
Abstract
Our management of anogenital warts was audited. By case-note review 95% were clear of original warts by three months (assuming wart clearance if patients stopped attending). However, by confirmed outcome (documented in case-notes or verified by telephone) only 81% were clear. The main reason for failure was inconsistent patient attendance. Subsequently, clinic staff were advised to emphasize the importance of regular treatment. A second audit was performed after 12 months. By case-note review 127/134 (95%) had achieved wart clearance, but by confirmed outcome only 74/89 (83%) were clear (P = 0.004). More men (89%) achieved clearance than women (80%). Again, the main reason for failure was inconsistent attendance. There are few data of outcomes in clinical practice at three months. Auditable outcome measures should be challenging yet achievable. Perhaps 90% clearance at three months is not achievable in clinical practice when allowing for the evidence base and patient choice. Is it time to revise the standard?
INTRODUCTION
Quality audit comprises audit against standards, process change where standards have not been met and then re-audit. Closing the audit loop is an essential part of the quality improvement process.
During 2010, we audited our clinical practice against the auditable outcome measure in the 2007 British Association for Sexual Health and HIV (BASHH) guideline for the management of anogenital warts 1 that 90% of patients should be clear of original warts by three months. A retrospective case-notes review was undertaken for all patients attending with first episode genital warts between 1 January and 28 February 2010. 2 By case-note review alone (assuming that warts had cleared if patients stopped attending) 95% were clear of original warts by three months. However, by confirmed outcome (documented in case-notes or verified by telephone) only 81% were clear. Inconsistent attendance appeared to be the main reason for failure to clear. Subsequently all clinic staff agreed to emphasize at the first visit the paramount importance of consistent attendance and adherence to treatment in order to achieve prompt clearance of anogenital warts. A second audit was performed in 2011 to investigate whether clinical outcomes had improved.
METHODS
A second retrospective case-note review was undertaken for all patients attending with first episode genital warts attending between 1 January and 28 February 2011. Consistency with the clinical protocol for the treatment of anogenital warts was recorded. Patients were contacted by telephone on up to three occasions to confirm whether their original warts had cleared by three months.
Data were analysed in Excel. A two-tailed test of proportions was used to determine confidence intervals and P values. Significance was considered when the P value was 0.05 or less.
RESULTS
Wart clearance by case-note review and confirmed outcome for audit one and audit two
% = percentage clear by three months
Of the 89 where clinical outcome was confirmed, more men achieved wart clearance than women. Thirty-one out of 35 men (89%) achieved clearance at three months compared with 43/54 women (80%), but the difference was not significant (P = 0.27).
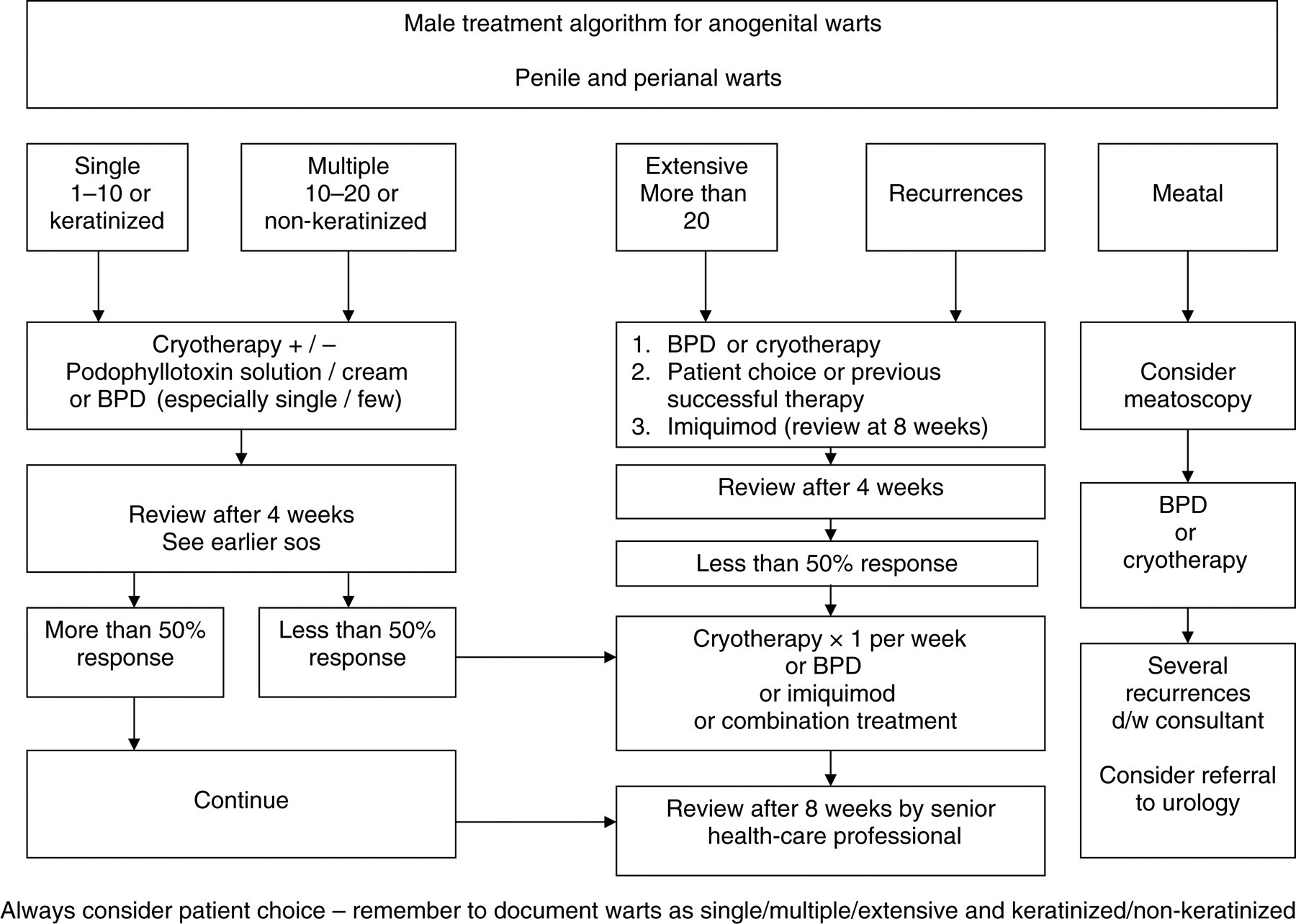
Overall 126/134 (94%) had treatment initially consistent with the clinical protocol for the management of anogenital warts. This included 71/74 (96%) who cleared their warts and 13/15 (87%) who did not (Figures 1 and 2). Initial protocol consistency was not associated with wart clearance (P = 0.15). Following the full treatment period, i.e. until wart clearance or until three months from first presentation, overall 108/134 (81%) adhered fully to the protocol, including 63/74 (85%) who cleared their warts versus 10/15 (67%) who did not (P = 0.09). The main reasons for non-adherence were lack of a clear documented follow-up plan and/or patients not attending for follow-up.
Female protocol for the treatment of anogenital warts BPD = bipolar diathermy Male protocol for the treatment of anogenital warts BPD = bipolar diathermy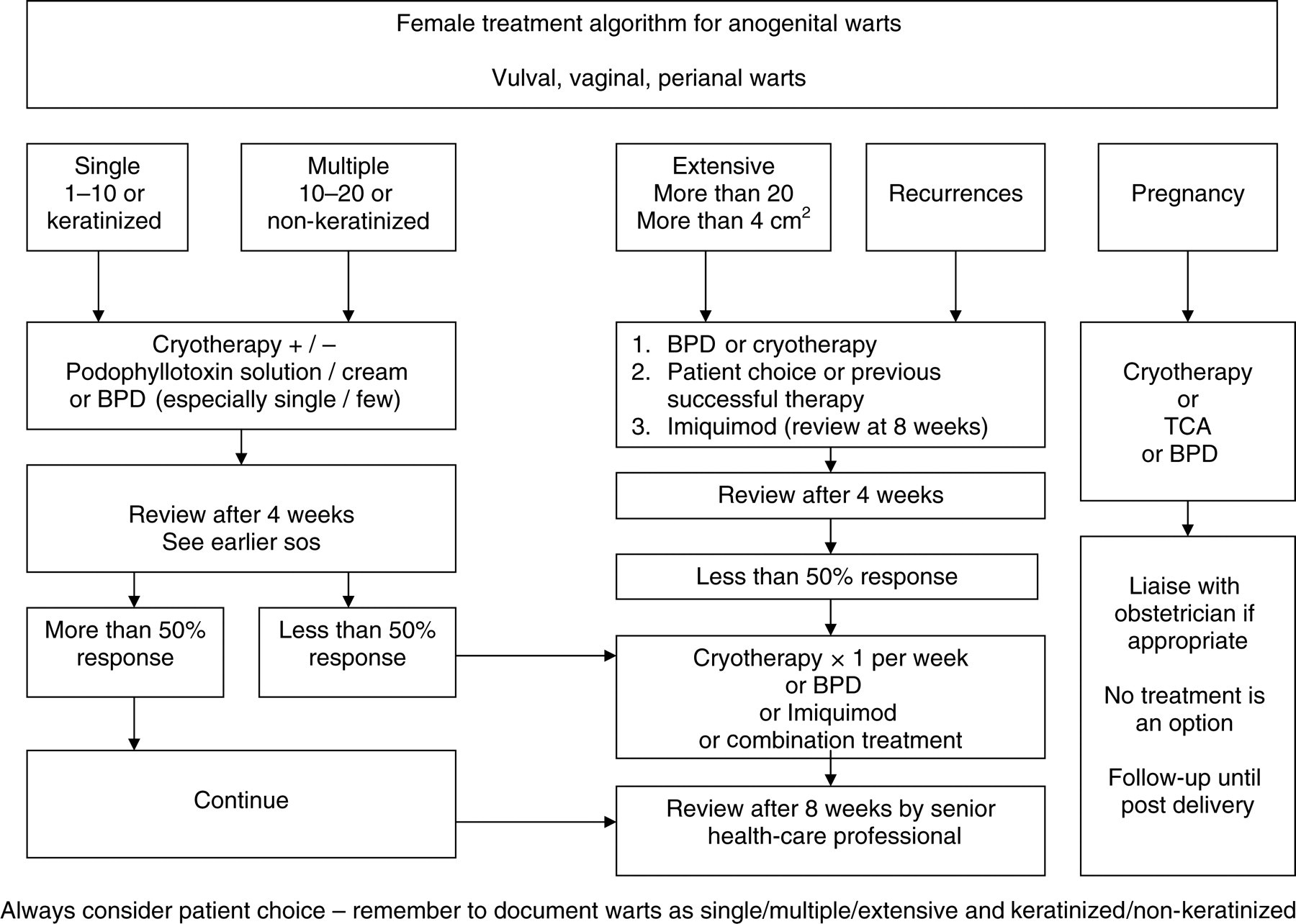
DISCUSSION
The two auditable outcome measures in the BASHH guideline for the management of anogenital warts
1
are as follows:
There should be 90% adherence to a local clinical protocol for the treatment of anogenital warts, and 90% of patients should be clear of original warts by three months.
The first outcome measure was achieved initially in audit two. It has been clearly demonstrated that the use of a clinical protocol significantly improves outcomes.
3
Initially, 94% had treatment consistent with the clinical protocol. Our protocol was reviewed after audit one (by presentation of the audit and discussion at a multidisciplinary team meeting). The protocol was found to be appropriate – in particular that first-line treatment allowed for staff to make recommendations and/or the patient to make choices regarding home treatment options dependent on the number and extent of the warts and the ease with which patients could reattend. Lack of availability of convenient appointments should not have been a barrier to reattendance – in addition to daily walk-in and all day appointments there are three evening clinics per week plus Saturday morning appointments, all with short waiting times.
The second outcome measure was not achieved in either audit one or audit two – results were 81% and 83%, respectively. In audit two, while outcome was confirmed in 89, only 37 (of which 81% had cleared) were confirmed by clinical assessment – the other 52 (85% cleared) were confirmed by telephone assessment. This is important because patients are more likely to underestimate than overestimate their wart burden. One paper 4 showed that at follow-up 30% of men and 44% of women still underestimated the extent of their warts. Also clinical assessment was able to distinguish between clearance and recurrence whereas telephone assessment was only able to determine whether the patient thought their warts had gone at three months and did not distinguish between persistence and recurrence.
Strengths of this paper are that it includes an audit and a re-audit of outcomes in clinical practice at three months. In both audits we made an attempt to contact everyone in whom the outcome was not known rather than making an assumption of clearance if patients were no longer attending. Audit one included a total of 101 patients and audit two included 134 patients. However, weaknesses must include the large number of patients we could not contact despite three attempts (37/101 and 45/134, respectively). There was no relationship between length of time from first visit and unanswered calls, although of course all calls were made at least three months from the first visit to allow for the outcome measure. There was also a similar level of unanswered calls in audit one when we were unable to contact 37/101 (37%) plus another 11 in whom no communication had been requested (total 48 [48%]). We called only the patient's mobile number – we did not call any land lines. Possibly patients had changed their numbers or did not have credit at the time we called. Although outcomes were confirmed in 53/101 and 89/134, respectively, this included telephone verification, which for reasons discussed before may not be entirely accurate.
There are several available treatments for anogenital warts and not one of these is clearly superior to the others. 5–9 Looking at the summary of clearance rates in the BASHH guideline, 1 only two treatment modalities have a range that actually reaches 90% clearance by three months namely cryotherapy (63–92%) and electrocautery/electrotherapy (78–91%). Podophyllotoxin is quoted as having a range of 34–77% and imiquimod 50–62%. The most recently published randomized controlled trial 4 showed clearance rates at three months of 60% with combination treatment and 45.7% for cryotherapy alone. A critical appraisal of the most commonly used treatments shows that most result in wart clearance between one and six months, 6 but recurrence rates are high. There are few data of outcomes in clinical practice at three months – the only audit 3 we could find showed clearance rates of 82% in women and 92% in men at three months, which is similar to our results. This is also consistent with the literature, as it has been shown previously that clearance rates for men are better than for women. 6
Auditable outcome measures need to be challenging yet achievable. However, it is difficult to judge precisely where the bar should be set. It is well recognized that standards set using expert opinion are unrealistic when compared with evidence of what is achievable. 10 It would be good to know if other clinics have been able to achieve the 90% standard in clinical practice. Perhaps 90% clearance at three months is not achievable in clinical practice when allowing for the evidence base and patient choice. Is it time to revise the standard? A suggestion might be 90% wart clearance in men and 80% in women at three months.