
Abstract
The southern African nation of Lesotho has an HIV seroprevalence of approximately 25%. To address the need for HIV care in rural Lesotho, a project called the Rural Health Initative (RHI) was launched in seven clinics in 2006. Data on enrolment were collected retrospectively and analysed for trends in gender enrolment over time. Of 6001 enrolled, 3904 were women (65.1%) and 2097 (34.9%) were men. When analysed by month of enrolment, there was a higher percentage of men enrolled in December compared with the other months of the year (χ2 = 15.98, P < 0.001). This may be due to the migratory work of the men in the mines of South Africa and suggests a need for targeted interventions to increase male enrolments over the entire calendar year.
INTRODUCTION
HIV is the most significant infectious killer of adults living in the world today 1 and the southern African Nation of Lesotho has a general HIV seroprevalence of 25%. 2 Access to antiretroviral therapy (ART) in Lesotho is limited and only one-third of those patients needing ART able to access it. 3
There are multiple factors that affect access to ART. One factor is gender, and multiple studies have shown that access to ART is not equal among the genders. 4–6 Given that women are often victims of gender discrimination, a larger literature has been devoted to access to ART among female populations. 7,8 In certain regions of the world, however – most notably southern Africa – a larger percentage of women are accessing HIV services compared with men. 9,10 There are multiple proposed reasons for this, including prevention of mother-to-child transmission as an entry point for women in HIV care, 11 stigma among men seeking health care (i.e. they are seen as ‘weak’ or ‘less manly’) 12–14 cultural beliefs 15 and work patterns. 16,17 This paper will explore trends over time disaggregated by gender in enrolment in an HIV programme in Lesotho between 1 June 2006 and 31 December 2008.
SETTING AND METHODS
Lesotho is a nation of 2.2 million people with a life-expectancy of less than 40 years of age. 18 Unemployment in Lesotho is high, and a majority of the men of productive age work in the mines of South Africa. 19 Gender distribution of the population is approximately equal: 48.7% men and 51.3% women as are rates of HIV. 20 ART coverage in the region in 2011 is estimated at 53% for women and 40% for men. 21 In June 2006, a collaborative programme known as the ‘Rural Health Initiative’ (RHI) was launched at seven rural primary care clinics. 22 Through the RHI, free HIV testing and treatment were offered to all clinic patients. Pregnant women were offered three-drug HIV treatment during their pregnancy and delivery regardless of CD4 count or clinical staging.
This paper is a retrospective review of patient enrolment from 1 June 2006 to 31 December 2008. At enrolment into HIV care, data were collected on date of enrolment, age and gender. Data were coded and analysed for gender differences in enrolment. These gender differences were also assessed by month of enrolment using chi-squared test of homogeneity of proportions to see if there were any changes over time. Age at enrolment data were assessed for normality using a skewness-kurtosis test, and gender differences in age at enrolment were assessed using Wilcoxon rank sum analysis. Analysis was conducted using Stata 11 (Statacorp, College Station, TX, USA). The study was approved by an ethics review committee in Maseru, Lesotho and by the human subjects committees at Harvard School of Public Health and Case Western Reserve University.
RESULTS
Six thousand and one patients were enrolled in HIV care through the RHI between 1 June 2006 and 31 December 2008. All patients had data on gender and date of enrolment. Of these 6001 patients, 3904 were women (65.1%) and 2097 (34.9%) were men. The gender distribution at enrolment was statistically significantly different from the census in 2006 in gender distribution in the country overall (48.7% men versus 51.3% women [P < 0.001]) and in the rural areas (49.4% men and 50.6% women [P < 0.001]). Five thousand four hundred and seventeen enrollees had reliable birth dates and mean and median ages were 36.7 and 35 years, respectively (SD 14.13; range <1–88 years). Median age at enrolment was significantly younger for women than men (34 versus 37 years, P < 0.001).
Trends in distribution of gender at enrolment over time were also assessed. A comparison was made between male enrolment in December (as a percentage of total enrolment) and all the other months of the year. For all three years combined, there was a higher percentage of men enrolled in December compared with the other months of the year (χ2 = 15.98, P < 0.001). When analysed by individual year, differences in proportions of December male enrollment versus the other months were statistically significant in 2007 (χ2 = 13.19, P < 0.001) and in 2008 (χ2 = 4.41, P = 0.036), but not in 2006 (χ2 = 2.15, P = 0.143).
Figure 1 shows male enrolment trends over time.
Percentage of men enrolled in HIV care by month of enrolment, 2006–2008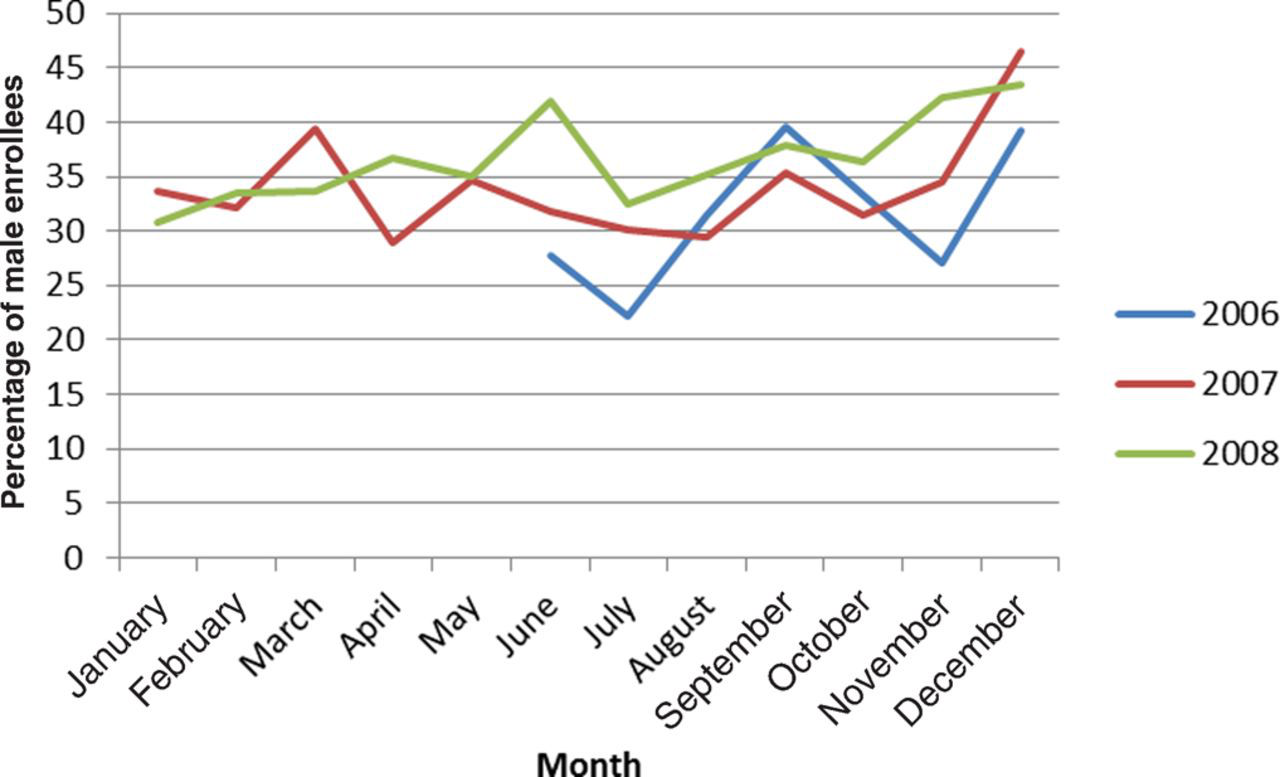
DISCUSSION
The data from this study in Lesotho show that women were more likely to be enrolled in HIV care programmes than men. The data also show that there is a significant difference in the gender distribution in December compared with other months of the year. There are multiple potential reasons for this gender gap. Women may be more likely to receive medical care as part of pregnancy or family services. 23 Stigma and cultural issues may also contribute to the gender differences seen here. 14 One potential contributor to the gender disparity may be the migratory work patterns of Basotho men. 24 Unemployment in Lesotho is high, and a majority of men from Lesotho migrate temporarily to South Africa to work in the mining industry. Work in this industry presents numerous health risks, and many of the men become infected and sick with HIV. 24 They usually return home from the mines in December for the Christmas holidays, 25 which may explain the significantly higher percentage of men enrolled in HIV care during this month.
This study has several limitations. It is a retrospective review of enrolment records. The population was not randomly selected and the conclusions may not be generalizable. There may have been historical changes that affected male enrolment. The analysis was not able to disaggregate by clinic as one-third of the data was without clinic identification; thus we were not able to control for any clinic level factors that may be contributing to observed trends. Furthermore, we were unable to control for any patient-level factors. There were no data collected on actual employment in the mines, as this work is often done illegally and clinics feared men would be reluctant to seek care if their work activities were documented. In spite of these limitations, this study suggests the need for outreach strategies among male populations in Lesotho and in South Africa. These strategies should involve public health authorities in both countries and take seasonal variation into account.
Footnotes
ACKNOWLEDGEMENTS
The authors of this paper are thankful to the many individuals and groups who assisted with the collection and analysis of this data, including the Clinton HIV/AIDS Initiative, Partners In Health and the Government of Lesotho. Funding was provided by Irish Aid, the Francois Xavier Bagnoud Center at the Harvard School of Public Health, Thomas J White and the Frank Hatch Scholars Program. Thanks are given to Megan Murray for her careful reading of this manuscript and helpful comments. The authors of this paper have no conflicts of interest to report.