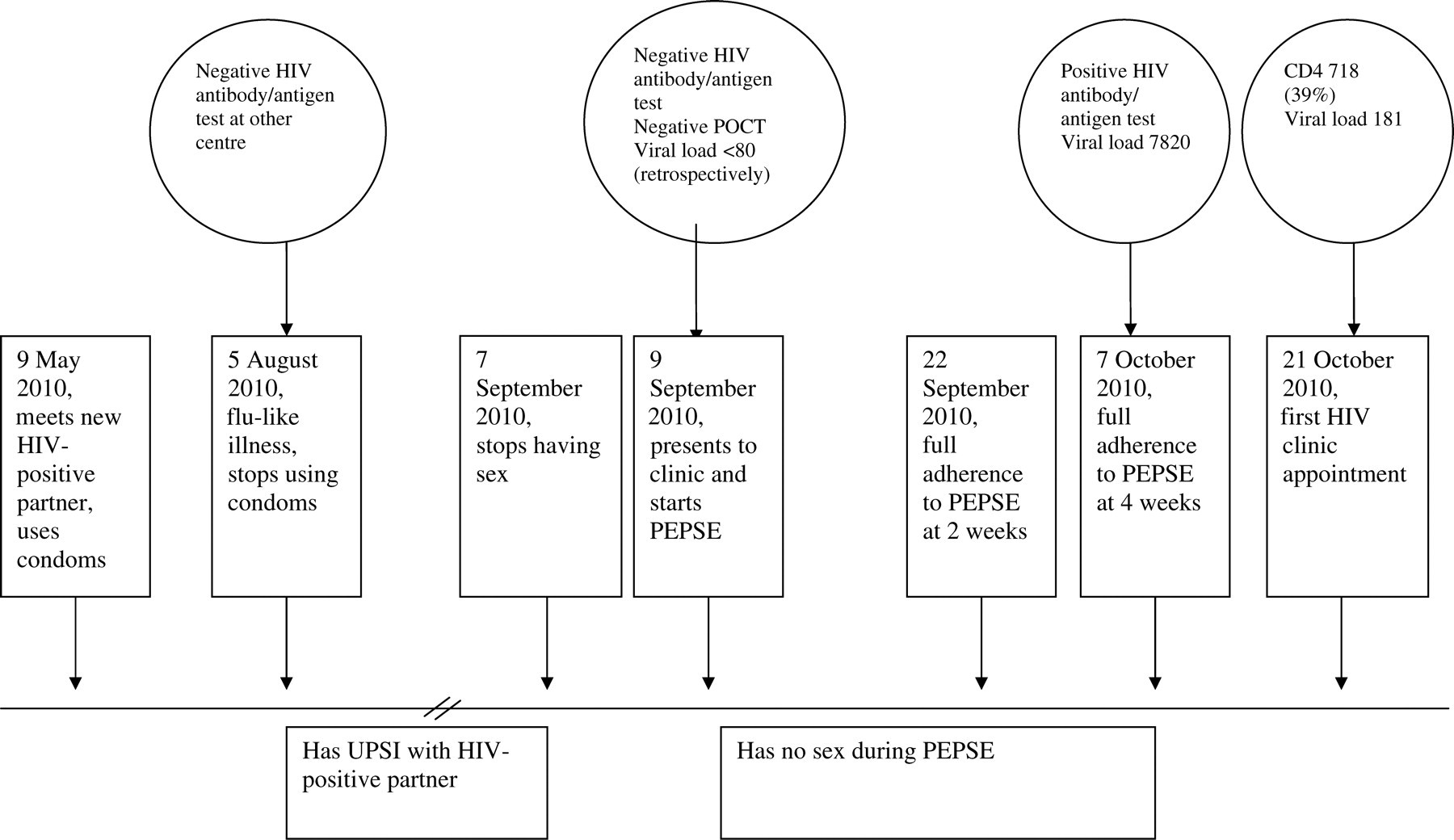
Timeline of events. POCT = point-of care testing; PEPSE = postexposure prophylaxis after sexual exposure; UPSI = unprotected sexual intercourse
DISCUSSION
The 2006 BASHH guidelines for the use of PEPSE recommend that it can be given when the individual presents within 72 hours of exposure if the source partner is HIV-positive and the individual has had URAI. 1 They also recommend that an individual undertake a rapid HIV test (point-of-care test [POCT]) prior to commencement of PEPSE. POCTs are good for detection of established HIV infection but are less sensitive than laboratory-based systems for detecting seroconversion. 2 The Oraquick POCT (a third generation test) in use at our clinic does not incorporate HIV p24 antigen testing.
POCTs are carried out in our clinic in parallel with a fourth generation venous blood test by health advisers who are trained by medical staff. A POCT is done by a finger prick capillary sample and two members of staff read the result. This together with the venous sample ensures that the rate of false-positives and false-negatives is negligible. The ADVIA Centaur HIV Antigen/Antibody (Ag/Ab) assay is carried out by fully trained laboratory staff. The laboratory takes part in the UK National External Quality Assessment Service (NEQAS) scheme 3 and has achieved full marks for HIV testing for the past 10 years. The quoted sensitivity of the test is 100% with a 95% confidence interval (CI) of 99.08–100.00% and the specificity is 99.74% with a 95% CI of 99.60–99.84%. 4
The recommended first-line assay for HIV testing is the fourth generation Ag/Ab test. 5 This shortens the window period for HIV infection to one month. Our case shows that it is difficult to identify HIV infection in high-risk patients presenting for PEPSE. Even if a fourth generation POCT had been used in our clinic, it is likely that HIV infection would have been missed. 6 Our patient tested for HIV six weeks before in another clinic, when he experienced symptoms that he believed to be those of seroconversion. Despite the test being negative, he continued to have URAI until 48 hours before presentation. He was aware of the window period and strongly believed that he had already seroconverted. In a non-randomized trial of 702 subjects receiving PEPSE, there were seven seroconverters (1%), three of whom had no further risks after PEPSE initiation, as with our patient. The other four had detectable HIV RNA at baseline or had further exposures to HIV. 7 Our patient decided to take PEPSE despite his strong belief that he was already HIV-positive in case there was a remote chance that PEPSE would be effective.
Although RNA can be detectable in blood one to two weeks after infection, HIV RNA ‘viral load’ assays are not used routinely for the detection of HIV infection due to the high rate of false-positives. 8 It is likely that infection occurred 7–21 days before he commenced PEPSE and that he was tested in the so-called ‘eclipse’ phase of infection 9 during the time that he continued to have URAI with his partner. He commenced PEPSE 48 hours after the last URAI; the earlier that PEPSE is initiated the more effective it is.
The 2006 BASHH guidelines for PEPSE also recommend that follow-up HIV testing occur at three and six months. Following the introduction of fourth generation HIV tests, our clinic adopted the policy of HIV testing at one month following exposure to HIV and therefore at the completion of PEPSE. This case illustrates the argument that earlier testing is warranted.
At the time of presentation to the clinic, the SPARTAC trial had not reported results; therefore, there were no guidelines to determine if primary HIV infection should be treated. 10 His viral load was 7820 copies/mL on the last day of PEPSE and 408 copies/mL at three months. His viral load was much lower than is seen in most seroconversion illnesses.
SUMMARY
PEPSE is not 100% effective, especially if the patient also had risks prior to the 72 hours between exposure and treatment. The use of POCTs, fourth generation HIV tests and HIV RNA tests in combination can still miss seroconversion in the ‘eclipse’ phase of the infection. These tests all look primarily for evidence of established infection and not for seroconversion.