
Abstract
Sexual transmission of HIV-1, in the absence of co-factors, is poorly efficient. Data support that herpes simplex virus type-2 (HSV-2) may increase a woman's susceptibility to HIV-1. Potential mechanisms by which HSV-2 serves as an HIV-1 enhancing co-factor include (1) initiation of a clinical or subclinical mucosal inflammatory response, (2) alteration of innate mucosal immunity and (3) weakening or breaching the protective genital epithelia. No clinical trial has examined prevention of primary HSV-2 infection to eliminate the major morbidities of this recurrent disease and as a strategy to reduce HIV-1 transmission. Topical administration of potent antivirals can achieve local concentrations that are orders of magnitude higher than those obtained with oral administration. This paper reviews major advances in oral and topical pre-exposure prophylaxis of HIV-1 and HSV-2 and, based on these data, hypothesizes that simultaneous prevention of sexual acquisition of HSV-2 and HIV-1 via topical antiretroviral agents will have a synergistic impact on both epidemics.
Keywords
Herpes simplex virus type-2 (HSV-2) is the most common cause of genital ulcers and is the most prevalent viral sexually transmitted infection (STI) in the USA and worldwide. 1 Current USA data (2005–08) indicate that 16.2% of USA residents are seropositive for HSV-2; prevalence is significantly higher among women (20.9%), non-Hispanic blacks (39.2%) and persons age >20 years old. 1 Of those who are seropositive, 81% report they had not received a clinical diagnosis of HSV-2 from any health-care provider. 1 Therefore, most sexual transmission of HSV-2 occurs when the source partner has no clinically noticeable genital lesions. 2,3 As with other prevalent STIs, male-to-female transmission of HSV-2 is more efficient than the opposite. 4,5
Epidemiological data show a link between the prevalence of HSV-2 and HIV-1. 6,7 For example, HSV-2 seroprevalence ranges from 22% in sexually active adults in the USA to 60% of HIV-1-negative women in sub-Saharan Africa to more than 80% among people infected with HIV-1. 6,7
While HSV-2 infection appears to make a woman more susceptible to HIV-1, the opposite also appears to be true: HIV-1-positive women have impaired mucosal immunity to fend off an HSV-2 primary infection or re-activation. 8–10 Inherent anti-HSV activity of cervico-vaginal secretions is diminished in HIV-1-infected (HSV-2negative) women, as compared with healthy, HIV-1- and HSV-2-negative controls, independent of the presence of serum HSV antibodies. 10
HIV-1 and HSV-2 also appear to have a synergistic relationship on a host's viral shedding: HIV-1-infected women shed more HSV-2 virus and HSV-2 suppression also appears to decrease HIV-1 viral load in serum and HIV-1 RNA shedding in the genital tract.
8,11–13
In summary, HSV-2 and HIV-1 infections facilitate each other's acquisition, transmission and disease progression. This synergistic relationship is illustrated in Figure 1.
Inter-relationships between HIV-1 and HSV-2 infections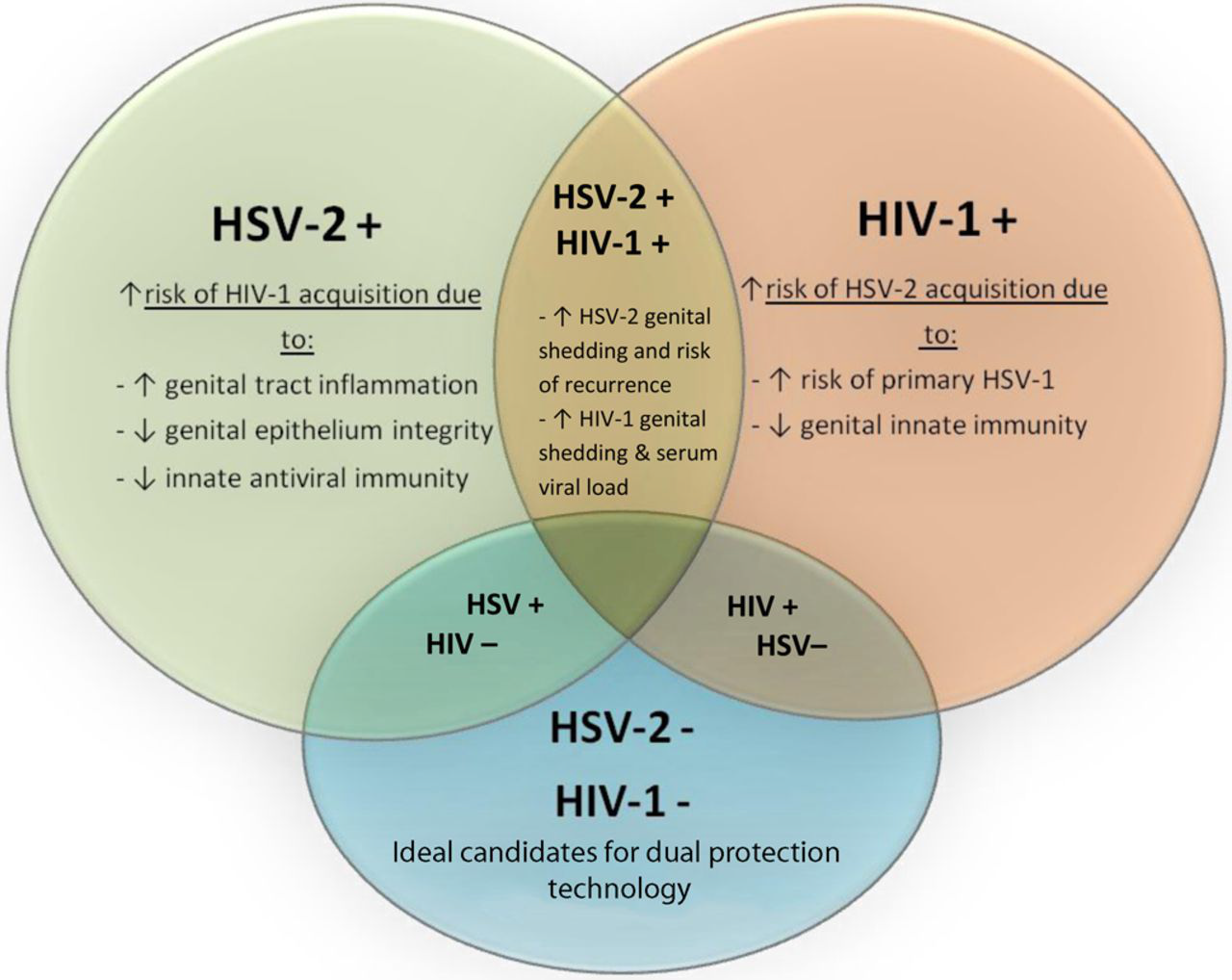
BIOLOGICAL MECHANISMS UNDERLYING THE ASSOCIATION BETWEEN HSV-2 AND HIV-1 ACQUISITION
The biological foundation of how HSV-2 increases a host's susceptibility to HIV-1 rests on several interacting mechanisms, the most obvious of which is frank disruption of the genital epithelium, which exposes intraepithelial and lamina propria HIV-1 target cells. 14 Additionally, the presence of HSV-2, even in the absence of genital ulcers, may recruit activated target cells for HIV-1, 8,15,16 alter innate mucosal immunity 10,17 and induce an inflammatory response. 18,19
HSV-2 infection increases the concentration of cervical HIV-1 target cells
Among HIV-1-uninfected female sex workers, the presence of HSV-2 infection was associated with a 10-fold increase in cervical CD4+ T cells expressing CCR5, considered to be the primary target of mucosal HIV-1 infection. 8 Women with HSV-2 also had a greater number of activated CD4+ T cells expressing CD69 and an increase in cervical immature dendritic cells expressing DC-SIGN in the cervico-vaginal mucosa. 8 There is an influx of dendritic cells and CD4+ and CD8+ T lymphocytes into recurrent HSV-2 ulcers. 15,16 These cells, which bear CCR5, CXCR4 and DC-SIGN receptors, persisted for months, even after lesion resolution and in the presence of antiviral therapy. Ex vivo infection of genital skin biopsies containing this inflammatory infiltrate supported three- to five-fold higher levels of localized HIV-1 replication than did skin biopsies from control areas that do not contain inflammatory infiltrates. 16
HSV-2 infection decreases mucosal innate immunity and induces a mucosal inflammatory response
Exposure to HSV-1 and HSV-2 in vitro causes a significant down-regulation of secretory leukoprotease inhibitor (SLPI) gene expression by human cervical epithelial cells, which persists even in the presence of the anti-HSV nucleoside analogue acyclovir (ACV). 17 This suggests that the virus uses down-regulation of SLPI as an immune evasion strategy. 17
SLPI has been shown to inhibit HIV-1 infection in vitro. 20 The reduction in SLPI concentration causes a subsequent up-regulation of nuclear transcription factor κB (NF-κB)-mediated proinflammatory pathways. 17 HSV-2 infection also directly activates NF-κB, which has been shown to induce HIV-1 replication. 18,19,21
In vitro experiments demonstrate that the cervico-vaginal secretions of HIV-1-negative women have inherent anti-HSV-2 activity. 10 This activity correlates with the concentration of soluble defensins, specifically human neutrophil polypeptides 1–3 (HNP 1–3). 10 Human cervical epithelial cells (CaSki) pretreated with SLPI were resistant to in vitro infection with HSV-2, even after washing. 10 CaSki cells pretreated with the cervico-vaginal fluid (CVF) lavages from healthy women were resistant to ex vivo HSV-2 infection, but the effect did not persist after washing. 10 It was hypothesized that the mechanisms of anti-HSV-2 activity of SLPI were different from those of HNP 1–3, with SLPI interacting directly with the target epithelial cell and HNP 1–3 interacting directly with the virus. 10 This group also demonstrated a reduction in HNP 1–3 in the cervico-vaginal secretions of women with HIV-1, compared with healthy, HIV-1-negative controls, further illustrating the adverse synergistic relationship between HIV-1 and HSV-2. 10
Depending on the Toll-like receptors (TLRs) and signal transduction pathways stimulated, innate antiviral responses at the cervico-vaginal mucosa may lead to potent antiviral defenses with little inflammation (type-1 response) or weaker antiviral defenses with greater inflammatory changes (type-2 response). 22 Upon infection, HSV-2 induces a complex array of innate and adaptive immune responses at the genital mucosal level. Induction of chemokines recruit activated CD4+ T cells and dendritic cells, which are targets for HIV-1 infection. 16,23,24 Proinflammatory mediators released by epithelial and immune cells facilitate HIV-1 replication. HSV-2 and other STI pathogens, as well as surrogate TLR ligands, induce HIV-1 replication directly acting on HIV-1 long-terminal repeat or, indirectly, via stimulated production of tumour necrosis factor α, interleukin (IL)-6, IL-8 and monocyte chemotactic potein-1 by primary epithelial cells. 25
The above evidence suggests that the HSV-2-positive woman's genital tract is more permissive to the establishment of HIV-1 infection. Based on these underlying mechanisms, many have hypothesized that suppression of HSV-2 recurrent infections would be an important HIV-1 prevention method.
CLINICAL STUDIES DESIGNED TO TREAT HSV-2 IN ORDER TO PREVENT HIV-1 ACQUISITION
Observational studies have shown a consistent association between HSV-2 seroprevalence and an increased risk of HIV-1 acquisition. 26,27 Among studies which documented HSV-2 prior to HIV-1 acquisition, HSV-2 was associated with a two-fold risk of acquiring HIV-1 (relative risk [RR] = 2.1 [1.4–3.2]). 26 This RR increased to 3.9 (95% confidence interval [CI] 3.1, 5.1) when the sequence of HSV-2 positivity and HIV-1 positivity was not known. 26 A second meta-analysis included additional subgroup analyses by gender and found that HSV-2-positive men were 2.7 times more likely to acquire HIV-1 (95% CI 1.9–3.9) and HSV-2-positive women were 3.1 times more likely to acquire HIV-1- than HSV-2-negative individuals (95% CI 1.7, 5.6). 27
RANDOMIZED CONTROLLED TRIALS
Despite strong observational evidence, three subsequent randomized controlled trials (RCTs) (the Tanzania study, the HIV Prevention Trials Network [HPTN] 039 study and an ACV prophylaxis trial in serodiscordant couples) found that daily oral ACV administration in HSV-2-positive women, 28,29 men who have sex with men (MSM) 28 and the HIV-1- and HSV-2-positive partner in an HIV-1–serodiscordant relationship 30 did not reduce the incidence of HIV-1. In the Tanzania trial, 821 women who were HIV-1 negative and HSV-2 positive were enrolled and randomized to twice-daily oral ACV (n = 400) versus placebo (n = 421), and followed every three months. 29 The incidence of HIV infection was 4.27/100 person years in both groups for a hazard ratio (HR) of 1.08 (0.64, 1.83). 29 Subset analysis showed that only a third of participants randomized to ACV had detectable ACV in their urine at the 12- and 24-months visits. 29
In the HPTN-039 trial, over 3000 HIV-1-negative, HSV-2-seropositive women in South Africa and MSM from sites in the USA and Latin America were enrolled and randomized to the same regimen of prophylactic oral ACV (n = 1581) versus placebo (n = 1591). 28 There were 75 HIV-1 seroconversions in the ACV group (3.9 per 100 person years) and 64 in the placebo group (3.3/100 person years) with an HR of 1.16 (0.83, 1.62). 28 There was a significant reduction in provider-observed genital ulcers in those individuals taking ACV. 28 Genital ulcers were reduced by 47% (RR = 0.53) and HSV-2 positive ulcers by 63% (RR = 0.37) in the ACV group (P < 0.001). 28 Compliance with medications, as assessed by patient report and pill counting was 94% in the ACV and placebo groups. 28
In a similar interventional trial, 3408 HIV-1 serodiscordant couples (where the HIV-1-positive partner was also HSV-2 positive) were randomized to prophylactic oral ACV, in the same dose as the Tanzanian and HPTN 039 trials, or placebo to the HIV-1-positive partner, in an attempt to reduce HIV-1 transmission to the naïve partner. 30 Prophylactic ACV reduced the mean plasma concentration of HIV-1 and the occurrence of HSV-2-positive genital ulcers, but did not significantly decrease transmission of HIV-1 to the seronegative partner (41 and 43 HIV-1 transmissions in the ACV and placebo groups, respectively, HR = 0.92, 95% CI 0.60, 1.41, P = 0.69). 30 Women accounted for 68% of new HIV-1 infections in this trial, reflecting the higher efficiency of male-to-female sexual transmission of HIV-1. 30,31
POSSIBLE EXPLANATIONS FOR THE LACK OF EFFICACY OF ORAL ACV TO PREVENT HIV-1 ACQUISITION IN THE RCTs
The answer to why observational data did not translate into effective interventional studies may be due to the following issues:
Drug availability and efficacy in preventing asymptomatic viral shedding
Oral ACV was used in the interventional trials because of its proven safety as a prophylactic agent, 32,33 widespread availability and low cost. An alternative drug, valaciclovir (VACV), was not chosen for the intervention trials because it was much more expensive and was not widely available in the test areas at the time of the studies. Oral VACV has potential advantages over ACV, including once-daily dosing, greater bioavailability and higher trough plasma levels. 2,4,34–36 Regarding protocol adherence, pill counting and participant self-report were the measurements for compliance in the HPTN 039. 28 The authors reported high protocol adherence by these endpoints. On the contrary, pharmacokinetic (PK) data from the Tanzanian trial suggested that compliance was poor. 29 Although varied studies suggest that compliance with once daily VACV dosing, compared with twice or more daily dosing of ACV, is increased (reviewed in 37 ), it is possible that missing a once-daily dose of a medication could result in lower systemic drug levels than missing one pill of a twice-daily-dosed medication. Moreover, large head-to-head studies show that VACV and ACV are equally effective in suppressing HSV viral shedding and recurrent lesions. 2,34–36 Unfortunately, it is known that despite available prophylactic regimens, release of HSV-2 from the neuronal reservoir still occurs with subsequent asymptomatic or symptomatic shedding of HSV-2. 2,4,38,39 Higher doses than standard suppressive therapy may also be needed. For example, recent data suggest that suppression of HSV-2 with high-dose VACV (1.5 g orally twice daily), as opposed to the standard suppressive therapy of ACV (400 mg orally twice daily), reduced plasma HIV-1 levels in patients dually infected with HIV-1 and HSV-2. 40 It is conceivable that if genital tract HSV shedding were further suppressed, prevention of HIV-1 infection would be improved. We speculate that increasing genital tract delivery of anti-HSV drugs will achieve this goal.
Plasma and vaginal levels of ACV are poorly correlated (r = 0.28, P > 0.05), with vaginal secretions containing 15–170% (mean 79%) of plasma ACV levels. 41,42 PK studies demonstrate that peak vaginal concentrations of ACV are reached 30–60 minutes after oral dosing. 42 Peak vaginal concentrations of ACV (0.8–3.6 nmols/g or 0.18–0.81 μg/mL) after daily oral dosing have been shown to be at or below the 50% inhibitory dose of ACV for HSV-2 (∼0.91 μg/mL). 43 Approximately one hour after oral dosing, vaginal secretion concentrations of ACV quickly decline. 42 Although no studies have investigated the use of current topical or oral ACV as primary prevention of HSV-2, based on the above tissue infectivity and PK data, it is hypothesized that increasing drug tissue levels above the 90% inhibitory dose (by higher or more frequent oral doses or by topical drug delivery) would be required to prevent primary infection by HSV-2 or to reduce recurrent genital epithelial replication and shedding. In addition, missed doses of oral ACV may significantly affect adequate genital concentrations of the drug, based on existing tissue PK data.
Study population
In the HPTN 039 trial, 26% of enrolled patients reported a genital ulcer in the past three months and only 9% had a genital ulcer on examination at enrollment. 28 In the Tanzanian study, genital ulceration and asymptomatic genital shedding of HSV-2 was very low (2% of participants had a genital ulcer at enrollment), which may indicate that enrolled participants had few recurrent outbreaks and a more latent disease course which may have diluted the preventive effect of ACV. 29 Generally patients with longstanding latent infections have less frequent clinical outbreaks. 44,45
Additionally, although a direct effect on HIV-1 replication was outside the purpose of the trials, it has been reported that phosphorylated ACV can inhibit HIV-1 reverse transcriptase in a cell-free system. 46–48 Further, activation (phosphorylation) of ACV by the HSV-dependent thymidine kinase only occurs within HSV-infected cells. 46,48 In order to have sufficient quantities of phosphorylated ACV to block HIV-1, there must be sufficient quantities of HSV thymidine kinase. 49,50 HSV-2 viral loads were not reported in any of the RCTs. However, infrequent genital ulceration seen in the RCTs may have been indicative of more latent disease course and lower HSV-2 viral loads, which in turn might not have provided sufficient quantities of this enzyme for ACV to have a direct effect on HIV-1 replication. 49,50
Theoretically, prevention of a primary HSV-2 infection, which typically is more symptomatic, has significantly higher viral loads and shows more robust changes in innate immunity and genital inflammation compared with recurrent activations would have had a larger impact on HIV-1 acquisition.
ACV prophylaxis may have prevented genital ulcers, but not the subclinical mucosal inflammatory reaction associated with them
This potential explanation is rooted in a commonly observed clinical phenomenon; even after frank genital ulcers resolve, symptoms such as pain and redness can persist. In the HPTN 039 trial, patients randomized to ACV had a significantly lower incidence of genital ulcers. 28 In the Tanzanian trial, only 15 incidences of genital ulcerations (6 in the placebo group and 9 in the ACV group; OR 1.69 [95% CI 0.61, 4.70]) were observed by providers at scheduled follow-up visits. 29 However, frank disruption of the epithelium may not be the only mechanism by which the genital mucosa becomes more susceptible to HIV-1 infection. The surrounding epithelium may have subclinical changes in inflammatory and innate immune response, leaving apparently normal epithelium still vulnerable to HIV-1 infection. In support of this, HSV-2 seropositivity in a small cohort of HIV-1 negative Kenyan female sex workers was associated with an increased concentration of cervical HIV-1 target cells even in the absence of genital HSV-2 ulcers. 8 Furthermore, sequential genital biopsies in HIV-1-negative, HSV-2-positive women (n=7) demonstrated a massive influx of CD4+ and CD8+ cells during episodes of genital ulcers, which persisted for months even after the epithelial lesion had healed. 15,16 Oral ACV therapy did not alter the persistence of these HIV-1 target cells. 15,16 Another group also demonstrated that CD4+ and CD8+ T lymphocytes persisted in the endocervix in between clinical episodes of HSV-2 and during asymptomatic and symptomatic HSV-2 shedding. 51 Thus, even in the absence of clinically noticeable HSV-2 lesions, alterations in innate mucosal immunity and inflammatory response, which likely exist to fend off further HSV-2 re-activations, appear to prime the genital tract for a productive HIV-1 infection. This suggests that in order to prevent increased susceptibility to HIV-1 infection, one would have to prevent primary HSV-2 infections and reduce or control HSV-2 epithelial replication and the subclinical changes in the genital mucosa associated with them during and in between recurrent episodes.
TOPICAL TREATMENT OF HERPETIC INFECTIONS
Currently, the Centers for Disease Control and Prevention (CDC) does not recommend topical treatments for HSV-2 lesions or recurrences, citing that these regimens are not as effective as oral or intravenous therapy. 52 Several trials in the 1980s investigating topical ACV ointment for the resolution of recurrent genital skin herpes ulcerations were disappointing, finding that topical ACV, in general, reduced viral shedding of HSV-2 in the lesions and reduced the time to complete crusting of lesions, but had minimal to no effect on the mean healing time of genital lesions, reducing inflammatory symptoms such as pain or preventing future recurrences, compared with placebo ointment. 53–56 Subsequently, it was thought that suboptimal treatment effect seen in these trials may have been due to poor penetration of ACV out of the ointment vehicle into the stratum corneum layer of the genital skin. 57 Later, improved efficacy of topical ACV in the treatment of genital HSV was shown with aqueous-based delivery vehicles, as compared with lipid-based vehicles. 58–60
PREVENTING HSV-2 AND HIV-1 INFECTIONS SIMULTANEOUSLY: NOVEL APPROACHES TO DUAL PROTECTION
The relevance of preventing HIV-1 infection is based on the devastating toll of this pandemic, which took the lives of 1.8 million people in 2009. 61 HSV-2 genital infection, albeit not lethal, is the most common STI in women and causes significant physical and psycho-social morbidity. 62 In addition, as stated above, it is a risk factor for HIV-1 infection. HSV infections have been the object of intense research; however, preventive options such as a vaccine remain elusive. 63
Results from the randomized, double-blind, placebo-controlled Centre for the AIDS Program of Research in South Africa (CAPRISA) 004 trial demonstrated that 1% tenofovir (TFV) vaginal gel, dosed in a pericoital, ‘BAT24’ regimen (within 12 hours before intercourse, repeated within 12 hours after intercourse, and no more than 2 doses in a 24-hour period), reduced the incidence of HIV-1 by 39% overall and 54% in high-adherence users. PK analysis indicates that topical TFV achieves higher genital tissue concentrations than oral TFV. 64 This proof of concept study has renewed interest in topical pre-exposure prophylaxis of HIV-1 and other STIs with the use of microbicides, especially those containing potent antivirals. 65 Unexpectedly, pericoital use of TFV gel also reduced the incidence of primary HSV-2 infection by 51%. 66 These findings need to be confirmed, as a treatment arm of a second large clinical trial, the Microbicide Trials Network (MTN) Study #003, the Vaginal and Oral Interventions to Control the Epidemic or VOICE trial, which used daily dosing of TFV vaginal gel, was discontinued for futility for HIV-1 prevention after a planned data safety monitoring board meeting in the fall of 2010. 67 No information has yet been released on the effect of daily TFV gel on HSV acquisition in VOICE trial participants. A confirmatory trial of the CAPRISA 004 study, using the BAT24 regimen, is currently underway (the FACTS 001 trial) in South Africa. 68
The clinical efficacy of TFV against HSV-2 observed in CAPRISA 004 trial may be explained by the high concentrations of TFV achieved in the CVF by topical administration of the gel (∼1 mg/mL), which have been shown in vitro and in vivo to be above TFV EC50 against HSV. 69,70 TFV 1% gel is currently being investigated for the topical prevention of both HIV and HSV genital infections and will likely constitute the first dual-protection technology to reach the market. In fact, data recently presented at the International AIDS Society (IAS) Conference in Rome (July 2011) found that topical TFV, in concentrations achieved in the CVF of women using TFV gel in the CAPRISA 004 trial, inhibited growth of HSV-1 and HSV-2 in primary human cell and tissue cultures. 71 Further, the active metabolite of TFV, TFV diphosphate, was detected in human epithelial and immune cells after incubation with TFV, and inhibited HSV DNA polymerase, linking it directly to inhibition of HSV replication and infection. 71
However, TFV concentration in CVF is a median derived from a range of values that extend below the EC50 of TFV. This means that many women in the CAPRISA trial had local TFV concentrations that were below TFV's in vitro effective concentration (around 150 μg/mL in cervical tissues). Furthermore, tissue concentrations of TFV are two orders of magnitude lower than those of seen in cervico-vaginal secretions (10 μg/mL). 72 It is likely that median epithelial concentrations of TFV are somewhere between those of the CVF (1 mg/mL) and those of the whole biopsied tissue (10 μg/mL), i.e. at or slightly above TFV in vitro EC50.
Based on PK data from oral and topical TFV administration, 64,69,70 topical delivery of ACV may achieve local concentrations that are orders of magnitude higher than its anti-HSV EC50. An approach being currently explored is the combination of TFV and ACV for topical delivery by a controlled-release device. 73 ACV is efficiently phosphorylated by HSV (and other herpes viruses)-dependent thymidine kinase in infected cells, and can also be phosphorylated in HSV-uninfected cells. 74 ACV is 400-2600 fold more potent than TFV against HSV-2. Therefore, on this basis alone, its combination with TFV should improve the reported anti-herpes activity and clinical effectiveness of TFV against HSV. 73 This hypothesis should be tested in a clinical trial of topical ACV to prevent HSV-2 acquisition in seronegative women.
Phosphorylated ACV, the active metabolite of ACV, also inhibits HIV-1 reverse transcriptase in a cell-free system. 46–48 As indicated, ACV is efficiently phosphorylated by herpes virus-dependent thymidine kinase. Phosphorylated ACV prodrugs have been designed which inhibit both viruses in infected and uninfected tissues. 46,48,50 These findings suggest the use of anti-HSV medications to reduce viral load in co-infected individuals who are not yet eligible for antiretroviral therapy. 40
Other dual protection products for the prevention of HSV-2 and HIV-1 are also in development, including a broad spectrum microbicide containing carrageenan and zinc. 75 In animal models, this product showed complete protection against RT-SHIV infection for up to eight hours after daily dosing for 14 days. 75 In vitro data suggest that zinc salts have activity against HIV-1 76 and HSV-2. 77,78
Finally, novel agents to provide dual protection against HSV-2 and HIV-1 and to expand protection against other STIs are being actively developed. 79 These novel agents include monoclonal antibodies against HIV-1 and HSV-2 envelope proteins. 79 In addition, alternative delivery forms including intravaginal rings, fast-dissolve tablets and films to be used vaginally are being investigated, both to reduce manufacturing costs, provide for discreet use by women and to offer women various dosage options. 79
CONCLUSIONS
In conclusion, data suggest that HSV-2 infection influences an HIV-1-negative host's susceptibility to HIV-1, but these observational data have not translated into effective treatments, as tested in RCTs. Failure of the RCTs may be due to a combination of factors including drug delivery and target tissue concentration, compliance with treatment and failure of the current regimens to normalize changes in cervicovaginal innate immunity and inflammatory response, which occur in HSV-2 infected individuals. Despite the failure of RCTs, the biological plausibility of how a highly prevalent, often asymptomatic and unreported infection such as HSV-2 can alter an individual's susceptibility to HIV-1 exists. In addition, combating HSV-2 infection to reduce its physical and psycho-social morbidity is an important goal on its own.
Although there are no current data to support that genitally applying ACV to HSV-2-negative individuals would prevent HSV-2 acquisition, it is hypothesized that topical application of ACV combined with TFV would be synergistic, and therefore more effective than TFV 1% gel in preventing HSV-2 acquisition. Based on the CAPRISA 004 study data, TFV gel, dosed pericoitally, significantly decreased HSV-2 acquisition. The FACTS 001 trial, which is underway, will be crucial to confirm the data from CAPRISA 004 study, particularly in light of the recent lack of effectiveness in preventing HIV-1 acquisition shown by the VOICE study, which dosed TFV gel daily, not pericoitally. Several new dual-protection technologies are under development. It is suggested that dual technology products such as a combination TFV/ACV vaginal gel or ring be tested as primary prevention products in HIV-1- and HSV-2-negative individuals, particularly those at high risk of infection. TFV 1% gel represents the most advanced of those products, constituting a possible new paradigm in primary, multipurpose prevention of STIs.
Footnotes
ACKNOWLEDGEMENTS
This review was supported by intramural CONRAD funds from the US Agency for International Development (Grant – GPO-A-00-08-00005-00) and the Bill and Melinda Gates Foundation (Grant 41266). The views expressed by the authors do not necessarily reflect those of the funding agencies. The authors thank the contribution of Alexandra Collado for performing literature searches and creating the diagram of Figure 1.