
Abstract
This systematic review was conducted to determine the effects of self-help interactive computer-based interventions (ICBIs) for sexual health promotion. We searched 40 databases for randomized controlled trials (RCTs) of computer-based interventions, defining ‘interactive’ as programmes that require contributions from users to produce personally relevant material. We conducted searches and analysed data using Cochrane Collaboration methods. Results of RCTs were pooled using a random-effects model with standardized mean differences for continuous outcomes and odds ratios (ORs) for binary outcomes, with heterogeneity assessed using the I 2 statistic. We identified 15 RCTs of ICBIs (3917 participants). Comparing ICBIs to minimal interventions, there were significant effects on sexual health knowledge (standardized mean difference [SMD] 0.72, 95% confidence interval [CI] 0.27–1.18); safer sex self-efficacy (SMD 0.17, 95% CI 0.05–0.29); safer-sex intentions (SMD 0.16, 95% CI 0.02–0.30); and sexual behaviour (OR 1.75, 95% CI 1.18–2.59). ICBIs had a greater impact on sexual health knowledge than face-to-face interventions did (SMD 0.36, 95% CI 0.13–0.58). ICBIs are effective tools for learning about sexual health, and show promising effects on self-efficacy, intention and sexual behaviour. More data are needed to analyse biological outcomes and cost-effectiveness.
INTRODUCTION
Poor sexual health is a major public health challenge, and face-to-face interventions have had mixed success. 1–4 Sexual health may not be addressed in health-care encounters because of pressure on health services, and reservations about raising complex and potentially sensitive topics. 5
Interventions delivered via the Internet or mobile phones offer advantages since they can be accessed privately and at users’ convenience. 6 Programmes can be tailored for individual needs 7,8 thus combining the scalability of a public health intervention 8 with the personalization of face-to-face interventions. However, it is not known whether interactive computer-based interventions (ICBIs) are effective for sexual health promotion, nor how they compare with face-to-face interventions.
METHODS
We used Cochrane Collaboration methods for conducting systematic reviews. We searched 27 electronic databases (including CENTRAL, DARE, MEDLINE, EMBASE, Cumulative Index to Nursing & Allied Health Literature, British Nursing Index and PsycINFO); five databases of grey literature for unpublished work; eight trials registers; hand-searched reference lists of published studies; and contacted study authors. 9 All databases were searched from their start date to November 2007, with no language restriction. The search strategy comprised three overlapping concepts: (1) randomized controlled trial (RCT) study design, (2) computer/Internet-based applications and (3) sexual health. We included studies involving participants of any age, gender, sexual orientation, ethnicity or nationality.
Eligible interventions were defined as interactive computer-based programmes that provide information and one or more of the following: decision support, behaviour-change support, or emotional support for health issues. Interventions had to be interactive, defined as requiring contributions from users which altered pathways within programmes to produce tailored material and feedback that was personally relevant. 7 We defined sexual health promotion as ‘strategies for improving the sexual health of the population by providing individuals, groups and communities with the tools to make informed decisions about their sexual wellbeing’. We included trials of computer-based interventions which are designed for self-help, excluding interventions designed to optimize health care once in a health-care setting and interventions delivered with expert facilitation (e.g. by teachers or health professionals).
We downloaded all citations identified by the search into Reference Manager software. Two review authors independently screened titles and abstracts for relevance, obtained the full text of any candidate studies, and extracted data. We contacted authors where necessary. We used Review Manager software for meta-analyses.
We recorded the quality of the randomization and concealment of allocation procedures, rating these (A) adequate (B) unclear or (C) inadequate sequence generation and/or concealment. Studies rated C were excluded completely from analysis because of the high risk of bias. We recorded other quality criteria (see Table 1, available online only at:
We sought numerators and denominators for dichotomous variables and means and standard deviations for continuous variables, calculating missing standard deviations from F statistics where available. Where appropriate, we pooled the results of RCTs using a random-effects model using standardized mean differences (SMDs) for continuous outcomes and odds ratios (ORs) for dichotomous outcomes. We comment on the size of SMDs using Cohen's rules of thumb, judging 0.2 to be ‘small’, 0.5 to be ‘moderate’ and 0.8 a ‘large’ effect. 10 We assessed heterogeneity using the I 2 statistic. We calculated estimates of practical significance by multiplying baseline standard deviations for knowledge, self-efficacy and intention (taken from the largest studies with available baseline data) by the combined effect size for these outcomes derived from meta-analysis.
We analysed separately studies that compared ICBIs to minimal intervention (group 1), and those that compared intervention to non-computerized, face-to-face sexual health education (group 2). Separate meta-analyses were also conducted for type of outcome (knowledge, self-efficacy, intention, sexual behaviour and biological outcomes; see Tables 2 and 3, available online only at:
RESULTS
The search generated 11,376 citations, with 156 citations identified for possible inclusion. One hundred and thirty-nine citations were excluded because they were not RCTs and/or did not meet our definitions of ICBI or sexual health promotion (see flow chart). Fifteen studies described in 17 papers therefore met the criteria for inclusion (Table 1). The total number of participants for whom outcome data were available was 3917. In total, 1602 participants received an ICBI: these were compared in two-arm or three-arm trials with 1629 who received minimal interventions, and 426 who received face-to-face sexual health interventions.
Three studies were conducted entirely online, 12–14 with 12 studies relying on some face-to-face contact with the researchers. The target populations were diverse, and intervention designs drew on a large variety of theoretical models (Table 1).
Eight interventions focused on HIV prevention, 12,14–20 three on sexually transmitted infection (STI) including HIV, 21–23 two on preventing unwanted pregnancy, 24,25 one on responsible sexual behaviour, 26 and one on preventing sexual assault and enhancing positive dating experiences. 27
The programmes produced material that was personally relevant in a variety of ways, the most common being feedback on knowledge tests 13,15,17,19,22,23,25,28 and feedback on virtual decisions. 20,21,26,27,29 The programmes made imaginative use of multimedia capability, for example, games, 15 stories, scenarios and simulations, 12,14–16,27 virtual characters with choices to make, 21,24 interactive virtual dates, 20,23 conversations with the computer or virtual characters 13,16,17,24,26 and animations, cartoons and music. 25 Some programmes provided the stimulus for ‘real world’ activities, including discussing answers to knowledge tests with others, 24 practising putting a condom onto a penis model, and practising communication and negotiation skills. 17
All included studies stated that the participants had been randomly allocated, with only five studies clearly reporting adequate sequence generation and concealment of allocation (rated ‘A’) (see Table 1). It was not possible to judge the adequacy of procedures in the remainder, so these were rated ‘B’. Retention at follow-up was variable (Table 1).
Tables 2 and 3 show which outcomes were selected for meta-analysis for groups 1 and 2 studies, respectively. No studies reported economic outcomes.
Comparison 1: are ICBIs effective in comparison to minimal interventions?
We combined outcomes from group 1 studies to address the question of whether ICBIs have an effect on sexual health outcomes.
Meta-analysis of six studies that reported sexual health knowledge showed an SMD of 0.72 (95% confidence interval [CI] 0.27–1.18), which is a moderate positive effect (Figure 1). The I
2 statistic (91%) showed substantial heterogeneity, reducing confidence in this result. One additional study showed no statistically significant differences in knowledge,
22
and another showed improvement in knowledge,
26
but data suitable for analysis were not available.
ICBI versus minimal intervention: knowledge. ICBI, interactive computer-based intervention; CI, confidence interval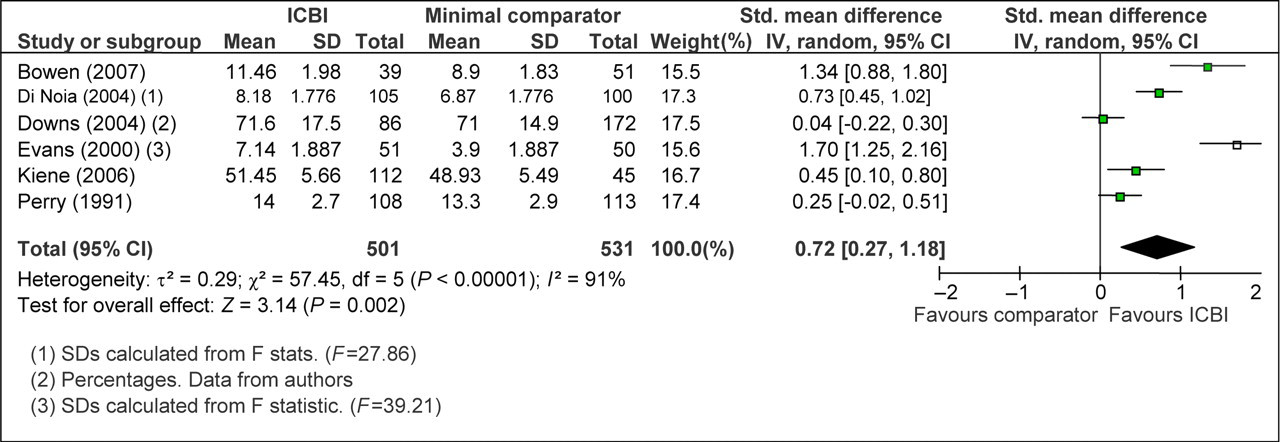
We combined data from six studies that reported data on self-efficacy (Figure 2), giving an SMD of 0.17 (95% CI 0.05–0.29), which is a small positive effect. One additional study reported no difference between intervention and control for self-efficacy, with data unavailable.
20
ICBI versus minimal intervention: self-efficacy. ICBI, interactive computer-based intervention; CI, confidence interval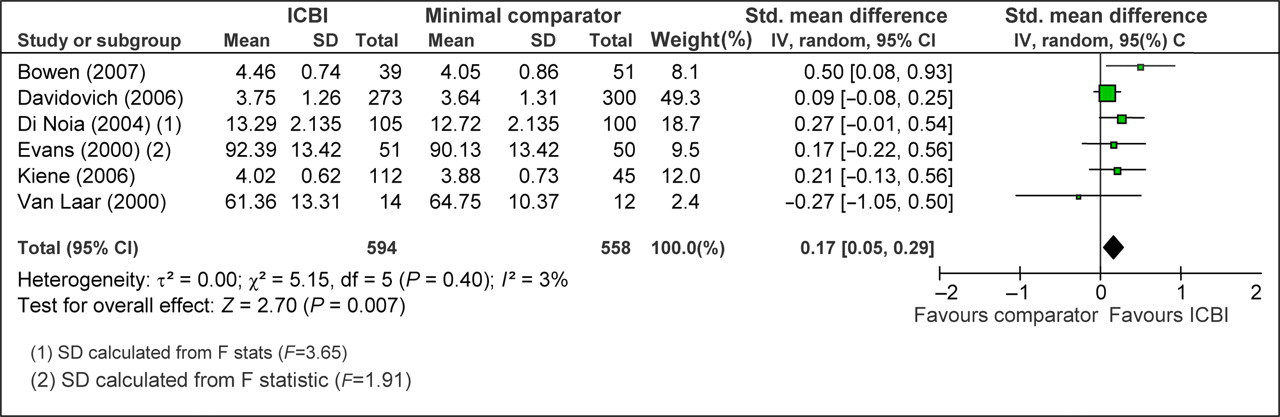
We combined data from three studies that measured intention (Figure 3), giving an SMD of 0.16, (95% CI 0.02–0.30), which is a small positive effect. One additional study reported no statistically significant difference between intervention and control for intention,
20
and another reported condom use readiness to change at two months,
22
but data for analysis were not available.
ICBI versus minimal intervention: intention. ICBI, interactive computer-based intervention; CI, confidence interval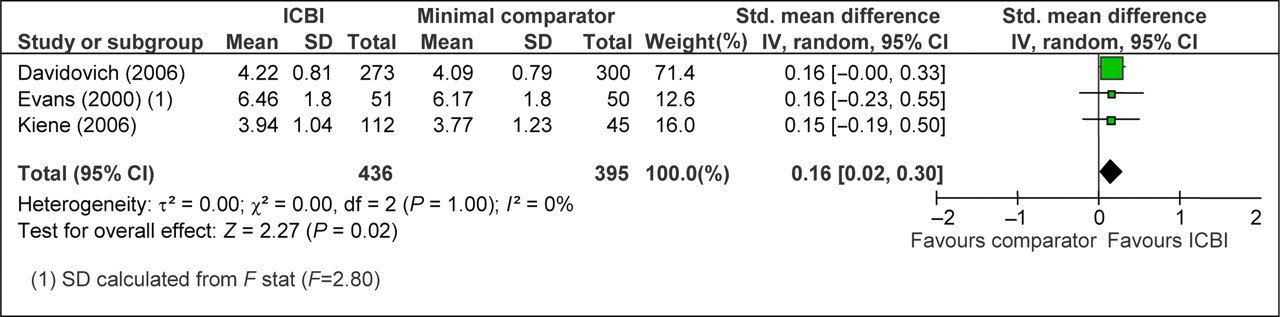
We combined data from three studies that measured sexual behaviour as a dichotomous outcome (numbers of events) (Figure 4). The outcomes combined were sexual victimization,
27
negotiated safety or condom use,
12
and condom use in the last three months ‘every time with every partner’.
21
We calculated the number of participants who did not experience sexual victimization, since this represents a desirable outcome. The OR was non-significant (OR 1.54, 95% CI 1.00–2.38). Data were unavailable for Jenkins et al. (condom use with risky partners).
22
ICBI versus minimal intervention: sexual behaviour (dichotomous). ICBI, interactive computer-based intervention; CI, confidence interval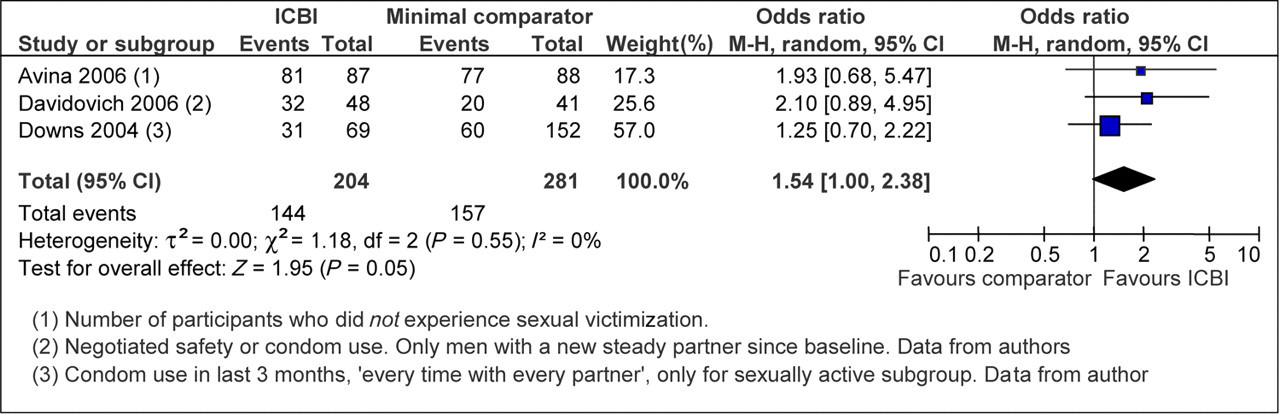
Two studies measured sexual behaviour on continuous measurement scales: condom use in the last 30 days,
17
and protected anal sex.
20
Data were unavailable for the latter; data from the former gave an SMD of 0.61 (95% CI 0.11–1.11), showing a moderate effect. We converted this SMD into an OR to combine it with the other studies reporting sexual behaviour outcomes (those in Figure 4). This resulted in a combined OR of 1.75 (95% CI 1.18–2.59; Figure 5), which is a statistically significant effect on sexual behaviour.
ICBI versus minimal intervention: sexual behaviour (combined). ICBI, interactive computer-based intervention; CI, confidence interval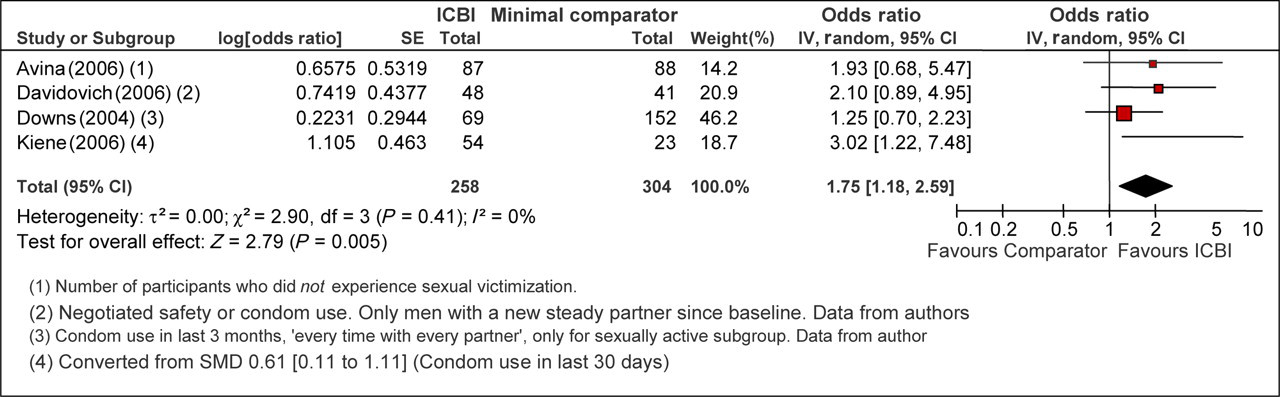
Two studies measured biological outcomes: HIV antibody serology 19 and vaginal Chlamydia DNA. 21 There were no new diagnoses of HIV in Perry et al. 19 so meta-analysis could not be undertaken. Data from Downs et al. 21 gave an OR of 0.74 (95% CI 0.25–2.14), which was a non-significant effect on Chlamydia acquisition. There were therefore insufficient data to draw conclusions about the effect of ICBIs on biological outcomes.
Comparison 2: are ICBIs as effective as face-to-face sexual health interventions?
We combined outcomes from group 2 studies to address the question of whether ICBIs for sexual health are as effective as face-to-face interventions.
Two studies reported on sexual health knowledge: the first study compared ICBIs with stress training
19
and the second with lectures.
16
Meta-analysis showed an SMD of 0.36 (95% CI 0.13–0.58), which is a small effect size (Figure 6). Two further studies reported no differences between ICBIs and a lecture with the same content,
24
and ICBIs and face-to-face counselling,
22
but data were not available to include in the meta-analysis.
ICBI versus face-to-face intervention: knowledge. ICBI, interactive computer-based intervention; CI, confidence interval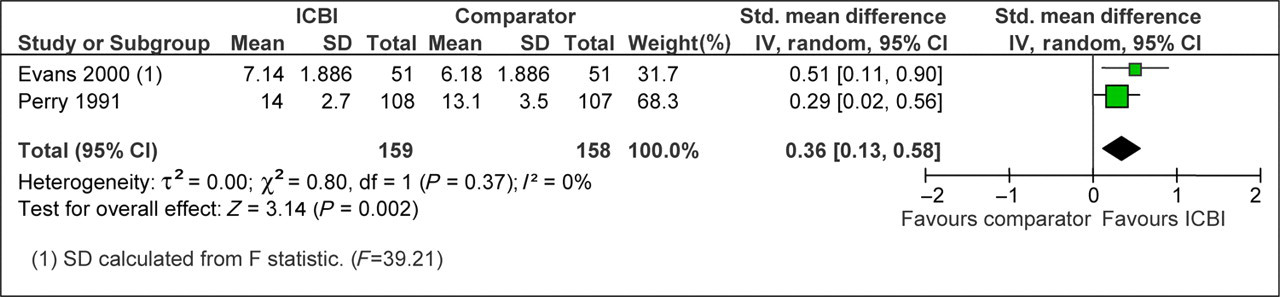
To derive an estimate of self-efficacy, we calculated the standard deviation from an F statistic for Evans et al., 16 finding no difference between ICBIs and a lecture (SMD = 0.38: 95% CI −0.01 to 0.77). However, this was a small study (n = 102 at follow-up), reducing confidence in the result.
One study in group 2 reported condom use intention.
16
We calculated an SMD from an F statistic, with results indicating greater intention after ICBIs than after a lecture (SMD = 0.46: 95% CI 0.06–0.85), which is a moderate effect size. However, the study was small (n = 102 at follow-up), reducing confidence in the result. One study reported readiness to change condom use at two months,
22
but data were not available for inclusion. Data were not available to analyse sexual behaviour or biological outcomes (Figure 7).
Computer-based interventions for sexual health promotion: Cochrane systematic review and meta-analysis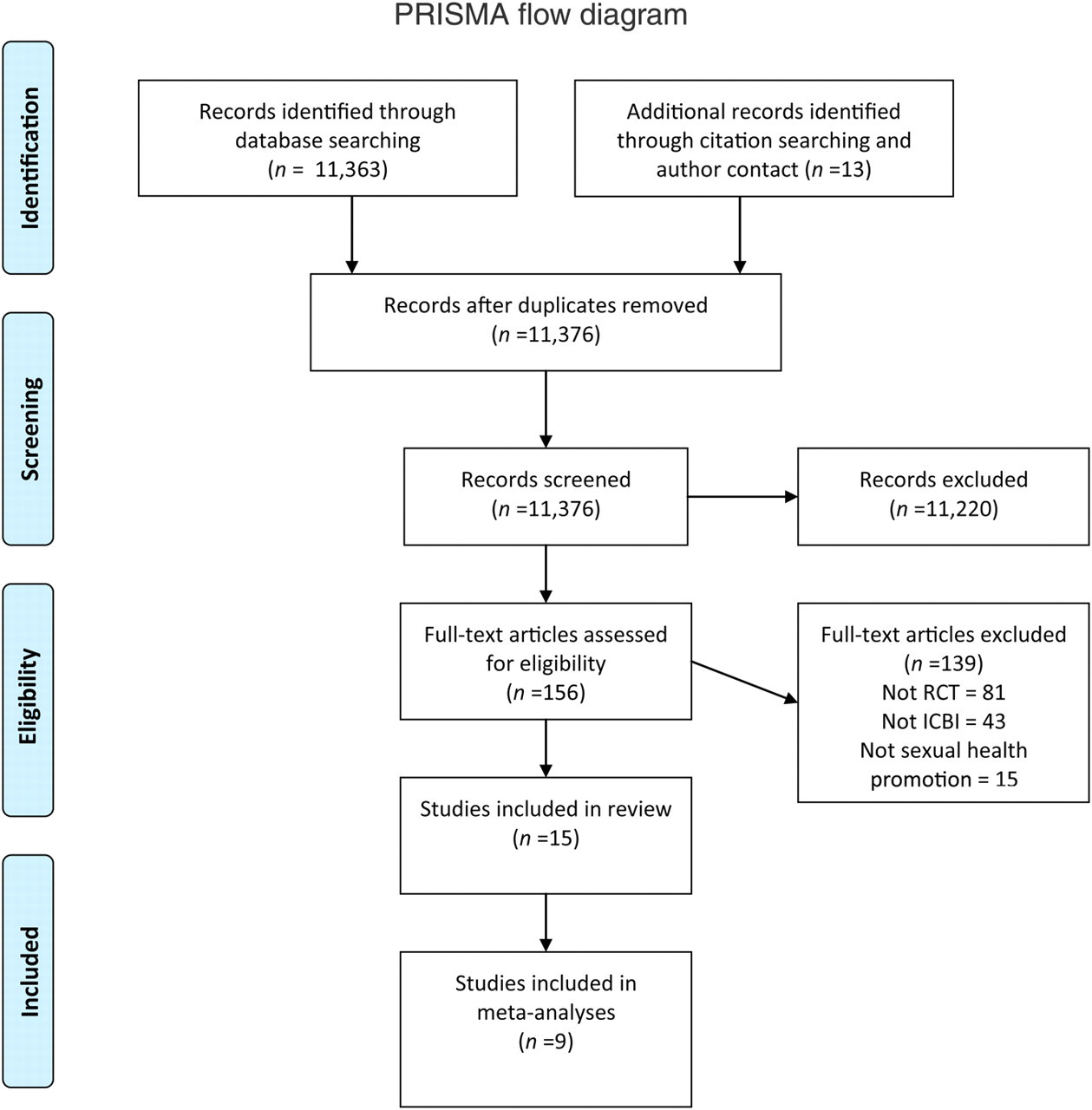
Estimates of practical significance
Standardized mean differences give an idea of the strength of evidence, but do not convey what these results might mean in practice. For knowledge, an SMD of 0.72 (Figure 1) translates into an increase in score from 6.75 to 8.50 on a 12-item true/false HIV knowledge test. 23 For self-efficacy, an SMD of 0.17 (Figure 2) translates into an increase in adolescents’ confidence in using a condom correctly from 4.10 at baseline to 4.18 measured on a five-point Likert scale. 23 For safer sex intention, an SMD of 0.16 (Figure 3) translates into an increase in students’ likelihood of using condoms and engaging in preparatory condom use behaviours from 3.77 to 3.96 on a five-point Likert scale. 17
DISCUSSION
This systematic review shows that ICBIs for self-help have small to moderate effects on sexual health knowledge, self-efficacy, intentions and behaviour. ICBIs seem at least as good as face-to-face interventions for knowledge acquisition. More data are needed to be confident about the effects on sexual behaviour, and there were insufficient data to draw conclusions about important outcomes such as STIs or unwanted pregnancies, and cost-effectiveness.
Our findings are compatible with systematic reviews of computer-based interventions specifically for HIV prevention, 30 for chronic disease, 31 for alcohol harm reduction 32 and for smoking cessation 33 which also demonstrated small to medium effects on outcomes.
Our review was conducted rigorously with careful delineation of inclusion and exclusion criteria. One strength of our review is the inclusion of studies which addressed social and emotional dimensions of sexual health as well as physical problems such as STIs, and our use of a clear theoretical rationale for the selection and combination of outcomes. There are limitations in the quality and reporting of some of the primary studies, and heterogeneity in some of our analyses reduces the level of confidence in these results.
Computer-based interventions are feasible for a variety of populations, and the gains in knowledge suggest that ICBIs can usefully contribute to sexual health education.
However, further work is required before commissioning interventions, including mapping of the pathways of sexual health behaviour change, testing the likely active components of ICBIs, 34 testing the mode of delivery (e.g. facilitated access in comparison with self-help programmes) and large, well-conducted trials to provide data on behaviour change, biological outcomes, cost-effectiveness and unforeseen adverse effects.
Footnotes
ACKNOWLEDGEMENTS
All authors declare that (1) none of the authors have support from any companies for the submitted work; (2) none of the authors have relationships with any companies that might have an interest in the submitted work in the previous three years; (3) their spouses, partners or children have no financial relationships that may be relevant to the submitted work; and (4) JVB, EM, IN and GR are members of a team which has developed an interactive computer-based intervention for sexual health, currently under evaluation in an online trial (funded by the Medical Research Council, 2008–11). The results of this trial are not yet available. JVB's salary (2006–07) was funded through a part-time post-doctoral research fellowship from the North Central London Research Consortium, UK. The Consortium had no role in the study design, data collection, interpretation of data, writing the report or decision to submit the article for publication. All authors were fully independent, with no external bodies influencing the conduct of this research.
This paper is based on a Cochrane review first published in The Cochrane Library 2010, Issue 9. We wish to thank the Cochrane Consumers and Communication Review Group editors and staff, particularly Professor Adrian Edwards, Dr Sophie Hill and Dr Megan Prictor.
The full search results and dataset are available from
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.