
Abstract
In Australia, the non-occupational post-exposure prophylaxis service in Victoria (VNPEPS) maintains a database of non-occupational post-exposure prophylaxis (NPEP) use throughout the state. Through the database the service can monitor and respond to patterns of NPEP presentation, re-presentation and follow-up as well as those who test positive for HIV. We describe a cohort of NPEP individuals from the commencement of the service to 31 December 2009. During this time, 1864 individuals presented for NPEP on 2396 occasions. The majority (85%) were men who have sex with men (MSM) presenting after receptive anal intercourse (56.1%). Repeat NPEP presentations were high (17.5%) and follow-up testing at week 12 post-NPEP was low (34%). Twenty-two patients (1.2%) tested positive for HIV at baseline presentation and six patients seroconverted to HIV during follow-up. The VNPEPS has initiated strategies to encourage behaviour change for those who re-present for NPEP, and to improve rates of week 12 follow-up.
Keywords
INTRODUCTION
Non-occupational post-exposure prophylaxis (NPEP) is a 28-day course of antiretroviral medication commenced within 72 hours of a high-risk HIV exposure that aims to prevent the transmission of HIV to the exposed individual. NPEP is widely prescribed across several continents and has been available in Australia since 1998. 1–6 Australian National NPEP guidelines were first published in 2001 7 and data from a national Australian observational cohort were published in 2007. 4
NPEP has been available in Victoria, Australia, since 2000, but up until 2005 was only available at the Alfred Hospital. The NPEP Service in Victoria (VNPEPS) was established in 2005 to improve access to NPEP throughout Victoria, as well as to monitor service delivery and patient follow-up. In this paper we present an analysis of data from the VNPEPS and discuss some of the benefits of a centralized NPEP service that provides state-wide care.
METHODS
Background information
The VNPEPS commenced in August 2005 and provides coordinated statewide access to NPEP for those exposed to HIV in the community. The service is funded by the Department of Health, Victoria, and operates on a hub and spoke model. The central administration of the service (the hub) is located at the Alfred Hospital and is staffed by an infectious diseases physician (0.2 EFT), clinical nurse consultant (CNC) (0.8 EFT) and clinical psychologist (by consultation). The spokes of the service include general practice clinics with a high caseload of patients who are men who have sex with men (MSM), sexual health clinics, infectious diseases units and emergency departments at selected hospitals in Victoria. There are currently 13 spoke sites in metropolitan Melbourne and five in regional centres of Victoria.
Central to the service is the CNC and the NPEP phoneline. The role of the CNC includes coordinating the supply of NPEP medications, monitoring patient follow-up, coordinating a service response for those who are repeat NPEP presenters, monitoring NPEP prescriptions for compliance with national NPEP guidelines and coordinating the NPEP phoneline.
The NPEP phoneline is staffed by NPEP specialist registered nurses. Following a known or a potential HIV exposure, an individual may call the NPEP phone line where, if the exposure is assessed to be high risk, the caller is triaged to an NPEP spoke site. Individuals may also go directly to a spoke site for an NPEP consultation. At the initial NPEP consultation a risk assessment is conducted, baseline testing for HIV and other blood borne viruses is performed and, where indicated, a seven-day NPEP starter pack (two or three drugs) is dispensed. NPEP is prescribed according to the state of Victoria NPEP guidelines, which have been modelled on national Australian guidelines. 8
The individual returns within seven days to collect their baseline test results, undergo screening for sexually transmitted infections (STIs) and to receive their remaining 21-day supply of NPEP. Follow-up HIV testing is then recommended between weeks 4–6 and at week 12. Individuals who have not returned for HIV testing at week 12 are either contacted directly by the NPEP CNC (the Alfred Hospital patients) or a list of overdue patients’ initials (first 2 characters of surname and first name) and dates of birth (DOB) is sent to individual spoke clinics to stimulate follow-up reminders to be sent by the clinic.
Data collection
Data from all patients who present for NPEP are collected by the practitioner at baseline presentation and follow-up. Verbal consent is required to include coded identified data (first 2 characters of surname and first name along with DOB) on the data form. This process has been approved by the Alfred Research and Ethics Committee.
Repeat presenters
A repeat presenter is anyone who is identified on the NPEP database (by matching initials and DOB) as having had more than one NPEP presentation. Those who are identified as having presented for NPEP three or more times in a two-year period are recommended for the ‘Repeat Presenters Model of Care’ intervention. This involves: (1) provision of a summary of the individual's NPEP history to the doctor who prescribed NPEP; (2) the recommendation that all subsequent care for NPEP be at a single nominated spoke clinic; and (3) a recommendation that the individual be referred for psychological assessment and counselling around HIV risk reduction and enhancing sexual safety.
Statistical analysis
All patient data are entered and maintained in a Microsoft Access database. Descriptive statistics were used to describe patient demographics, HIV exposure types, prescribing patterns, repeat presentations and patient follow-up. Time between repeat presentations was calculated as the difference in time between one consultation and the next. A rank-sum test was performed for time between presentations using STATA (Stata Statistical Software, Release 8.0, College Station, TX, USA).
RESULTS
Patient characteristics
The number of annual presentations for NPEP has almost doubled from 324 in 2005 to 607 in 2009 (Figure 1). Between August 2005 and December 2009, a total of 1864 individuals presented for NPEP on 2396 occasions. The majority of presentations were by men (94%). The average age at presentation was 34.7 years for men (range 14.4–83.5) and 32.4 years for women (range 15.0–62.0). MSM represented 84.7% of all presentations for NPEP and 97.0% of all men. Sixty-eight (2.8%) presentations were following sexual assault. Twenty-two (1.2%) individuals were found to be HIV antibody positive at baseline presentation and six individuals were documented to seroconvert to HIV after receipt of NPEP. Three of these were identified at a subsequent NPEP baseline presentation but had not had any HIV testing between the two NPEP presentations. The other four were identified through follow-up HIV testing (weeks 4, 6, 16 and 26). Of these, three reported significant other risk exposures either before or after receipt of NPEP and therefore cannot be classified as NPEP failures.
Presentations for non-occupational post-exposure prophylaxis in Victoria, Australia, January 2000–December 2009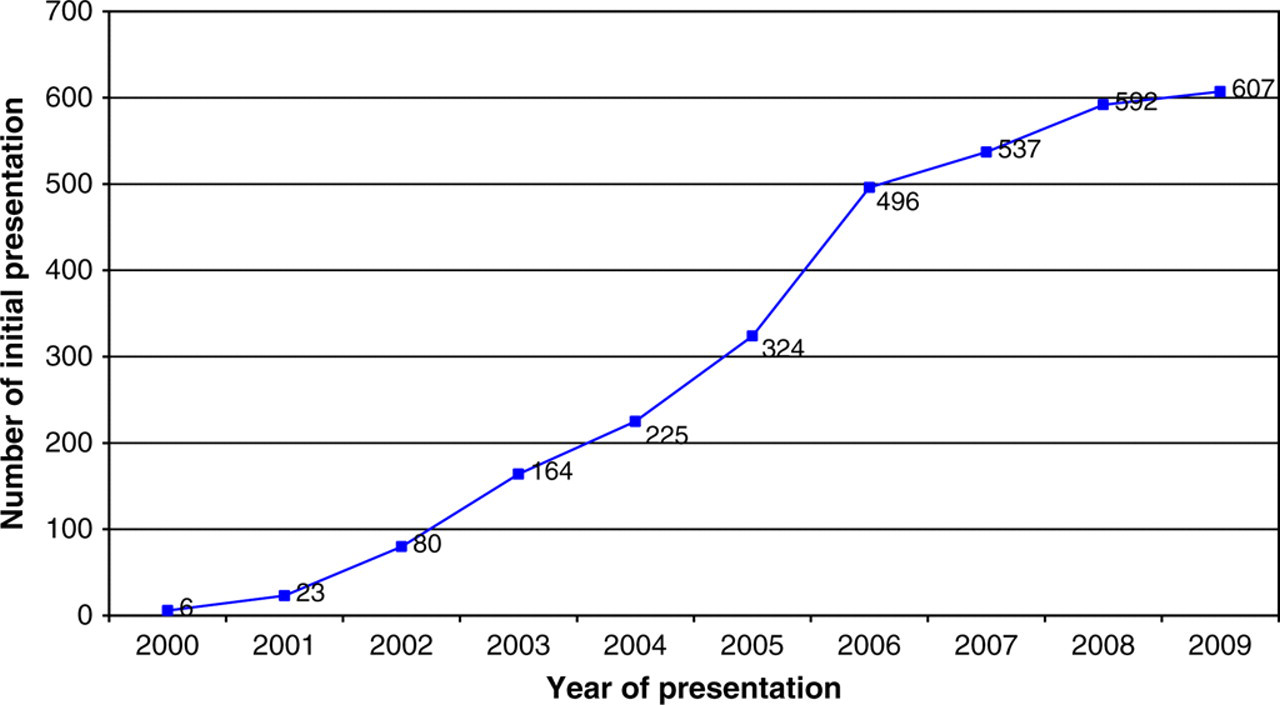
Exposure type
Characteristics of exposures that led to non-occupational post-exposure prophylaxis (NPEP) consultation
*Sexual exposures only (n = 2227)
†Multiple responses possible
‡For those prescribed NPEP and for whom data on time from exposure to presentation are complete (n = 2047)
NPEP prescriptions
Non-occupational post-exposure prophylaxis (NPEP) regimens prescribed
The number of prescriptions for NPEP that fall outside of the national NPEP guidelines has decreased over time. A prescribing policy was developed by the VNPEPS in November 2007 when it became apparent that in some cases NPEP was being prescribed for exposures that did not warrant prophylaxis or a triple-drug regimen was being prescribed where a two-drug regimen was indicated. A phone call to the prescriber in these cases by the NPEP physician and education sessions at spoke clinics has improved adherence to guidelines with the target of 90% being achieved overall.
Re-presenters
Between August 2005 and December 2009 a total of 326 patients (17.5%) presented for NPEP on more than one occasion, with a range of 2–11 presentations. The majority was MSM (313, 96.0%). One hundred and ten patients (33.7%) had three or more presentations, and 19 (5.8%) presented five or more times. For all patients presenting in 2009 (n = 547), 162 (29.6%) had previously had NPEP. In addition, 47 (8.6%) received NPEP on more than one occasion in this 12-month period; 36 received NPEP twice, nine received NPEP three times and two received NPEP four times in 12 months. All were MSM.
Time between presentations for NPEP reduced with increasing number of presentations. Median time between presentations for those who presented between two and four times was 252 days, whereas for those who presented five or more times the median time was 140 days. This was statistically significant (P < 0.001).
Forty-three individuals (all MSM) were identified as eligible for the repeat presenter intervention programme between January 2008 (when the intervention began) and December 2009. All were offered referral to the VNPEPS clinical psychologist; however, only 13 patients were formally referred by their prescribing doctor. Two individuals preferred in-house counselling at the clinic where they accessed NPEP and one individual went into a drug and alcohol detoxification centre. It is not possible to accurately determine the rate of uptake of the model by patients as in approximately one-third of cases there was no feedback from spoke clinics.
Follow-up
Follow-up for those who were prescribed NPEP was 86% at week 1, 47% at week 4/6 and 34% at week 12. Follow-up for week 12 ranged from 10% to 60% between clinics.
DISCUSSION
Since the introduction of the VNPEPS the prescription of NPEP has almost doubled, from 324 occasions in 2005 to 607 in 2009. The number of people presenting for repeat NPEP is also increasing over time. Notably, the majority of presentations are MSM with high-risk sexual exposures for which NPEP is prescribed according to national NPEP guidelines. 8 Follow-up rates at week 12 are low and range from 10% to 60% for individual clinics. Twenty-two patients (1.2%) have tested HIV-positive at baseline and six patients have seroconverted to HIV post-NPEP use.
An increase in NPEP presentations has occurred in many countries following publication of NPEP guidelines and/or NPEP publicity and promotion. 2,5,9,10 Increased availability of NPEP in France resulted in widespread NPEP use for low-risk sexual exposures. 11 In Australia, NPEP use reported in the HIM cohort (a cohort of Sydney-based MSM) increased from 2.9/100 person-years (PY) in 2002 to 7.1/100 PY in 2007. 9 The substantial increase in NPEP presentations in Victoria is thought to be a result of the combination of improved access and increased awareness of NPEP in the MSM community. Despite this increase, NPEP use in Victoria remains confined to those with the highest risk exposures.
The rates of repeat presentation in our cohort are high and are increasing over time. Of all the patients seen since the VNPEPS began in 2005, 17.5% have had NPEP on more than one occasion. This is similar to the number who reported prior NPEP use (14%) in the Australian cohort study. 9 Although almost a third of individuals who presented in 2009 had previously used NPEP, only 47 (8.6%) did so more than once in the 12 months of 2009. This is lower than the rate of repeat presentation reported within a 12-month period in San Francisco, CA, USA (17.5%). 12 Repeat NPEP presentation rates in Europe are significantly lower with rates of 6%, 4.3% and 2.5% reported in Denmark, Switzerland and Amsterdam, the Netherlands, respectively. 2,3,5 Reasons for this are not immediately apparent. It is reassuring to note that despite high rates of repeat presentation to the VNPEPS, a recent study did not find an association between number of presentations for NPEP and HIV seroconversion. 13
Our Repeat Presenter Model of Care was developed in response to concern about the increasing number of repeat NPEP presentations in Victoria. In a high caseload health service, New South Wales, a mandatory counselling referral is automatically generated following a third or subsequent NPEP presentation to that health service within a 12-month period. 14 In the UK, prescription of a second or subsequent course of NPEP in a 12-month period is contingent upon the patient attending for risk reduction counselling. 15 Our model strongly encourages referral to a clinical psychologist; however, only approximately one-third of patients agreed to participate. This is likely to be due to the fact that, unlike the UK, psychology attendance is not compulsory for repeat presenters and NPEP continues to be prescribed for high-risk situations.
The VNPEPS CNC coordinates an active follow-up system for the whole NPEP service. Although follow-up HIV testing is recommended at one, three and six months after NPEP, 6,8 the VNPEPS only performs active follow-up at three months after NPEP, as evidence suggests that follow-up at six months is impractical and that testing at three months should detect all but a very small proportion of cases of HIV seroconversion. 16
Individuals seen at the Alfred Hospital are contacted directly (by phone or SMS) and for those seen at spoke clinics a list of overdue patients’ initials and DOBs is sent. Despite this, rates of return for repeat HIV testing at three months are disconcertingly low, although they are not dissimilar to rates published in Western Australia (22.3%). The Australian cohort study did not record three-month follow-up but follow-up at six months was less than 25%. Follow-up rates reported in Europe are higher with 51% follow-up at three months reported in both Switzerland and Denmark 2,5 and 85% in Amsterdam at three months. 3 San Francisco also achieved high rates of follow-up with 75% returning at six months. 12 However this was in the setting of a clinical trial with intensive study visits at weekly intervals. Some individuals in Victoria will have had their follow-up HIV testing at another clinic not associated with the VNPEPS, thus our data may underestimate the true number who complete follow-up. The VNPEPS has intensified efforts to improve follow-up in 2010 with initiatives such as more regular telephone contact and SMS reminders for Alfred Hospital patients; preliminary results are encouraging. In addition, a study to investigate the impact of rapid HIV testing on follow-up rates is planned to commence in early 2011. HIV rapid testing is not currently available in Australia.
Six individuals were identified as having seroconverted to HIV during the follow-up period and three of these disclosed other risk factors during follow-up, suggesting NPEP failure was less likely. Two of the seroconverters were partners and had both used NPEP five months previously following a high-risk exposure to a casual partner known to be HIV infected. Neither had any recommended follow-up testing and they both tested positive for HIV at a subsequent NPEP presentation. It is not known if there were other high-risk exposures in this period; however, a UK study reported that MSM on NPEP had previous risks for which NPEP was not sought. 17 Without this information it is not possible to determine if they were NPEP failures or not. The final seroconverter denied any other risk events other than the exposure that led to NPEP prescription and therefore must be considered a probable NPEP failure. This represents 0.04% of NPEP courses prescribed.
Our finding that 22 individuals were HIV seropositive at baseline (1.2%) was surprising. This rate is higher than the rate reported in the San Francisco study (0.75%) 12 and almost three times the reported rate of 0.43% (7/1601) in the Australian cohort study. 4 This underscores the importance of baseline HIV testing and the need for prompt follow-up of baseline results to identify those who are already HIV infected and for whom a two-drug NPEP prescription could jeopardize future treatment options. It also supports recent findings of high rates of undiagnosed HIV infection in MSM in Victoria who undertake at-risk behaviour. 18
CONCLUSION
The VNPEPS maintains a centralized database which has the benefit of capturing detailed data on many aspects of NPEP use throughout the whole of Victoria and assists the service to identify where quality initiatives are needed. In this regard the VNPEPS is unique in Australia, as although some other states maintain databases, we have the advantage of a fully coordinated service with clinical staff who provide support and feedback to prescribers at NPEP clinics. We have previously targeted prescribing practices with a resulting decrease in inappropriate prescriptions. Currently, we are focused on ways to improve follow-up rates and continue to recommend psychological support to those who demonstrate their ongoing high-risk behaviour through multiple NPEP presentations.
Footnotes
ACKNOWLEDGEMENTS
The authors acknowledge clinic staff and patients of affiliate spoke clinics for provision of data and the Alfred Hospital Infectious Diseases Epidemiology and Data Unit for data management.